MKCCG PLT Prescribing Workshop Thursday 25 th January

MKCCG PLT Prescribing Workshop Thursday 25 th January

CCG Update-General update PLT Thursday 25 th January Dr Nicola smith CCG Chair

CCG Update-Finance …… Ø Made good progress on “financial turnaround” and there has been a recent slowing down of elective care. Ø We are reasonably confident that we will end the financial year within budget Ø Thanks to practices who have worked on prescribing, managed routine referrals within acceptable levels and adhered to low priority restrictions + thresholds. Ø This is good for our local system as it means that we retain our autonomy and there are no additional requirements and conditions placed upon us by NHSE But… Ø Many of the strategies we have had to use are one-off initiatives which will not continue to reap benefits in future years. For example we have delayed investments in to service improvements that will not deliver savings in the current financial year. Ø Next year we have a “QIPP” savings target of £ 16 million. We know that the CCG has the capability to deliver around £ 8 million of savings so we know that we face significant reductions or restrictions to services unless we can make significant transformational changes to the system in which we work.


CCG Update-System transformation …… ØSTP wide Primary Care Transformation scheme ØPlace Based Accountable Care partnership for MK Ø CCG alignment

CCG Update-Flu…… Flu season not over Small percentage increase in uptake overall Uptake in children has improved Pregnant women still an issue Pharmacies now doing around 2 -3 % of patients which is small numbers but increasing Ø Need to check if all coding is correct so will give you the final position next time Ø Early review and planning for next year Ø Ø Ø

CCG Update-IFR …… You will have noticed a growing waiting time for IFR referrals (currently at around 12 -13 weeks) The CCG apologises for this totally unacceptable situation The CCG has had contractual discussions with the provider of the service to reduce the wait. Due to lack of improvement in the The CCG is now taking further action to urgently resolve the situation

CCG Update-Consultant to consultant referral policy review…. …… Aims • As with all referrals , those made by consultants should reflect good clinical practice and make appropriate use of resources in the health system. • Winning hearts and minds rather than contract challenges • GP workload should not be increased inappropriately as a result of our policy The easy bit……. • Consultants should always refer directly for anything urgent or 2 WW referrals • Consultants should refer to tertiary centres in cases where specialist expertise is required for the management of the clinical problem • Consultants should generally not refer patients for problems that are completely unrelated to the problem for which the patient has been referred. The grey area…. • Internal or onward referrals can be made, under certain circumstances , by consultants when the intervention of another speciality is required to manage the patient’s presenting problem. • If a patient is to be referred back to their GP , the consultant should not raise the patient’s expectation of a further referral. However, GPs sometimes appreciate advice from consultants regarding the next steps for the patient. Guidance on the grey area…. • A list has been created for common clinical pathways where this happens on a regular basis eg surgery to anaesthetics for pre-op assessment, rheumatology to orthopaedics for surgical intervention Monitoring • Clinical audit and volumes of referrals with a view to quality improvement , not punitive challenge mkccgimprove@nhs. net
 – Ravenscroft…… • Single point")
CCG Update-Integrated Community Musculoskeletal and Pain Management Service (IMSK) – Ravenscroft…… • Single point of access for musculoskeletal conditions (age 16+) via RMS • Clinically urgent (red flag) referrals excluded. Earlier this year, MKCCG and Ravenscroft conducted a MSK Enhanced Triage pilot, offering a ‘face to face’ assessment for all T&O referrals intended for the hospital. Over the course of the pilot, a significant number of patients benefitted from further rehabilitation or conservative management rather than experiencing long waits for consultant led appointments. As a result of these benefits for patients, the CCG has commissioned Ravenscroft to continue the enhanced triage service for Milton Keynes patients. In addition, if prior approval is needed as part of that onward referral, Ravenscroft will now complete the necessary paperwork - therefore, for the conditions below GPs will no longer need to complete the prior approval request paperwork as long as the referral is sent to Ravenscroft for an assessment. Bunions, Carpal Tunnel, Hip Replacement, Knee Replacement, Dupuytren’s Contracture, Ganglion, Hip Arthroscopy & FAI, Hip Resurfacing for Advanced Arthropathy, Knee Arthroscopy, Shoulder Arthroscopy, Therapeutic Injections. Epidural Injections for Lumbar Back Pain, Therapeutic Facet Joint Injections, Thermal radiofrequency denervation of lumbar & cervical facet joints, Trigger Finger

Questions? Contact Michelle Millard, MKCCG Patient Safety Coordinator: 01908 278 681 / mkccg. seriousincidents@nhs. net

