Mission Parivar Vikas Improved access to contraceptive family


")








 at")





 & Centchroman(Chhaya) • Proposed Activity-: upto Sub Center")




![Compensation to Private/NGO B. futh fpfd. Rld] ljdkjh la. LFkku esa ljdkjh Vhe dh](https://slidetodoc.com/presentation_image/32e3753f9faeebcc413551383e529a43/image-25.jpg "Compensation to Private/NGO B. futh fpfd. Rld] ljdkjh la. LFkku esa ljdkjh Vhe dh")

 HFD district may organise Mission Parivar Vikas")










- Slides: 37
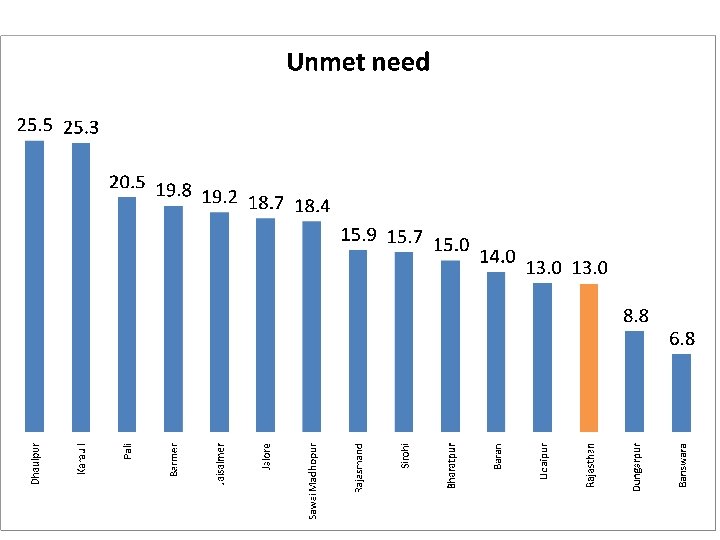
Mission Parivar Vikas Improved access to contraceptive & family planning services in high fertility districts District TFR Unmet Need Bharatpur 3 15. 0 Baran 3 14. 0 Pali 3. 1 20. 5 Sirohi 3. 1 15. 7 Jaisalmer 3. 2 19. 2 Rajasmand 3. 4 15. 9 Dungarpur 3. 5 8. 8 Jalor 3. 6 18. 7 Sawai Madhopur 3. 6 18. 4 Udaipur 3. 6 13. 0 Karauli 3. 7 25. 3 Banswara 3. 9 6. 8 Dhaulpur 4 25. 5 Barmer 4. 4 19. 8
Selection of District • High Fertility Districts in seven high focus states- UP, Bihar, Rajasthan, MP, Chattisgarh, Jharkand Assam. • Districts with TFR 3. 0 & above. • These districts constitute 28% of India population and contribute to 30% of maternal death and 50% of infant death. • Districts of Rajasthan are- – Bharatpur , Dhaulpur, Karauli, Sawai-Madhopur (Bharatpur Zone) – Udaipur, Dungarpur, Rajsamand, Banswara ( Udaipur Zone) – Jalore, Barmer, Jaiselmer, Pali, Sirohi (Jodhpur Zone) – Baran (Kota Zone)
(AHS 2012 -13)
21. 6 21. 2 Dhaulpur 21. 6 Karauli Sirohi Dungarpur Jalore Rajasmand Karauli S. Madhopur Jaisalmer Udaipur Barmer Bharatpur Baran Banswara Dhaulpur 33 38 Rajasmand 21. 6 Sawai Madhopur 21. 7 31 Banswara 21. 7 31 Barmer 21. 8 30 Baran 21. 9 29 Jaisalmer 22 29 Udaipur Median age at first live birth among women aged 15 -49 yrs 22. 1 28 Rajasthan 22. 1 26 Jalore 23 Pali 21 24 Bharatpur 22. 2 Pali 22. 4 Dungarpur Sirohi % of Girls Married under the age of 18 49 39 20. 8
26. 8 24. 9 24. 1 23. 9 23. 8 23 22. 7 Rajasthan Jaisalmer Sirohi Bharatpur Pali 26. 8 Baran Sawai Madhopur 27. 1 Karauli 27. 1 Rajasmand 27. 4 Jalore 28. 6 Dungarpur 28. 8 Dhaulpur 30 Udaipur Banswara Barmer 31. 8 Crude Birth Rate
ai w 63. 8 er Bharatpur Sawai Madhopur Baran 36 rm r 37 Ba pu ai 62. 8 Ud 61. 4 lo re Live births taking place before an interval of 36 months (%) 37. 9 Rajasmand Jaisalmer 40. 1 Ja i ul 60. 7 ra r Pali 41. 4 Ka pu ho 59. 7 ad M ur lp 59. 5 au Karauli 42 Sa a 43. 3 Dh ar w 59. 1 ns Dungarpur 44. 4 Ba r tp u 58. 5 ra Dhaulpur 44. 9 Bh a d an m 57. 8 ja s Sirohi 44. 9 Ra an th as 56. 7 Ra j 56. 3 Banswara Rajasthan 45 li r Udaipur 45 Pa pu ar 54. 4 ng er lm n Jalore Barmer 48. 6 Du isa Ja ra 51. 2 Ba Si ro hi 50. 6 Women reporting birth of 2 and above (%) 33. 3 65. 3 66. 6
6 Rajasmand 15 Jaisalmer 16 Banswara 18 Dungarpur Jalore 37 Pali Barmer Udaipur 66 Sawai Madhopur 72 Sirohi Baran 89 Bharatpur 97 Dhaulpur Karauli Failure in Sterilization cases in No’s 2015 -16 83 64 49 29 2
