Mild Therapeutic Resuscitative Hypothermia Edward M Omron MD










 • Coagulopathy (impaired coagulation cascade and")






- Slides: 19
Mild Therapeutic Resuscitative Hypothermia Edward M. Omron MD, MPH Critical Care Service
Introduction • Improving outcomes from sudden cardiac death is a healthcare and only 0 -30% survive to discharge. • Mild resuscitative therapeutic hypothermia with basic neuro-critical care interventions may improve neurologic outcomes in survivors of cardiac arrest. • Basic neuro-critical care interventions – – – – Airway Protection (Intubation and Mechanical Ventilation) MAP >70 Hg or Cerebral Perfusion Pressure > 60 mm Hg Treatment of cerebral edema if present PCO 2 arterial 30 -35 mm Hg (not hyperventilation) GI and DVT prophylaxis Treatment of hyperglycemia (Glucose > 150 mg/d. L) Head of Bed to 30 degrees at all times
How does cooling work? • During cardiac arrest maintenance of cerebral perfusion and oxygen delivery is critical to neurologic outcome. • Hypothermia influences the entire cascade of destruction from ischemia, reperfusion injury, and cerebral edema • reduction in cerebral metabolism • reduction in vascular permeability and cerebral edema • reduction in immune response and inflammation
Clinical Studies • Two prospective, randomized clinical trials published in 2002, compared mild hypothermia (32 – 24 Celsius) with normothermia in comatose survivors of out of hospital cardiac arrest. • Both studies demonstrated a decreased likelihood of death and improved neurologic recovery with hypothermia and basic neuro-critical care interventions.
How to Cool • Different cooling techniques are combined for optimal patient cooling. • Induction cooling is accomplished initially with ice-chilled crystalloid infusion and ice packs followed by a cooling blanket system. • Endovascular Cooling with Surface Cooling: – Initially, 10 – 30 ml/kg ice-cold (4 degrees Celsius) crystalloid solutions (Lactated Ringer’s or Normal Saline) over 30 minutes – Cooling apparatus (Blanketrol III) with the water temperature set to 93 degrees Fahrenheit (33 degrees Celsius).
Timing and Depth of Cooling • Cooling should be initiated after return of spontaneous circulation. The 2005 AHA ACLS guidelines recommend cooling patients to 32 -34 Celsius for 12 - 24 hours. • Place rectal, esophogeal probe or Foley catheter thermistor in the patient and connect to machine. • Desired core temperature is 93 degrees Fahrenheit (33 – 33. 5 degrees Celsius) within 4 hrs of presentation to the intensive care unit (goal is within 2 hrs). • Maintain a core temperature of 93 degrees Fahrenheit (33 – 33. 5 degrees Celsius) for 18 hrs.
Cooling Monitoring • Shivering which prevents achieving the target temperature is treated aggressively with paralytics and or demerol. • Mechanically ventilated patients are deeply sedated. • Midazolam (Versed) drip (0. 5 mg/ml) 50 mg/100 ml NS Initiate at 1 – 2 mg/hr • Fentanyl drip (5 mcg/ml) 500 mg/100 ml NS -Initiate at 0. 5 mcg/kg/hr. • Atracurium (Tracrium) 0. 3 – 0. 5 mg/kg IVP as loading dose, followed by 8 – 14 mcg/kg/min continuous infusion with both Train of Four and Bi. Spectral Index (BIS) Monitoring options. – Train of 4 titrate 0 to 1 and Bi. Spectral Index < 60
Rewarming • After 18 hrs, begin warming the patient. • Set the cooling machine for a desired body temperature of 98. 5 degrees Fahrenheit (37. 5 degrees Celsius) with desired rate for warming at < 0. 5 degrees/hr. • DO NOT ALLOW THE PATIENT TO SHIVER. Rebound hyperthermia is common and must be avoided.