Incidents and Serious Incidents • General Practice refers to internal incidents and/or occurrences outside of the ordinary which require some level of intervention as Significant Events. These are typically low harm and may require some changes and/or learning but are not usually systemic. These should be recorded internally and shared with MKCCGs Primary Care Manager quarterly. • Serious Incidents are defined as incidents occurring during NHS funded healthcare (including in the community), which result in one or more of the following: – Unexpected or avoidable death of one or more people. This includes suicide/self-inflicted death; and homicide by a person in receipt of mental health care within the recent past
 – Unexpected or avoidable injury to one or more people that")
Serious Incidents (SIs) – Unexpected or avoidable injury to one or more people that has resulted in serious harm – Unexpected or avoidable injury to one or more people that requires further treatment by a healthcare professional in order to prevent the death of the service user; or serious harm – Actual or alleged abuse; sexual abuse, physical or psychological ill-treatment, or acts of omission which constitute neglect, exploitation, financial or material abuse, discriminative and organisational abuse, self-neglect, domestic abuse, human trafficking and modern day slavery – A Never Event – all Never Events are defined as serious incidents although not all Never Events necessarily result in serious harm or death. See the recently updated Never Events Policy and Framework for the national definition (January 2018): https: //improvement. nhs. uk/resources/never-events-policy-and-framework/ – An incident (or series of incidents) that prevents, or threatens to prevent, an organisation’s ability to continue to deliver an acceptable quality of healthcare services
 Support • If in doubt, check it out: If unsure whether")
Serious Incident (SI) Support • If in doubt, check it out: If unsure whether an incident needs to be escalated as an (SI), please discuss with MKCCGs Patient Safety Coordinator • Specialist advise is also available within the CCG, e. g. around mental health, safeguarding, end of life, falls, etcetera • All patient safety related incidents (whether an SI or not), should be logged on the National Reporting and Learning System: https: //report. nrls. nhs. uk/nrlsreporting/ • Information Governance related incidents should be logged via the IG Toolkit. Support for Primary Care is available from the IG team: Telephone – 0121 611 0730; Email – igcentral@ardengemcsu. nhs. uk

Questions? Contact Michelle Millard, MKCCG Patient Safety Coordinator: 01908 278 681 / mkccg. seriousincidents@nhs. net

Milton Keynes in RED 60400 550 200 25800 7700 3300 1900 50 £ 459 K 70 £ 829 k 40 £ 502 K

CCG Update-Social Prescribing ……

CCG Update-And Finally…… Report any difficulties and ideas mkccgimprove@nhs. net March PLT – Blood borne viruses, MSK, Deputy Coroner May PLT – Suicide (planning afternoon and an evening session)

Polypharmacy and deprescribing Janet Corbett, Head of Prescribing and Medicines Management

Agenda 2. 20 pm Introduction and welcome 2. 25 pm Voting buttons quiz 2. 45 pm Prescribing and Deprescribing for frail elderly patients – Dr Than Mya 3 pm Tea break 3. 20 pm Principles and Practice of Prescribing and Deprescribing in Palliative Care - Dr Jane Wale 3. 50 pm Case study and round table discussion and feedback 4. 20 pm Tools available to support polypharmacy and deprescribing 4. 35 pm Round up and close

Learning Objectives • To understand appropriate and potentially inappropriate polypharmacy • To understand the definition of deprescribing • To be aware of the medico-legal issues relating to deprescribing • To be aware of tools that support deprescribing

What is deprescribing? Deprescribing is the process of withdrawal of an unnecessary or inappropriate medication, supervised by a healthcare professional (to distinguish from patient non-adherence) with the goal of managing polypharmacy and improving outcomes.

Polypharmacy and Deprescribing - Why is this important? There is very limited evidence on the safety and efficacy of medicines in older adults, particularly in the frail, who often have multiple comorbidities and functional impairments • Polypharmacy in older people is associated with decreased physical and social functioning; increased risk of falls, delirium and other geriatric syndromes, hospital admissions and death, and reduced adherence by patients to essential medicines • The HARMS Study demonstrated a clear correlation between the risk of hospital admission and the number of high risk medications prescribed • Elderly people often feel better after their medication is discontinued. In a clinical trial to reduce polypharmacy in older people, the patients' global assessment scale improved in 88% and in most patients cognitive function improved • Just because a specialist recommended starting two drugs last year doesn’t mean they are best-placed when it comes to stopping the drugs now …. This is usually, and appropriately, the clinical decision of the regular doctor with the general overview • Practices are tasked with identifying and managing moderate and severe frailty and undertaking medications reviews

Medico-legal issues Many prescribers are understandably concerned about potential medico-legal issues of deprescribing and where they stand if they stop a medicine for which there is an evidence-based guideline to use it. The European Journal of Hospital Pharmacy (a BMJ publication) explored the concept of clinical negligence and informed patient consent. The review concluded that the law presents no barriers to deprescribing if it is undertaken in partnership with the patient, supported by knowledge, skills and experience of both parties. In addition, in March 2015, a unanimous decision in the UK Supreme Court (Montgomery v Lanarkshire Health Board) made it clear that doctors must ensure their patients are aware of the risks of any treatments they offer as well as benefits and of the availability of any reasonable alternatives. In the right setting and at the right time, deprescribing provides a real opportunity to minimise side effects, drug interactions and pill burden through a patient centred conversation. Document agreements and goals


Quiz Emma Hooton Neighbourhood/In-house pharmacist

What proportion of over 75 s takes 4 or more medicines regularly? 1 - 17% 2 - 36% 3 - 40% 4 - 65% 82

What proportion of over 75 s takes 4 or more medicines regularly? 1 - 17% 2 - 36% 3 - 40% 4 - 65% 1% 9% 39% 51%

Answer: 36%

What is the average number of medicines per day taken by nursing home residents? 1 - Six 2 - Eight 3 - Twelve 4 - Sixteen 84

What is the average number of medicines per day taken by nursing home residents? 1 - Six 42% 45% 2 - Eight 3 - Twelve 4 - Sixteen 8% 5%

Answer: Eight

Which of these medicines is implicated in adverse drug reactions that can increase the risk of hospital admissions? 1 - NSAIDs 2 - Antidepressants 3 - Beta blockers 4 - Clopidogrel 5 - All of the above 84

Which of these medicines is implicated in adverse drug reactions that can increase the risk of hospital admissions? 1 - NSAIDs 26% 2 - Antidepressants 0% 3 - Beta blockers 1% 4 - Clopidogrel 0% 5 - All of the above 73%

