Midterm Barium Enema Large Intestine It begins in

Midterm Barium Enema

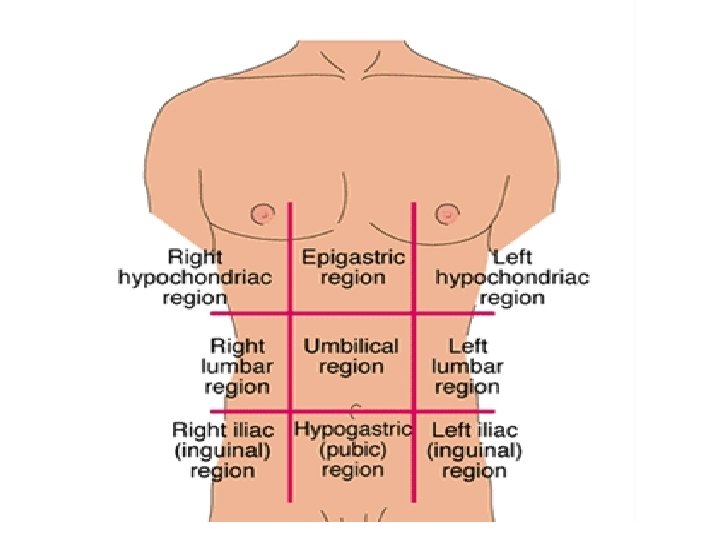
Large Intestine It begins in right iliac region when it joins the ileum of the small intestine. The length is approximately 5 ft. (152 cm) long and is greater in diameter than the small bowel (2. 5 in diameter).

Large Intestine Anatomy CECUM COLON RECTUM ANAL

Colon subdivision Ascending Transverse Descending Sigmoid
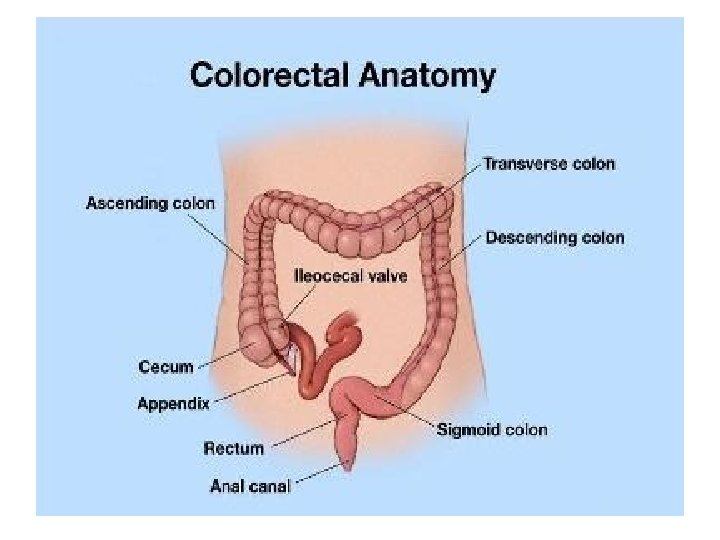

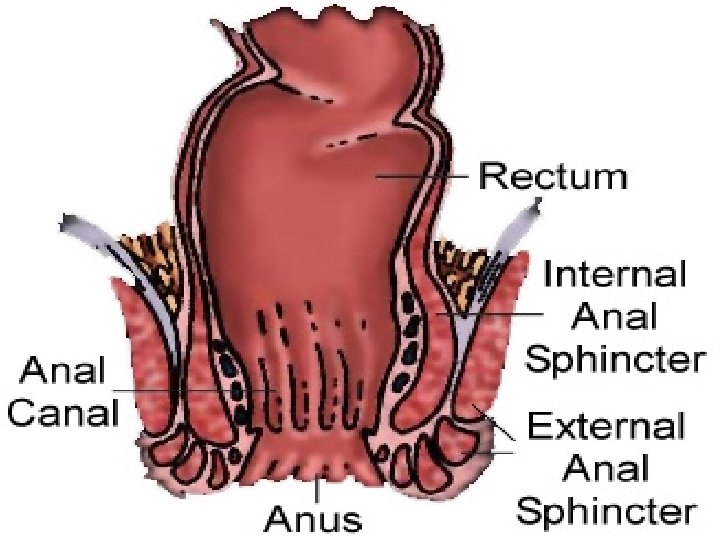
*Rectum and Anal Canal* Rectal Ampulla Anal canal Anus
 It is a Radiographic study of the")
Barium Enema (BE or Lower GI series) It is a Radiographic study of the large intestine. Purpose: to study radiographically the form and function of the large intestine, as well as to detect any abnormal conditions.