er lm isa 83. 7 Ja 82. 5 Jaisalmer Rajasmand Dungarpur 4509 ur er 77. 2 rm Sirohi 4626 Ba re lo Dhaulpur 5126 Ja 70. 8 oh i Sawai Madhopur 5970 Sir r pu Baran Karauli 6522 ai Ud pu r ad ho a ar ns w 7166 Dh au lp M ai w 70. 4 Sa Banswara 7878 Ba ul i % of Sterilization on 3 and above 75. 2 74. 5 73. 4 68. 4 ra 9397 Ka 60. 1 li Barmer Jalore Pali 9754 Pa pu r ar ng d 60 Du an m 59. 5 as pu r Bharatpur Udaipur 10229 Ra j n 59 Bh ar at ra Ba th an as Ra j 15261 Average Sterilization of last 3 years Sterilization Performance 10126 3705 2848 88. 8 92. 2
ra Ka ul i ad ho pu r Ba ns w ar Du a ng ar pu r Dh au lp ur Bh ar at pu r M ai w Sa d an r pu ai oh i Sir m as Ra j n ra ha n st ja Ud Ra Ba li re lo Ja Pa er rm Ba 368. 32 er 296. 92 lm 254. 20 228. 48 201. 66 200. 29 289. 16 391. 22 503. 05 171. 87 isa 200. 00 356. 86 91. 72 164. 49 100. 00 174. 88 0. 00 17. 45 Ja 600. 00 Population Density 500. 00 400. 00 300. 00
Difference between HFD District and Others Indicators Population High TFR 14 districts Non High TFR 32 districts 2, 33, 58, 905 4, 51, 89, 532 Rajasthan 6, 85, 48, 437 % population 34. 1 65. 9 Area (Jaisemer- 146424. 0 195815 342239 Population Density 159. 5 230. 8 200. 3 TFR 3. 5 2. 7 2. 9 IMR (AHS 2012 -13) 60. 8 52. 3 55 Family Planning Practices( Modern Method) 57. 5 64. 3 62. 4 Unmet Need 16. 9 13. 5 13 CBR 26. 6 22. 7 24. 1 21. 7 22. 0 21. 3 40. 3 44. 5 42. 1 29. 3 45 Child Sex Ratio (0 -6 years) 2011 893. 8 885. 8 888 Total Literacy rate 2011 61. 8 67. 3 66. 1 Median age at first live birth among wome aged 15 -49 yrs Median age at first live birth among wome aged 25 -49 yrs Live births taking place after an interval of 36 months (%) Women reporting birth of 2 and above (%) 21. 9 21. 2 41. 5
Strategies Delivering assured services. Building additional capacity / HRD for enhanced service delivery. Ensuring commodity security. Implementing new Promotional Schemes Creating enabling environment
Delivering assured services • Roll • • • out of Injectable Contraceptive DMPA(Antara) at one go upto sub center level. Augmentation of PPIUCD Services to all delivery points. Augmentation of Sterilization services through HFD compensation scheme. Condom Boxes at strategic locations ( like health facilities, gram panchayat bhawan, etc) Social Marketing of condoms and pills. Mission Parivar Vikas Campaign (4 per year)
Building additional capacity / HRD for enhanced service delivery. • Service providers will be trained upto sub center level for injectables. • Service providers would be trained for PPIUCD/ IUCD (30% MO / 70% Nurse). • Streamlining of non performing service providers. • Accreditation with private service provider
Ensuring commodity security. MIS to be opeartionalized to track the supplies & consumption to different facilities (e-Saadhan). A designated FP logistic manager to be placed at State level.
Promotional Schemes Saas Bahu Sammelan Local Radio Spots with messages from local actors. * Parivar Vikash Shivir at Panchayat Samiti Level *Parvar Vikash Sangosthi at Village level through MMU & MMV