Answer: All of the above

Which medicine, when taken long term, needs regular liver function tests and monitoring for pulmonary symptoms? 1 - Amoxicillin 2 - Nitrofurantoin 3 - Paracetamol 4 - Ticagrelor 83

Which medicine, when taken long term, needs regular liver function tests and monitoring for pulmonary symptoms? 1 - Amoxicillin 1% 2 - Nitrofurantoin 3 - Paracetamol 4 - Ticagrelor 61% 17% 20%

Answer: Nitrofurantoin

What does acute kidney injury cost the NHS each year? 1 - £ 10 m 2 - £ 100 m 3 - £ 400 m 4 - £ 620 m 82

What does acute kidney injury cost the NHS each year? 1 - £ 10 m 5% 30% 2 - £ 100 m 49% 3 - £ 400 m 4 - £ 620 m 16%

Answer: £ 620 m
 in an 80 year old")
What is the number needed to treat ( NNT) in an 80 year old on alendronate & calcium/vit. D to prevent a further hip fracture? 1 - 50 2 - 75 3 - 105 4 - 150 81
 in an 80 year old")
What is the number needed to treat ( NNT) in an 80 year old on alendronate & calcium/vit. D to prevent a further hip fracture? 1 - 50 21% 37% 2 - 75 3 - 105 4 - 150 23% 19%

Answer: 105

Drugs which have an anticholinergic effect can be very problematic in frail adults causing falls, declining cognitive function and tend towards increased mortality. What is the Anticholinergic burden score for solifenacin? 1: 0 2: 1 3: 2 4: 3 76

Drugs which have an anticholinergic effect can be very problematic in frail adults causing falls, declining cognitive function and tend towards increased mortality. What is the Anticholinergic burden score for solifenacin? 1: 0 2: 1 0% 14% 55% 3: 2 4: 3 30%

Answer: 3

Which medicine has Anticholinergic burden score of 1? 1 - Paracetamol 2 - Ranitidine 3 - Paroxetine 4 - Metformin 81

Which medicine has Anticholinergic burden score of 1? 1 - Paracetamol 26% 43% 2 - Ranitidine 25% 3 - Paroxetine 4 - Metformin 6%

Answer: Ranitidine

What was the mean age range of participants in trials for sulphonylureas, as first line/monotherapy for T 2 DM? 1 - 42 -54 2 - 55 -68 3 - 40 -60 4 - 65 -80 78

What was the mean age range of participants in trials for sulphonylureas, as first line/monotherapy for T 2 DM? 1 - 42 -54 38% 24% 2 - 55 -68 3 - 40 -60 4 - 65 -80 31% 6%

Answer: 55 -68

Which of these is not a medication review tool? 1 - The Larger Criteria 2 - The Beers Criteria 3 - STOPP-START 4 - NO TEARS 76

Which of these is not a medication review tool? 1 - The Larger Criteria 28% 30% 2 - The Beers Criteria 3 - STOPP-START 4 - NO TEARS 7% 36%

Answer: The Lager Criteria

Dr Than Dar Mya MBBS , MRCP Geriatrics , FRCP Consultant Physician MKUH

Background • Cohort • Cases • Process –care setting / correlation with number of prescribers

Case 1 /Prescribing cascade • 90 • PMH-Hypertension on Bendroflumethiazide 2. 5 mg, Felodipine MR 5 mg • -Recent RMCA infarct -Aspirin /Omeprazole /Atorvastatin • -COPD • - Recurrent Unexplained Syncopal Episodes (24 hour tape – high VEs burden on Beta-blocker –Bisoprolol 2. 5 mg • - Trial Levetiracetam 250 mg OD • Other Drug-Diltiazem 60 mg tds • -Zomorph 20 mg BD • ATSP -as unresponsive –hot, pale, floppy when stood up • Similar episode every time gets out of bed to mobilise with physiotherapy –significant postural drop
Bendroflumethiazide 2. 5 , Felodipine MR")
Medication review /PIP medication ? • • • 1)Bendroflumethiazide 2. 5 , Felodipine MR 5 mg 2)Bisoprolol 2, 5 mg od 3)Diltiazem 60 tds 4)Zomorph 20 BD 5)Aspirin , Omeprazole &Atorvastatin 6)Trial Levetricetam 250 mg OD • STOPP Criteria –Avid Combined Rate limiting CCB and Betablocker • -Adjust antihypertensive based on supine and postural BP • -Avoid long term opiates in recurrent fall •

Case 2 /Review medication once clinical status changed • • • 58 male – PMH -Bipolar Disorder on long term Lithium 800 -type 1 DM on Insulin -Recent NSTEMI –CABG Dual antiplatelet therapy Atorvastatin 80 ng OD -HF reduced LVSF LVEF 37 % (Ramipril 2. 5 mg OD Spironolactone 25 mg OD Frusemide 40 BD Bisoprolol 2. 5 mg OD

• Presented with atypical chest pain 4 week post CABG • Bloods –urea 12. 6 (6. 5), Creatinine 124 (64 ), EGFR 52 • Lithium 1. 45 (0. 6 -1. 2 mmol /l ) • Clinically dehydrated, Low systolic BP-100 mg, no evidence of fluid overload
Lithium 800 nocte 2)Dual antiplatelet therapy 3)Atorvastatin 80 mg OD")
Medication Review /PIP ? 1)Lithium 800 nocte 2)Dual antiplatelet therapy 3)Atorvastatin 80 mg OD 4)Bisoprolol 2. 5 mg OD 5)Ramipril 2. 5 mg OD 6)Spironolactone 25 mg OD 7)Frusemide 40 mg BD Review current valid indication and dose –with change in circumstances –new comorbidity –additional medication –biochemical profile –ADR/Interaction • ESC guideline practical guide on use of HF medication in patients with HF with reduced EF • •

