Mitral Valve Anatomyimportant Anatomic Relationship The functional components

 Posterior Annulus")

 SYSTOLE")

, congestive")










 8073+3 60 NYHA I-II NYHA III-IV 40 -")

 80 53% 60 40 Ef Ef 50 -60% EF<50% P-0.")
 Effective regurgitant orifice (ERO)")





![Posterior leaflet excision [carpentier] Posterior leaflet prolapse 2 to ruptured or elongated chordae.](https://slidetodoc.com/presentation_image_h2/73eee2762eb51456e1c3f8eda6606ad4/image-28.jpg "Posterior leaflet excision [carpentier] Posterior leaflet prolapse 2 to ruptured or elongated chordae.")


![Edge-Edge Technique [Alfieri] Innovative method for mitral valve repair. A running suture along](https://slidetodoc.com/presentation_image_h2/73eee2762eb51456e1c3f8eda6606ad4/image-31.jpg "Edge-Edge Technique [Alfieri] Innovative method for mitral valve repair. A running suture along")




- Slides: 35
Mitral Valve Anatomy-important Anatomic Relationship The functional components of the mitral valve apparatus include: Annulus Leaflets Chordae Papillary muscles LV wall Abnormality in any of these component will result in mitral regurgitation.
Anterior Annulus Anterior leaflet Anteromedial commissure Posterolateral commissure Posterior leaflet (3 lobes) Posterior Annulus SLIDE 3 - PICTURE FIGURE 1 Chordae tendinae Medial papillary muscle Lateral papillary Muscle MITRAL VALVE
Left main Coronary artery Intervalvular trigone Circumflex coronary artery Anterolateral papillary muscle Posterior leaflet Left coronary sinus Noncoronary sinus Anterior leaflet Secondary Chorda tendinea Posteromedial papillary muscle Primary chorda tendinea Tertiary chorda tendinea Coronary Sinus
DOG LV DIASTOLE OBSERVED Fiber Dimensions Calculated Spherical LV Model (`100 g) SYSTOLE
The left ventricular wall composed of muslce fibers, connective tissue, fat neurovascular structures and lymphatics
Photomontages assembled from electron micrographs of dog LV cells are from control (A), congestive heart failure due to mitral regurgitation (B), and recovery state after successful mitral valve surgery (C). Electron micrograph of adult LV canine myocardium. Long axes of several cells cross the figure from left to right. Arrows mark the location of boundaries between adjacent cells. Large open spaces are capillaries perfused with fixative.
Ephysilus Weave Myofibril Stranos Myocyte Capillary Tendon Struts Schematic illustration of substructure of the connective tissue matrix of the myocardium.
Systolic Torsion of LV Asymmetry of fiber radii, sarcomere length and electrical activation allows torsion of the apex relative to the base.
Base Endocardium Apex Epicardium Model for generation of torque for LV wall. Vectors force generation at the epicardial and endocardial surfaces could neutralize each other. The epicardial fibers at the epicardial surface have a longer radius and a more powerful moment arm. Sarcomere lengths, activation time, and infolding of the wall contribute to heterogencity of the relation between structure and function between the inner and outer regions of the wall. Differences in the total force generated are believed responsible for the LV systolic twist.
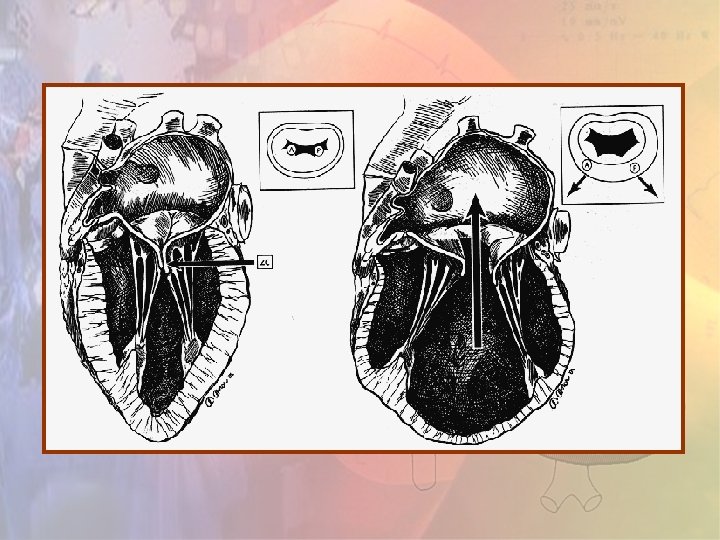
Mechanism of mitral regurgitation
Etiology of Mitral Regurgitation in Patients Undergoing Valve Repair
Pathophysiological Changes in Mitral Regurgitation Decrease left ventricular impedance Increase left ventricular end-diastolic volume Increase stroke work and afterload Decrese ejection fraction and increase left ventricular end-systolic dimension Myocardial fibrosis and end-stage cardiomyopathy
The Natural History of Mitral Regurgitation Mitral regurgitation is a progressive disease With an increase on average of 7. 5 ml/year for regurgitant volume and of 5. 9 mm 2/year for the effective regurgitant orifice. The progression of mitral regurge also cause progression of LV remodelling at the same rate.