Clinical Indications

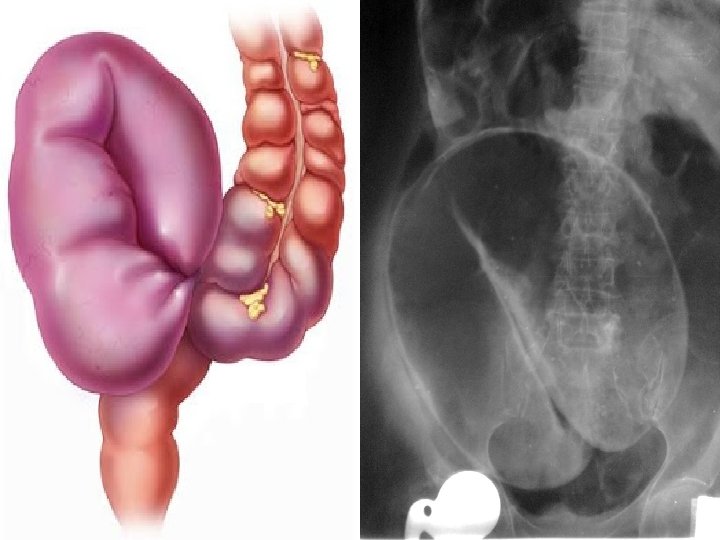
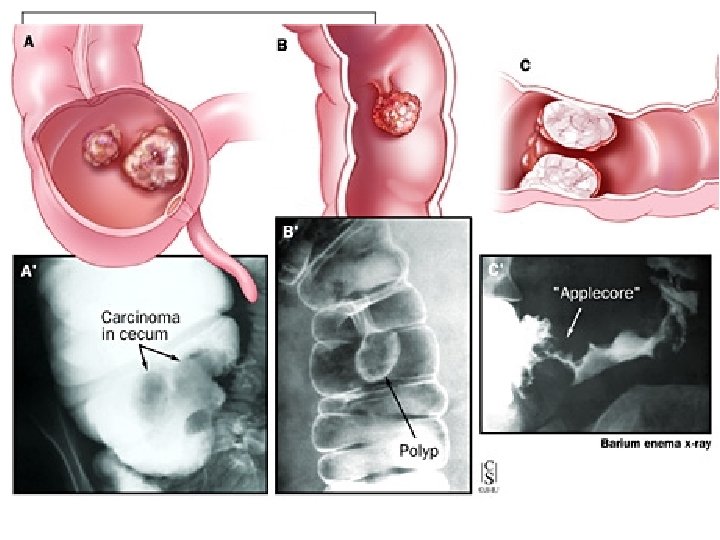
Colitis caused by many factors including bacterial infection, diet, stress, and other environmental conditions. Diverticulum outpouching of the mucosal wall resulting from herniation of the inner wall of the colon. Neoplasm tumors in large intestine. Volvulus twisting of a portion of the intestine on its own mesentery.

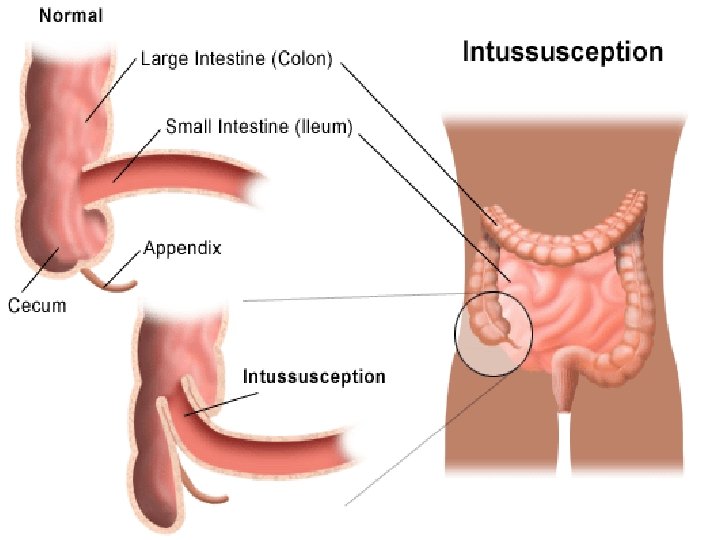
Intussusceptions telescoping of one part of the bowel into another. Polyps A polyp is an abnormal growth of tissue projecting from a mucous membrane.

 Pregnancy")
Contraindications to Cathartics Gross bleeding Severe diarrhea Obstruction Inflammatory lesions (appendicitis) Pregnancy

Preparation of the Patient The final objective is that the section of alimentary canal to be examined must be empty. 2 – classes of Cathartics Irritant cathartic – castor oil Saline cathartic – magnesium citrate or sulfate

Irritant Cathartic Saline Cathartic

Contrast media

Contrast Media High – density Barium Sulfate It is excellent for use in double-contrast studies of the alimentary tract in which uniform coating of the lumen is required. Air contrast Carbon dioxide may also be used because it is more rapidly absorbed than nitrogen of air when evacuation.