Diuretics in HF • • • Relieve congestion –irrespective of EF Use minimum dose necessary –euvolaemia Adjust dose –volume status Monitor renal function Cr CL <30, Creatinine >221 -Thiazide

Prognostic Medication for HF reduced LVSF • Symptomatic & Survival, reduce Hospitalization. • ACEI first line EF<40% • MRA –EF <35 %despite BB&ACEI • Start low dose • Aim –highest tolerated dose – • Monitor renal function 1 -2/52 after initiation and titration – 4/12 ACEI • MRA –more close monitoring - • Trouble shooting • Some –abnormal – u&e • Acceptable -Creatinine 50% above baseline (266 umol/l) (Egfr <30 )--/K 5. 5 • Further rise Stop concomitant nephrotoxic drugs & reduce diuretics if not congested • Not resolved –half the dose recheck in one weekspecialist • Stop –Creatinine rise 100% >310 umol/l , Egfr <20
 • Mr A 66 -Metastatic")
Case 3 (potential future therapeutic benefit vs life expectancy) • Mr A 66 -Metastatic colonic cancer with peritoneal disease progression –palliative management -expected prognosis less than 12 months • PMH- NSTEMI more than 1 year ago • Medication –Dual Antiplatelet Therapy /Atorvastatin / Betablocker /Ramipril
Dual Antiplatelet (Aspirin and Clopidogrel ) 2)Atorvastatin")
Medication Review /Potentially Inappropriate Medication • • 1)Dual Antiplatelet (Aspirin and Clopidogrel ) 2)Atorvastatin 3)Bisoprolol 4) Ramipril • Life limiting disease prognosis less than 12 months – Statin • Dual Antiplatelet Therapy –unless recent NSTEMI –Coronary Artery Stent – risk of bleeding higher /no therapeutic advantage over single antiplatelet 12 months post event

Case 4 Medication –questionable efficacy without any evidence 78, lives alone with a cat PMH- Dementia -Heart failure with preserve LV Systolic function Ramipril 2. 5 mg Frusemide 40 BD Spironolactone 25 mg -Type 2 DM on Empagliflozin 10 mg Metformin 500 BD Presented as Advanced Dementia, poor oral intake, significant dehydration –AKI (Creatinine 344 (99) Urea 49. 3) • Not fluid overload • • •
Empagliflozin 10 mg • 2)Metformin 500 BD • 3)Frusemide 40 BD •")
• 1)Empagliflozin 10 mg • 2)Metformin 500 BD • 3)Frusemide 40 BD • 4)Ramipril 2. 5 mg • 5)Spironolactone 25 mg EBM –HFp. LVSF –no role of neuroendocrine antagonist (ACEI, ARB, Betablocker ) • Gliflozin –use not advised in Elderly & those with Cr Cl<60 • Renal function /Oral intake /Function –improveusual place of residence

Case 5 -underutilization of appropriate medication Potential Prescribing Omission • Mr C, Age 72 • Recurrent Embolic stroke PAF on Apixaban 2. 5 mg BD –Normal Cr cl, Age 72, Body weight 82 kg • Represented with Right sided weakness • MRI DWI –new left thalamic lacunar infarct • Medication review - ? Atorvastatin - ? Apixaban 2. 5 mg BD • BNF –stroke prevention in AF –Apixaban reduce dose to 2. 5 mg BD if Cr CL<30 ml/min and • Age >80 or Body weight , 60 KG • Under anticoagulation causing recurrent embolic stroke

Case 6 –Functional decline • 79 • PMH-Alzheimer's –Behavioural and Psychological symptoms on Risperidone 1 mg BD for 2/12 &Memantine 10 mg OD . -Type 2 DM on Metformin -Hypertension on Amlodipine • Transferred from Psych unit because of sepsis, reduce mobility and bilateral pressure sores • Sleepy most of the day, Not engaging with Physio –awaiting placement. • Medication review – 1)Memantine 10 mg • 2)Risperidone 1 mg BD • 3)Metformin 500 MG BD • 4)Amlodipine 5 mg od

Prescribing in Elderly -Unique challenges • Age related physiological changes in PK/PD • Unclear Evidence –outcome /appropriate dosage (trial excluded age group) • Time to benefit vs life expectancy • Frail, Multiple comorbidity & Poly pharmacy –risk of Adverse drug reaction/interaction –causing prescribing cascade • Commonly used drug for Geriatric patients –Poorly tolerated Anticholinergics /Analgesic –opiates, NSAIDS /Delirium – antipsychotic /Antidepressant • Prescribing cascade

• Drugs Problem –Inappropriate –Prescribed /Dosed /Monitored • Common-ADR event –Neuropsychiatric (over drowsiness /acute delirium, confusion ) • -AKI • -Fall with or without Injury • -Functional decline • -Syncope • Dose related –hip fracture study –psychotropic, hypnotic, anxiolytic, TCA, Neuroleptic, BP medication • Common cause dose related ADE –failure to dose adjust as per renal insufficiency (serum creatinine may not accurately reflect renal function –reduce muscle mass ) • 52% -Community –mild renal insufficiency – med require dose adjustment • Start – low dose –titrate up as tolerated (monitor SE /Biochem )