Importantly, progression is not uniform, 10% of mitral regurgitation regress spontaneously The rate of reversal varies 6 weeks to 1 year
The Natural History of Severe Mitral Regurgitation High morbidity at 10 year: Atrial fibrilliation - 30% Heart Failure - 60% Sudden death at the rate of 1. 8% per year
Timing of Surgery What information is needed to define the timing of mitral surgery? Symptoms-Functional Class Impact of Pre-operqtive symptoms on survival after mitral surgery
100 - 90+2 76+5 Survival (%) 8073+3 60 NYHA I-II NYHA III-IV 40 - 48+4 20 - P<0. 0001 0 Years N 8 I-II 0 199 1 192 2 187 3 184 4 181 5 169 6 125 7 95 8 63 9 42 10 34 III-IV 279 249 236 227 211 201 174 183 103 74 51 Figure 1. Overall postoperative survival compared between patients in NYHA Class I/II and patients in Class III/IV – Numbers at bottom indicate patients at risk.
Left Ventricular Function Ejection Fraction Left ventricular and systolic dimension Assessed by echocardiography
100 75% Survival (%) 80 53% 60 40 Ef Ef 50 -60% EF<50% P-0. 0001 20 0 0 2 4 32% Years 6 8 10
Degree of mitral regurgitation-hymodynamics Regurgitant volume (R. Vol. ) Effective regurgitant orifice (ERO) Assessed by quantitative doppler echo The respective thresholds for severe mitral regurgitation are (R. Vol. ) > 60 ml. and ERO > 40 mm 2
Timing of Surgery Translate into_when the patient seen_promptly provided no major comonbidities The concept of waiting fro signs of early LV dysfunction is not advised
QUESTION: Should we advise follow-up with medical treatment?
ANSWER: NO, even if ejection fraction is low. Operative mortality is not excessive. Post operative complications are often delayed. The precision of the prediction of the outcome is imperfect.
Mitral Valve Surgery The optimal intervention for mitral surgery is valve repair. Superior hemodynamics and ventricular function. Less distortion of ventricular shape. Avoidance of prosthetic related complications. valve and Excellent long term clinical outcome.
Mitral Valve Repair Leaflet plication Mc. Goon Plication
Posterior leaflet excision [carpentier] Posterior leaflet prolapse 2 to ruptured or elongated chordae. Excise unsupported leaflet Posterior leaflet Ruptured chordae Repair annulus Repair leaflet Supported repair
Subvalvar apparatus inspection with a nerve hook. The middle portion of the leaflets is identified
The central stitch is used to check the symmetricity of the orifices.
Edge-Edge Technique [Alfieri] Innovative method for mitral valve repair. A running suture along the free edge of the leaflets is done.
Chordal Repair Anterior leaflet prolapse Excise unsupported leaflet Anterior leaflet Ruptured Chordae tendineae Mobilize apposing posterior leaflet Posterior leaflet Transfer supported posteior leaflet Attach posterior leaflet and repair annulus Completed repair
CONCLUSION: Mitral regurgitation is a surgical issue. Timing of mitral surgery still remained one of the most vexing problems of clinical cardiac science. The concept of waiting for signs of early LV dysfunction not exists anymore. The outlook is poor for patients who are treated medically.
Chronic severe Mitral regurgitation No symptoms Echocardiography Left Ventricular ejection Fraction >0. 60 and end-systolic Dimension <45 mm Left Ventricular ejection Fraction >0. 60 or end-systolic Dimension >45 mm Symptoms Echocardiography Mitral valve reparable Mitral valve not reparable Ejection fraction >0. 30 No atrial fibrillation or pulmonary hypertension Clinical and Echocardiographic Follow-up Ejection fraction >0. 30 Atrial fibrillation or pulmonary hypertension Mitral-valve surgery (valve repair preferred if technically feasible) Management of Chronic Severe Mitral Regurgitation Mitral-valve replacement
THANK YOU!!