Creating enabling environment Advocacy and Inter-sectoral Convergence to reduce TFR for a healthy mother and child. State Level-: Meeting under CM with State HFMs, local MPs/ MLA, PS(HFW) with DMs/ Collectors and CMHOs of HFD and stake holders. District Level-: Meeting under DM with CMHO and BCMO / BDO and line functionaries. Block Level-: Meeting under BCMO / BDO with all MO’s, Nurse , Sarpanch , Patwaries, NYK Volunteers and National Service Scheme Volunteers.
Expected Outcome Number of Sterilization: 10% TFR Decline- points/year annual increase in each district. TFR >=4 : decline by 0. 3 Number of IUCD insertions: 10% TFR 4. 0 -3. 5 : decline by 0. 2 annual increase in each district PPIUCD acceptance rate TFR 3. 5 -3 : decline by 0. 1 <10% : 25% annual increase 10 to 20% : 15% annual increase >20% : 10% annual increase
Roll out of Injectable Contraceptive (Antara) & Centchroman(Chhaya) • Proposed Activity-: upto Sub Center Level – Identification and training of doctors and Staff Nurses, ANM – Onsite and whole site orientation of staff on new contraceptives – Commodity supply to these facilities with trained staff – IEC & BCC activity by district IEC cell and ASHAs after orientation – Service Provision for new contraceptive choices. • Financial Package-: – Post Training follow up Incentivizing ASHA’s @ Rs. 100/dose/ASHA Incentivizing beneficiary @ Rs. 100/dose received Incentive to be proposed from 2017 -18 PIP and for training budget to be utilized from 2016 -17 PIP
PPIUCD Services Proposed Activity-: at all delivery points Identification and training of doctors and Staff Nurses, ANM for PPIUCD services and ensure their empannelment. Availability of PPIUCD & IUCD service delivery and follow up register. Quality protocols to be followed as per Go. I guidelines. • Extension of PPIUCD incentive scheme to include incentive for beneficiaries – Rs. 300 may be paid to the acceptor of PPIUCD to cover their incidental cost and the travel cost for two follow up visits
Augmentation of Sterilization Services through HFD Compensation Scheme jktdh; la. LFkkvksa ij gksus okyh ulc. Unh ij ns; jkf’k Øal- enokj fooj. k efgyk ulc. Unh izloksÙkj iq: "k ulc. Unh efgyk ulc. Unh ¼izlo ds rqj. Ur ckn ; k izloksijk. Ur 7 fnu ds Hkhrj½ 1 2 3 4 5 ulc. Unh dslst dks ns; {kfriwfr. Z jkf’k ulcanh izsjd dks Mªx , . M Msªflax ds fy; s ulcanh vk. Wijs’ku djus okys lt. Zu dks , us. LFksf. VLV@, us. LFksfl; k lgk; d ¼MO½ ¼If any½ 2000 : 300 : 150 : 3000 : 400 : 100 : 325 : 75 : 3000 : 400 : 50 : 400 : & 6 7 efgyk fpfd. Rld dks ul. Z@, y, poh@, , u, e dks ¼bues ls ftldh M~; w. Vh lt. Zu vf. Ll. Vs. UV ds : i esa yxkb. Z xb. Z gks ½ 50 : 40 : & 50 : & 40 : 8 vks. Vh VSDuhf’k; u ; k v. U; led{k LVk. WQ 21 : 27 : 21 : Conti…