Prescribing Cascade • Treating ADR of previously prescribed medication • Further polypharmacy, further increase risk of ADR • eg 1)polypharmacy –fall and postural hypotension /confusion –treat as ? UTI /Sepsis 2) treating antipsychotic induced extrapyramidal –with antiparkinsonian medication • Suspect ADR –with any new clinical symptom unless proven otherwise • Minimise risk –Medication review • Review patient –PMH –Drug history

Potentially Inappropriate Prescribing • When pill burden>disease burden • Over prescribing –excessive dose-weight , biochemical profile -longer than intended duration -questionable efficacy (without valid indication ) -unfavourable risk-benefit trade off -without informed choice • Under prescribing - Not prescribing clinically indicated medication without any contraindication (potential prescribing omission )

Medication Review • BGS Recommendation –Annually • Actively seek Opportunity –to identify –those at risk PIP/those in need for specific medication –at every clinical encounter –in all setting • Overall responsibility –medication regime –GP • Aim –avoid –under and over prescribing /informed choice (pill burden and benefit vs risk), avoid flare up of LTC *minimise ADR , improve QOL • Targeted DE- prescribing -not denying effective treatment to eligible pts /about avoid ADR, simplify regimen, improve compliance &outcome • Target population • Process • Overall quality-appropriate poly pharmacy –good prescribing

Target population At risk of ADR, drug to drug interaction Multiple comorbidity and Poly pharmacy Frail ELDERLY Functional decline –house bound Cognitive dysfunction- compliance /side effect At risk of fall Limited life expectancy –prognostic medication –not be appropriate • High risk &Poorly Tolerated Medication /Medication with little or no benefit • Those on Long Term drug treatment-regular benefit vs harm assessment , as clinical needs and circumstances changes – • •
Comprehensive - both medical and drug history, • 2)Identify")
Medication review process • 1)Comprehensive - both medical and drug history, • 2)Identify –indication (preventative or symptom control) for each drug and check current valid indication –help target potentially inappropriate prescribing • 3)Access whether PIP can be stopped • 4)Plan withdrawal regime –reduce or stop one medication at a time (easier to identify the likely cause if problem develop ). • Some drugs need dose tapering –prevent withdrawal /allow monitoring –BB, opioids , barbiturates, antidepressant, gabapentin • 5)Monitor response ( benefit or harm) after each medicine has been stopped or tapered • (reappearance of pre-existing disease –no adverse consequence ) • 6)Involve patient /NOK –reach agreement –aim-optimize efficiency, minimise SE, improve QOL (informed choice ) • 7)Any potential prescribing Omission

Cautious stepwise withdrawal symptomatic decline if stopped • Medicines in this group may require specialist advice. • ACE inhibitors /Diuretics in heart failure (LVSD ) • Medicines for heart rate or rhythm control (beta-blockers; digoxin). • Opioids/antidepressants/ antipsychotics/anti epileptics/Parkinson’s Disease/clonidine/baclofen/ steroids/ benzodiazepines. Medicines for which specialist advice is strongly advised before altering include: • Medicines prescribed by specialist teams Anticonvulsants for epilepsy. Antidepressants initiated in secondary care. Antipsychotic and mood stabilising medicines (e. g. lithium). Medicines for the management of Parkinson’s Disease. Amiodarone. DMARDs.

Poorly Tolerated In frail Elderly /High drug burden index • Risk of functional decline • Anticholinergic /sedative /opiates(Analgesic and Incontinent Drugs ) – mobility cognitive decline-fall • BP pills –postural hypotension • Antipsychotic -atypical /conventional • Tricyclic

Avoid High-risk combined regime • medication 2 . NSAID + ACE inhibitor or ARB + diuretic [‘triple whammy’ combo] + e. GFR less than 60 ml/min + Diagnosis heart failure + Warfarin or new oral anticoagulants (NOACs) e. g. dabigatran, apixaban, rivaroxaban + Age > 75 without PPI • Warfarin with Macrolide, Quinolone, Metronidazole

Medicines and Dehydration • It may be indicated to WITHHOLD the following in patients diagnosed with severe dehydration • ACE inhibitors/(ARBs)/Diuretics • NSAIDs • Metformin These can then be restarted when the patient has improved (e. g. after 24 to 48 hours of eating and drinking normally).

Patients at risk of falling • Medication review should be considered as part of a multifactorial assessment in patients at risk of falling. • Medicines listed below associated with an increased risk of falls; • long-acting or long-term hypnotic or anxiolytic • Antihypertensive, beta-blockers Diuretics • Antidepressants • Antipsychotics, anti-epileptic medication (especially if used for pain) • First generation (sedating) antihistamines • Medicines used for Parkinson’s Disease (review in conjunction with specialist) • Anti-cholinergic medication used for bladder spasm or other medicines with anti-cholinergic side effects e. g. TCAs

Delirium /Challenging Behaviour • 90% of people with dementia experience behavioural and psychological symptoms, at some point. • Distressing symptoms can be prevented or managed without medication. • However, antipsychotic medications are frequently prescribed as a first resort. • Benefits of antipsychotic medications are limited over longer periods. • Retrospective study Dementia –new Antipsychotic Vs No – increase risk of death –at 30&180 days Antipsych group (AHR 1. 55 , CI-1. 15 -2. 07)

Specific consideration for patients with Dementia on Antipsychotic When to review dose/indication When not to stop antipsychotic • Dementia & been on antipsychotics for more than 3 months and have stable symptoms should be reviewed with a view to reducing/stopping antipsychotic medication. • Patients with co-morbid mental illness such as schizophrenia, persistent delusional disorder, psychotic depression or bipolar affective disorder. 2