Physiological Effects of Cooling
Blood Gases and Temperature When a patient is cooled, p. CO 2, p. O 2 decrease, and p. H increases, measured at the patient’s temperature. At 37ºC in Machine: 7. 35 / 45 / 100 At 33ºC in Patient: 7. 41 / 40 / 90
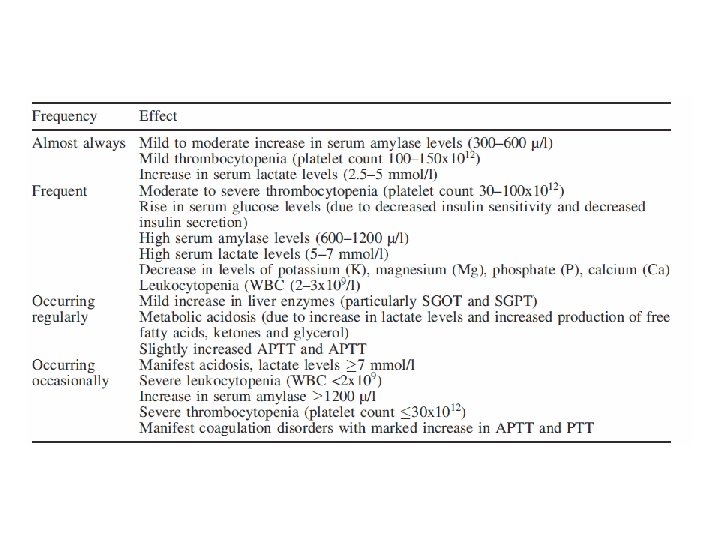
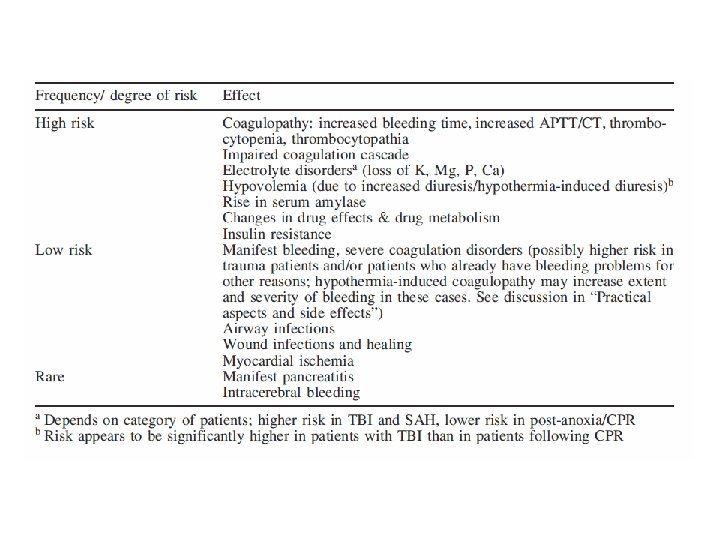
Complications of Cooling • Hypovolemia (hypothermia induced diuresis) • Coagulopathy (impaired coagulation cascade and thrombocytopenia) • Electrolyte disorders (hypothermia induced diuresis, K, Mg, Ca) • Insulin resistance • Changes in drugs effects and metabolism (altered clearance of fentanyl, midazolam, and atracurium)
Electrolyte and Fluid Shifts As you cool the patient, vasoconstriction will decrease effective vascular volume. - Diuresis - Lose potassium - Lose phosphate - Potassium shifts intracellularly As you warm up, patient intravascular space expands, and potassium shifts out of cells Danger of hyperkalemia if you replaced potassium earlier (Abiki 2001; CCM 29: 1726 -30; Zeiner 2004; Resuscitation 60: 253 -61)
Case Review • 65 yo wm presented to IRMC s/p cardiact arrest secondary to ventricular fibrillation with return of spontaneous circulation within 60 minutes – GCS on admission E 1, M 1, V 1 = 3 T – PMH: St. Jude Aortic Valve for AS, CAD, EF 25% – Meds: Coumadin, Furosemide, monopril
• Vital Signs and Labs – BP 122/72, HR 91, Temp 99 F, RR 26, Sat 99% – Vent Settings: PRVC TV 600 , Peep 0, FIO 2 = 100%, set rate 14 – ABG: 7. 47, 27, 484, 19. 5 – Na 139, K 4, BUN 16, Creat 0. 9 – INR 3. 7 – WBC 9, Hematocrit 41 – Troponin and CPK 2000
Hospital Course • Hypothermia protocol initiated with cold saline and Blanketrol III set to 93 F • Clinical assessment initially revealed hypovolemia: crystalloid volume loading – MAP >70 mm HG (presumed increased ICP) • ABG at 4 hours – p. H = 7. 255, PCO 2 59. 4, Pa. O 2 278 – Could not correct respiratory acidosis till paralysis initiated, train of four 0 to 1 and bispectral to 40
Hospital Course • First 6 hours – – – K = 2. 8, repleted P = 1. 8 repleated Lactic acid = 2 INR > 5, corrected with FFP WBC decreased to 2. 7 • After 24 hours – CT Head, No Acute Intracranial Process – Paralysis stopped with slow neurologic recovery – Retroperitoneal Bleed recognized and treated
Questions?