Øal- enokj fooj. k efgyk ulc. Unh iq: "k ulc. Unh izloksÙkj efgyk ulc. Unh ¼izlo ds rqj. Ur ckn ; k izloksijk. Ur 7 fnu ds Hkhrj½ 9 10 12 13 14 ysc Vs. Duhf’k; u@ysc Vs. Duhf’k; u miy. C/k u gksus dh f. LFkfr esa ysc Vs. Duhf’k; u dk dk; Z djus okyk v. U; rduhdh LVk. WQ lt. Zu Vhe dks ykus ys tkus okys ljdkjh okgu ds pkyd dks r. Fkk LVsf. Vd ls. UVj tgka ij ogha dh lt. Zu Vhe ulcanh vk. Wijs’ku djrh g. S ftlesa okgu pkyd dk dksb. Z dk; Z ugha gksrk g. S vr% okgu pkyd dks ns; jkf’k vk. Wijs’ku esa lgk; d v. U; ok. MZck. W; dks nh tk ldrh g. SA ulc. Unh f’kfoj esa jft. LVªs’ku @ulc. Unh vk. Wijs’ku ls l. Ecf. U/kr le. Lr Qke. Z Hkjus , oa vko’; d fjdk. MZ la/kkfjr djus okyk lkaf[; dh deh. Z ; k v. U; dkfe. Zd dks fjÝs’kes. UV ¼ulc. Unh djkus vk; s dslst] v. Vs. Ms. UV o lk. Fk vk; s c. PPkksa ds fy, nw/k] pk; ] fc. Ldq. V vkfn dh O; o. LFkk djus ds fy; s ds. Ei izca/ku@fofo/k O; ; ds fy; s dqy jkf’k 19 : 23 : 19 : 7: & 7: 23 : & 23 : 20 : & 20 : 2800 : & 4000 : 20 : 4000 :
Compensation to Private/NGO A. futh v. Lirky@, uthvks dh Vhe ifjokj d. Y; k. k ds v. Urx. Zr ulcanh lsok, sa ljdkjh la. LFkkuksa esa tkdj nsrs g. S] rks blds rgr fu. Euafdr ns; gksxh%& Tubectomy (Interval and Post Abortion) Post-Partum Sterilization Vasectomy Acceptor ¼ ulcanh dsl½ 2000 3000 Motivator/ASHA ¼ izsjd½ 300 400 Clerk/ Documentation ¼ f’kfoj@la. LFkk ij fjdk. MZ la/kkfjr djus okys dkfe. Zd½ 30 0 30 1170 600 70 3500 4000 3500 Private Provider Total yk. Hkk. Fkh. Z ds Pre Operative Examination, Operation, Post Operative Care, Camp Management dh iw. k. Z tokcnsgh lacaf/kr futh la. LFkku dh gksxh r. Fkk yk. Hkk. Fkh. Z ds {kfriqfr. Z jkf’k ds Hkqxrku dh iq. k. Z tokcnkgh lacaf/kr ljdkjh fpfd. Rlk la. LFkku gh gksxh. A
Compensation to Private/NGO B. futh fpfd. Rld] ljdkjh la. LFkku esa ljdkjh Vhe dh lgk; rk ls ulcanh vk. Wijs’ku djus dh lsok, sa iznku djuk pkgrs gks. A blds rgr fu. Eukafdr izfriwfr. Z jkf’k ns; gksxh%& Tubectomy (Interval and Post Abortion) Post-Partum Sterilization Vasectomy Only Sterilization Surgery 200 325 400 Local Anaesthesia/Anaesthetist 50 75 0 Total 250 400 C. iathd`r futh fpfd. Rlk la. LFkku@x. Sj ljdkjh lax. Bu }kjk Lo; a dh la. LFkk ij ulcanh vk. Wijs’ku djus ij ns; izfriwfr. Z jkf’k%& Tubectomy (Interval and Post Abortion) Post-Partum Sterilization Vasectomy Facility ¼ la. LFkk ½ 2500 3000 2500 Client ¼ yk. Hkk. Fkh. Z ½ 1000 3500 4000 3500 Total
Condom Boxes at Strategic Locations in Health Facilities Coverage: - The scheme will be applicable for 14 High Fertility Districts (Both Rural and Urban areas) (Bharatpur, Dhaulpur, Karauli, Sawai Madhopur, Udaipur, Dungarpur, Rajsamand, Banswara, Jalore, Barmer, Jaiselmer, Pali, Sirohi, Baran ) Key Activities: - • Meeting of the Districts / block authorities / Health Volunteers / Local Leaders to Identify places for placing condoms boxes. • Introducing Condom Boxes at strategic locations. Number of Condom boxes may vary from facility to facility based on the strategic locations in the facility demand eligible couple catered by the facility. • Condom boxes should be made from the available resources. • Each condom box in the facility to be mandatorily tagged and should be given a Unique number (For eg: Condom Box-1; Condom Box-2 etc. ) • Replenishment System: Each condom box to be replenishment at least monthly or as soon as warranted based on the consumption. Condom boxes should be replenishment by “Free Supply”