Anticholinergics in Elderly • • Prescribe with caution Susceptible to SE Secreto –dry mouth /eye Motor –AROU /Constipation Sedation , Confusion , delirium , fall Cognitive decline Number &potency –Link –Mortality

Anticholinergic –Potency ranking scale • • • • • Antihistamine (H 1 /H 2 RA )–chlopheniramine, diphenhydramine , hydroxyzine -fexofenitidine, loratidine -Ranitidine Anti muscarinic –overactive bladder –oxybutynin, solifenacin, tolterodine, trospium Antimascarinic –antispasmodic –atropine, hyocine, glycopyrrolate Anti emetic –promethazine, hydroxyzine (antihstamine ) Antidiarrhoea –loperamide Psychotropic –conventional (chlopromazine, haloperidol ) -atypical –Risperidone, Quatiapine, Olanzapine Antidepressant -TCA –Amitriptyline, Trazodone -SSRI –Paroxetine -Mirtazapine Baclofen Benzodiazepine Opioid Analgesics Mirtazapine Not exhausted – increasing dose and simultaneous use - anticholinergic activity

Minimise use of anticholinergics • Consider anticholinergic burden scale. • Proactively monitor at regular intervals for efficacy and tolerance • If suspicion of anticholinergic induced impaired cognition, MMSE , consider switching or stopping if clinically appropriate • Refer patients suffering from significant anticholinergic side effects due to psychotropic medication to an appropriate specialist • Avoid prescribing anticholinergics with acetylcholinesterase inhibitors e. g. donepezil, rivastigmine

Avoid underutilization of Appropriate Prescribing • START criteria • 22 validated criteria to identify potential prescribing omission • Organ specific guidelines vs Overall benefit • Prioritize –active treatment of serious condition, > less impact on QOL – compliance /limit drug interaction • Indicated drugs –too need dosed /monitored appropriately

SUMMARY • Regular Review medical &drug history along with functional , cognitive , biochemical status • Reappraise with –change in clinical status /treatment goals • Ask –Current valid indication / is the dose appropriate • -What is intended benefit / -What is the potential harm • -Time to benefit vs life expectancy • -What dose patient want (best interest) • - Judge organ specific EBM vs overall clinical status • -Monitor –response /ADR • Watch out -Poorly tolerated –AKI prone /Anticholinergic /Drowsy. • High Risk combination /Duplication • -Mindful of prescribing cascade at any episode of deterioration • Avoid Potential Prescribing Omission
![References • Multimorbidity: clinical assessment and management NICE guideline [NG 56] September 2016 •](http://slidetodoc.com/presentation_image/016076bc54dce361ff90bbd67d542abe/image-92.jpg "References • Multimorbidity: clinical assessment and management NICE guideline [NG 56] September 2016 •")
References • Multimorbidity: clinical assessment and management NICE guideline [NG 56] September 2016 • Upto date -Drug prescribing for older adults Paula A Rochon, MD, MPH, FRCPC Section Editor: Kenneth E Schmader, MD Deputy Editor: Daniel J Sullivan, MD, MPH • Int J Clin Pharmacol Ther. STOPP (Screening Tool of Older Person's Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Gallagher P 1, Ryan C, Byrne S, Kennedy J, O'Mahony D • A Practical Guide for the Treatment of Symptomatic Heart Failure with Reduced Ejection Fraction (HFr. EF)Brent N Reed 1 and Carla A Sueta • Key Considerations for Prescribing in Frail Adults GIG CAMRU NHS Wales

Refreshment Break

Principles and Practice of Prescribing and Deprescribing in Palliative Care Dr Jane Wale Consultant Palliative Medicine 25. 1. 18

1. General principles of prescribing in Palliative Care 2. Prescribing and deprescribing in specific conditions in last 100 days of life 3. Symptom control in the last days/ hours of life

General principles of prescribing in Palliative Medicine 1. Assessment and attention to detail 2. Information / explanation 3. Management of the problem 4. Medication 5. Monitoring and reviewing

Assessment and attention to detail What is the problem? What is the impact of the problem on the patient and family? What does the patient think is causing the problem? What have they tried so far? What is the goal of treatment?

Information/ Explanation • Improves compliance • Sets realistic treatment goals • Provides reassurance

Management Non pharmacological management/ pharmacological management Breathlessness – breathing techniques/ fan/ relaxation / visualisation techniques Nausea – sea bands / acupuncture Pain – radiotherapy/ nerve blocks/ exercise Bowel obstruction- NG tube

Which one? What’s the lowest dose that will work? What’s the best way of giving it? Can 1 medicine do 2 things? What next? STARTING MEDICATION Am I sure that benefit>burden? Rescue medication Compliance Cost Which medicine can I reduce/stop? Any interactions/ allergies?

PRINCIPLES OF STOPPING MEDICATION IN PALLIATIVE PATIENTS

Any medicine causing problems? ? Two medicines doing same thing STOPPING MEDICATION Burden of taking medication >benefit? Reason for taking medication Harm of stopping ? Indication still there ? Prophylactic

Management of diabetes in last 100 days of life Goals of treatment Avoidance of hypoglycaemia, DKA, hyperosmolar hyperglycaemic state Avoidance of dehydration For the patient to be able to eat what she/he wants to eat Maintaining the empowerment of the individual patient in their diabetes management to the last possible stage Practical measures 1 - aim for pre meal glucose between 6 -15 mmol/l – see if oral agents can be stopped 2 - Match the regime to the meals 3 - simplify regime- may make sense to have more insulin rather than tablets and insulin (most oral agents can cause problems if patients not eating much ? Change to repaglinide) 4 - when appetite very poor or oral route lost convert to once daily insulin 5 - Minimise invasive blood glucose monitoring