Mission Parivar Vikas’ Campaigns: (4 Per Year) HFD district may organise Mission Parivar Vikas Compaigns in April, July, October and January (11 th to 25 th of the designated months). In July and October the activity will be clubbed with WPD and Vasectomy Fortnight. For April and January the activity is proposed to be divided into-7 days- Services delivery. Coverage: The Scheme will be applicable for All 14 HFD (Both Rural and Urban areas) (Bharatpur, Dhaulpur, Karauli, Sawai Madhopur, Udaipur, Dungarpur, Rajsamand, Banswara, Jalore, Barmer, Jaiselmer, Pali, Sirohi, Baran ) In urban areas the incentive may be given to Link Workers or equivalent working in urban areas.
Key Activity: State and District Level Activities State level meeting-At least one meeting before commencement for the fornight and subsequent meeting following completion of each round to review service delivery data monitoring feedback and any other issue and plan for the next round. District level meeting at least one meeting within two days of state meeting to review progress in planning and implementation State to provide technical guidance, including funding and operational guidelines and fix guidelines for district to plan and implement service delivery rounds which will further guide blocks. Ensure involvement of other relevant departments including ICDS, PRI and key family planning partners, RMNCH+A lead partners and other organizations at state and district levels. Civil society organizations (CSo) including professional bodies such as Indian medical association (IMA) and FOGSI may be involved. Ensure identification of nodal officer for urban area in each district. he/she will facilitate micro planning for in urban areas of the district. State to ensure to adequate number of IEC material (as per prototypes) and updated planning and reporting formats are printed and disseminated to district in time. ensure that these materials are printed and in local languages if necessary. Deploy senior state level health officials to high TFR districts for monitoring and ensuring accountability framework. State to track district adherence to timelines, including micro planning indenting of FP logistics and review each round of mission parivar vikas campaign and guide corrective actions. State/ district to ensure availability of required family planning commodities. District to track block and urban areas for adherence to timelines including micro planning, indenting
Promotional Schemes. . Parivar Vikash Shivir Objective- Create awareness and sensitization on family planning methods and to promote the benefits of small family norm Justification-The Health shivir had proved to be successful not only in disseminating information on family welfare and population issues, but also in providing actual services to people who otherwise had limited access to health facilities. Venue-: Health Institution at Panchayat Samiti HQ. Total 122 Panchayat Samiti in High Fertility District.
Ø Activities-: • Distribution of Family Planning Contraceptives. • Counseling on family planning methods. • Health Checkup & Follow up • IUCD Insertion Camp. • Talk Show, Quiz, • Slogan Competition for Secondary & Higher Secondary Classes. Ø IEC • Posters & Banners on various methods under Family Planning Program. • Specific Poster on Postpartum Family Planning Services & Injectables • Balika Sambhal Yojna • Beti Bacchao Yojna (Save the girl child). • Compensation & Incentive Package. • Age of Marriage & Spacing between births • Audio-Video(short films) of all Health programmes. • Folk Show
Parivar Vikash Sangosthi Objective- Create awareness and sensitization on family planning methods and to promote the benefits of small family norm Justification- Parivar Vikash Sangosthi will be clubbed with Medical Mobile Units(MMU) The for disseminating information on family welfare and population issues and also in providing health services to people who otherwise had limited access to health facilities. Venue-: As per the schedule of MMU in 16250 villages.
Ø Activities-: Distribution of Family Planning Contraceptives. Counseling on family planning methods. Health Checkup & Follow up IUCD Insertion Camp. Talk Show, Quiz, Slogan Competition for Secondary & Higher Secondary Classes. Ø IEC Posters & Banners on various methods under Family Planning Program. Specific Poster on Postpartum Family Planning Services & Injectables Balika Sambhal Yojna Beti Bacchao Yojna (Save the girl child). Compensation & Incentive Package. Age of Marriage & Spacing between births Audio-Video(short films) of all Health programmes. Folk Show
Saas Bahu Sammelan is aimed to facilitate improved communication between mother-in-law and daughter-in-law through interactive games and exercises and building on their experience it can be scaled up for other states so as to bring about changes in their attitudes and beliefs about reproductive and sexual health. Fund Flow: The funds for the scheme would be sourced from NHM Flexipool and routed through State PIPs. The budget may be proposed in NHM state PIP from 2017 -18 onwards. Districts to estimate the cost per sub centre ( Rs. 15000/Smmelan) and release the same to sub centre. Sub centre ANM will further utilize this fund to organize the Smmelan along with ASHA The expenditure details will be maintained by ANM in Sub Centre, Which should further be verified regularly by PHC/Block account officer in the Same manner as the other NHM Funds The Expenditure details should be regularly audited. S. No. Activity Name Financial Package: 1 Incentive to ASHA to mobilize Saas Bahu for the Smmelan 2 Organization of Sammelan 3 Token Gifts for Participants (Max. Rs. 20/- Participants Total Cost @ 1 Meeting 100 500 1000 (as per actuals ) 1600 Cost per Sammelan: Rs. 600/Meeting ( Rs. 1500/- for Organizing Smmelan and tokan gifts
Key Activity ANM to develop a microplan for Saas bahu Sammelan in each village in the format below: S. No. Name of the Population Village ASHA of Village Date/Day of Tentative Sammellan Number of Participans The Above micro plan should be updated regularly ASHA to prepare list of eligible couples and mother-in-law in their area. ASHA , AWW to motivate Saas Bahu pairs to come for the event. A minimum of 10 Saas Bahu Pairs should be present for the sammellan involving marginaized sections of the village. ANM to support ASHA and AWW for the same and be a part of these Sammellan. This can be done on rotational basis so that all the village/Sammellan of her catchment area are covered in a year. Identify champion mother-in-law who have provided support to her Bahus for using family planning methods Invite Gram Panchayat Members/Community influential for the event. Plan the event with games, communication exercises and other activity.