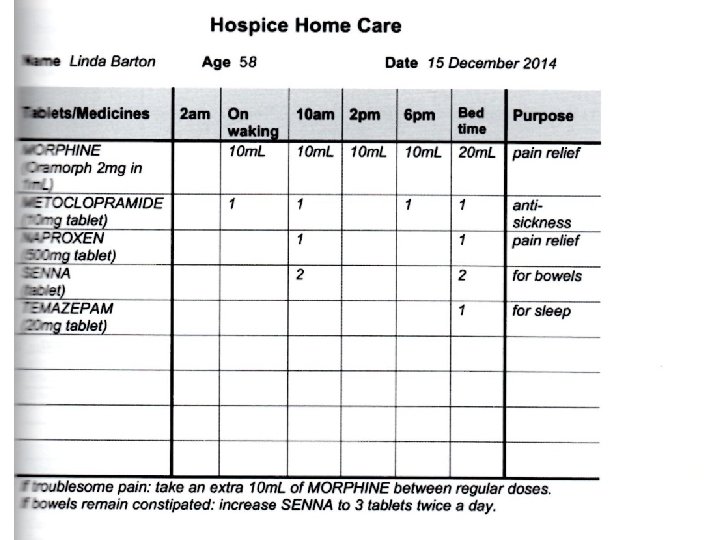
Management of COPD in last 100 days 1. Optimise current regime – unlikely to be able to use inhalers effectively – consider nebuliser 2. Non –pharmacological breathlessness management 3. Pharmacological breathlessness management:

Management of heart failure in last 100 days Goals of treatment To help symptoms – SOB, pain, cough, dry mouth, anorexia, constipation To reduce tablet burden To improve insight and understanding To plan ahead – switch off ICDs if appropriate

Medications that may need stopping Drug Rational for stopping Nitrates Very limited role in advanced heart failure Beta blockers Low HR, low pulse, cold extremities, fatigue ACEI Concurrent illness causing hypovolaemia ARB Concurrent illness causing hypovolaemia Mineral corticoid receptor antagonist High K, renal impairment Diuretic usually need to continue – can be given via a syringe driver

Management of chronic kidney disease in last 100 days Medication Advice Statins Stop when prognosis felt to be months Aspirin Stop early, unless vascular stent-when advice is to continue Vitamin D analogues Stop when prognosis felt to be months Anti hypertensive Loosen BP control- stop if tablet burden too high Phosphate binders Stop when oral intake poor Sodium bicarb Stop late – only when unable to swallow Diuretics Continue as long as possible

Symptom Treatment Breathlessness If fluid overload- diuretics Non pharmacological management Pain Paracetamol Avoid NSAIDs Tramadol 50 mg max bd or Oxynorm 2. 5 mg prn 8 -12 hourly S/C Alfentanyl / Fentanyl Could use buprenorphine or fentanyl patch if pain stable Try clonazepam 0. 5 mg if pain sounds neuropathic Nausea + vomiting Haloperidol 0. 5 mg or metoclopramide 5 mg tds Itch Chlorphenamine 4 mg /ondansetron 4 mg/pregabalin 25 mg nocte Agitation Haloperidol 0. 5 mg
 Anti HIV medication Anti convulsants")
What not to stop Diuretics Immunosuppressants (transplant patients) Anti HIV medication Anti convulsants

Last days- hours of life Anticipatory medication

Help and support for HCP • MK Palliative Care Advice Line • 24/7 • Palliative Medicine consultant on call 01908 306962 113

One more thing…. GSF= Gold Standard Framework = Good Supported Future

Good Supported Future I am on the GSF register I have an Advance Care Plan I have a treatment escalation plan I have a DNACPR form

One more thing….

Thank you Any questions?

Case study and Discussion • Over to you ………….
")
Consider… • The number and types of medicines being taken (appropriate and problematic polypharmacy) • Any changes to the benefit to risk profile for each medicine • Are all medicines fully optimised? • Individualised goal setting with Irene; what is important to her?

Consider… • Physiological changes that may affect drug metabolism and require dose/frequency adjustments • Individualising the interpretation of national guidelines for single, long-term conditions with Irene’s multimorbidity • Stopping medicines used for preventing chronic disease (time to reach benefit)
 burden • Adherence • Patients living with frailty suffer more")
Consider… • Pill (medicine) burden • Adherence • Patients living with frailty suffer more Adverse Drug Reactions (ADRs), drug: drug interactions and may have an exaggerated response to a minor stress, e. g. a simple infection or the addition of a new medicine

Rational Decision Making EFFICACY Benificence COST Justice SAFETY Non-malificence PATIENT FACTORS Patient autonomy From: What constitutes good prescribing? Barber N. BMJ 1995; 310: 923 - 925.