STRATEGIC ACTION 3: ENSURING COMMODITY SECURITY A management information system to be operationalized to track the supplies and consumption to different facilities. A designated FP logistics manager should be placed at state level in all the 7 HFS FUND FLOW: The funds for the schemes woul be sourced from NHM flexipool and routed through the state PIPs. The budget may be proposed in NHM State PIP from 2017 -18 onwards. STRATEGIC ACTION 4: CAPACITY BUILDING FUND FLOW: The funds for training for new contraceptive would be sourced NHM flexipool and routed through the state PIPs. STRATEGIC ACTION 5: CREATING ENABLING ENVIORNMENT : Advocacy and inter-sectoral convergence to reduce TFR for a healthy mother and child: State level (at lest 1) meeting under CM with state HFM, local MPs/MLAs, ps (HFW) with DMs collectors and CMOs of HFD and stake holders. District level (bi annually) : meeting under with DM and CMO and BMOs/ BDOs, and line functionaries and other stake holders working in districts. Block level (Quaterly): meeting under BMO/ BDO with all MOs, nurses and surpanch & patwaris Nehru Yuvak Kendra volunteers and national service Schemes Volunteers. FUND FLOW: The funds for training for new contraceptive would be sourced NHM flexipool and routed through the state PIPs. The budget may be proposed in NHM State PIP from 2017 -18 onwards.
District Program Implementation Body-: List of members (DHS can be the main body of District Program Implementation Body with addition of few members, if required) District Collector Principle Medical Office Districts Programme Manager District IEC officer District ASHA Coordinator Chief Medical and Health Officer Add/Dy. Chief Medical and Health Officer (FW) Districts Account Manager District Store Manager Periodicity of Meeting: Monthly or Sooner as required Terms of Reference : Assess progress of Implementation Mission Parivar Vikas at district. Address any challenge in implementation and take corrective actions. Review the demand generation activities in the districts and impact on FP uptake. Review any adverse event report and adverse media publicity and take remedial actions for same. Review the service provision in the identified Facilities and develop plan to enhance service delivery in these facilities. Ensure the availability of providers in the identified facilities for each type of FP services. Ensure implementation of Training plan as per suggestive strategy and follow up. Review the findings of monitoring visit shared by Development Partners and take corrective actions. Take immediate corrective actions to ensure supply of commodities and fulfill any logistic requirement. Submit implementation status and progress report to SPIB on monthly basis. Review the audit reports of the activities under Mission Parivar Vikas .
Block level Activities: Orientation of frontline workers/ANMs/LHVs/health supervisors-to be conducted by block medical officer. the participants would be health workers ANMs/LHVs health supervisors etc. ) and social mobilizers (ASHAs, AWWs and link workers) ASHAs to be Oriented on eligible couple survey for estimation of beneficiaries and will be expected to conduct this survey in their assigned area, and if required. Outside their area as well. Financial support will be provided for conducting this exercise @ Rs 150/ASHA/round. Service delivery during Parivar Vikas Abhiyan Fixed day services for family planning to be organized in high delivery case load facilities with sufficient infrastructure. Extensive mobilization for FP services at least 5 days prior to the service delivery activity. Team of doctors may be from medical college, district hospitals SDH, CHC private facilities or NGO/ Trust . In case the district does not have service providers the same can be mobilized from nearby district. FP provision providing all range of FP services. TA/DA to doctor per day for these service fornight Rs. 1000/-( the amount is in addition to the compensation scheme) (subject to performance of minimum number of 10 cases/day/provider) In addition to above sub centers to be activated for provision of IUCD services.