Tools available to support polypharmacy and deprescribing Some key questions 1. Is there a valid and current indication and is the dose appropriate? ? e. g. PPIs- use minimum dose to control GI symptoms - risk of c. difficile and fracture e. g. quinine use- see MHRA advice re safety e. g. long term antibiotics 2. Is the medicine preventing rapid symptomatic deterioration? Should usually be continued eg Meds for heart failure, Parkinson’s Disease 3. Is the medicine fulfilling an essential replacement function? If the medicine is serving a vital replacement function, it should continue eg levothyroxine 4. Is the medicine causing: - Any actual or potential ADRs Contra-indicated drug or high risk drugs group - strongly consider stopping Poorly tolerated in frail patients - consider stopping

Tools available to support polypharmacy and deprescribing Some key questions cont. 4. cont. Any actual or potentially serious drug interactions – consider stopping. Particular side effects? May need to consider stopping; don’t prescribe additional medicines to counter s/e 5. Consider drug effectiveness in this patient - refer to the ‘Drug Effectiveness Summary’ which estimates effectiveness. 6. Are the form of medicine and the dosing schedule appropriate? Is there a more cost effective alternative with no detriment to patient care? Is the medicine in a form that the patient can take supplied in the most appropriate way and the least burdensome dosing strategy? Is the patient prepared to take the medication? 7. Do you have the informed agreement of the patient/carer/welfare proxy? Once all the medicines have been through steps 1 to 6, decide with the patient/carer/or welfare proxies what medicines have an effect of sufficient magnitude to consider continuation and discontinue others.

Tools available to support polypharmacy and deprescribing The STOPP tool is a screening tool which can be used to identify potentially inappropriate prescribing for older people. See at http: //www. em-consulte. com/showarticlefile/245669/main. pdf • The Anticholinergic Cognitive Burden Scale was developed with UK Medicines Research Council is used to assess potential risk of anticholinergic side effects of commonly prescribed drugs. See http: //www. indydiscoverynetwork. org/Anticholinergic. Cognitive. Burden. Scale. html • • Poorly tolerated drugs in frail elderly Digoxin in doses of 187. 5 mcg daily or greater Benzodiazepines and z-drugs, particularly for long-term use Phenothiazines (e. g. prochlorperazine) Antipsychotics Tricyclic antidepressants (TCAs) Anticholinergics Opioids and gabapentin / pregabalin Combination analgesics (e. g. co-codamol)

Tools available to support polypharmacy and deprescribing Database of Treatment Effect This tool provides estimates of the effect of NICE recommended drugs, compared to placebo, on specific outcomes, in specific conditions. It is designed to inform discussions between patient and clinician when considering the benefits and harms of taking long term medication. Beers Criteria Lists high risk medicines and offers safer alternatives NO TEARS Helps to structure a medication review • Need and indication • Open questions • Tests and monitoring • Evidence and guidelines • Adverse events • Risk reduction or prevention • Simplification and switches • HARMS
")
Tools available to support polypharmacy and deprescribing High risk combinations Non-Steroidal Anti-inflammatory Drugs (NSAIDs) +ACEI or A 2 RA + diuretic (triple whammy) +e. GFR < 60 ml/min +Diagnosis heart failure +Warfarin or NOACs, e. g. dabigatran, rivaroxaban, apixaban +Age >75 without PPI Warfarin or NOAC +antiplatelet in frail patients – risk is high and combination should be challenged +NSAID +Macrolide and quinolone antibiotics (if concomitant use is essential, ensure appropriate INR monitoring) +Azole antifungals including miconazole oral gel (if essential, ensure appropriate INR monitoring) Heart Failure Diagnosis +glitazone +NSAID +tricyclic antidepressant The PINCER clinically important errors: 1. Patients with a history of peptic ulcer prescribed non-selective non-steroidal anti-inflammatory drugs (NSAIDs) without co-prescription of a proton-pump inhibitor 2. Patients with a history of asthma prescribed β blockers; 3. Patients > 75 years old prescribed angiotensin converting enzyme (ACE) inhibitors or loop diuretics without assessment of urea and electrolytes in the preceding 15 months.

NNT and NNH NNT NNH Helps assess benefits from drugs or interventions Estimates the number of patients who may suffer an adverse event from an intervention Estimates the number of patients that have to be treated for one to gain a particular benefit Inverse of absolute risk reduction so patients at higher risk usually have more to gain The higher the NNT, the more patients have to be treated for benefit Time frame for delivery of benefit must be considered Eg BP control Low risk patients NNT = 80 High risk patients (Diabetes, vascular disease) NNT = 32

Patient Decision Aids Used as part of a shared decision making process, encouraging active participation by patients in healthcare decisions e. g from NICE • Atrial fibrillation: medicines to help reduce your risk of a stroke – what are the options? • Statin to reduce the risk of coronary heart disease and stroke • Type 2 diabetes in adults: controlling your blood glucose by taking a second medicine – what are your options? eg from Chris Cates – NNT On line

Key Points • • No surprises, as the possibility of stopping the medicine should have been discussed with the patient before starting it Review all current medicines – on acute and repeat screens Identify any medicines to be stopped, substituted or reduced Plan a deprescribing regimen in partnership with your patient Frequent reviews and patient support GPs can safely deprescribe medications with patient agreement Doing so will decrease pill burden and improve patients quality of life

Next steps The PIS 2017 -18 was for GPs to review three patients aged over 75 years taking at least 9 oral medicines each Mixed bag – some done well but …. • • • Not all patients met the criteria for inclusion Not all columns completed i. e. NNT, ACB Score Some reviews had N/A or nothing to stop although patients were receiving high risk medicines To complete the PIS target, you are asked to: • Re-review patients with information from today • Have a practice meeting to feedback the information from today and re-challenge each other on your medication reviews • Submit a final practice report with a copy of minutes from your meeting • Submit the review sheets showing completed actions from the 3 medication reviews per GP to Nikki Woodhall by 31 st May 2018.

Final Thought …… “Active and healthy ageing is important for everyone. Focusing on frailty now creates a golden opportunity to enable more of us to age well while planning ahead, discussing what matters most and ensuring we get the right care and support, both now, and into the future". Professor Martin Vernon, National Clinical Director for Older People, NHS England
- Slides: 132