Mixture of Barium suspensions Single contrast 12 % - 25% weight / volume Double contrast 75% - 95% weight / volume

Barium Containers Closed system type enema Open system type enema

Closed system type Open system type

Enema Tips 3 – common enema tips Plastic disposable Rectal retention Air contrast retention

“Prior to any special procedure a scout film should be taken first. ”

Enema tips insertion Sims position – relaxes the abdominal muscles and decreases pressure within the abdomen.

Sims Position

Summary of Enema tip insertion Describe the tip insertion to pt. Place pt. in sims position. (pt. should lie on the left side, with the right leg flexed at the knee and hip 3. Shake and inspect the enema container to provide good mixture. Allow the barium to flow through the tubing and from tip to remove any air in the system 1. 2.

Continuation… Wearing gloves, coat enema tip with water-soluble lubricant. (KY jelly or any sterile lubricant) 5. On expiration, direct enema tip toward the umbilicus proximally 1 to 1. 5 inches 6. After initial insertion, advance up superiorly and slightly anteriorly. Do not force enema tip. 4.

Continuation… Tape tubing in place to prevent slippage. Do not inflate unless directed by radiologist 8. Ensure IV pole/enema bag is no more than 24 inches (60 cm) above the table. Ensure tubing stopcock is in the closed position and no barium flows into the pt. 7.

Procedures 3 – Types of Examinations of Colon Single – contrast Ba. Enema Double – contrast Ba. Enema Defecogram

Single Contrast Ba. Enema

Double Contrast Ba. Enema

Cont… Single – contrast utilizes only a positive contrast medium. Double – contrast Difference is that in an examination there is both air and barium.

2 - Approaches of Doublecontrast Administering

Two-stage procedure described “by Welin” A. In which the entire colon is filled with a barium suspension. B. Patient evacuates the barium and immediately returns to the fluoroscopic table for injection of air or other gaseous contrast into the colon.

Single-stage double contrast examination The barium and the air are instilled in a single procedure as compared to the two-stage which reduces time and radiation to patient.
 1) 2) 3) 4) 5) 6) 7) 7")
7 – pump method (by Miller) 1) 2) 3) 4) 5) 6) 7) 7 pumps, left lateral position 7 pumps, LAO position(left PAoblique) 7 pumps, prone position 7 pumps, RAO position 7 pumps, right lateral position 7 pumps, RPO position +7 pumps, supine position

10 – Miller’s Routine Sequence of Radiographs AP – to include flexures Left lateral rectum AP – 15 – 25 degs. Cephalic(CR) to include rectum. 4) 15 – 25 degs. RPO – to include Left colic 5) Right lateral – to include rectum 1) 2) 3)

Cont… Prone PA – to include flexures Prone PA with 15 – 25 degs caudal angulation (Angle Prone)– to include rectum. 8) 15 – 25 degs LPO- to include the right colic flexure. 9) Supine – AP tightly collimated ileocecal region proj. taken in 2 – 3 degs obliquity. 10) Using horizontal central ray, upright proj. of both flexures and lateral rectum. 6) 7)

Usually used in the hospital Modification of Positions for Barium Enema

Position and film Structure Shown used Central Ray • AP (recto sigmoid • AP view of the • 5 -7 cm above the area) Rectum & Sigmoid level of the pubic • Film: 10 x 12 cm should be included symphysis crosswise • Left/Right position • True lateral • 5 -7 cm above the of the recto sigmoid position of the level of the pubic area Recto sigmoid symphysis in the • Film: 10 x 12 cm midaxillary plane lengthwise • AP (Single Contrast) • An Entire colon • At the level of the L 4 • Film: 14 x 17 cm filled with contrast or at the level of the media should be iliac crest demonstrated including the splenic flexure and

Position and film Structure Shown used Central Ray • AP Double Contrast • Film: 14 x 17 cm lengthwise • An Entire colon filled with positive and negative contrast media should be demonstrated including the splenic flexure and the rectum. • At the level of the L 4 or at the level of the iliac crest • RAO Position (optional) • Film: 14 x 17 cm lengthwise • Entire colon should be included • Right colic (hepatic) flexure should be less superimposed or open when compared to the PA • At the level of the L 4 or at the level of the iliac crest • LPO Position (optional) • Entire colon should be • Film: 14 x 17 cm included lengthwise • Left colic (splenic) flexure should be less superimposed or open when compared to the PA • At the level of the L 4 or at the level of the iliac crest

Position and film used • Right Lateral Decubitus • Film: 14 x 17 cm lengthwise • Left Lateral Decubitus • Film: 14 x 17 cm lengthwise Structure Shown Central Ray • Best demonstrate • At the level of the L 4 the “up”, medial or at the level of the side of the iliac crest ascending colon and the lateral side of the descending colon, when the colon is inflated with air. • Best demonstrate • At the level of the L 4 the “up”, medial or at the level of the side of the iliac crest descending colon and the lateral side of the ascending colon, when the colon is inflated with air.

Position and film used • Ventral Decubitus • Film: 10 x 12 cm lengthwise Structure Shown Central Ray • A cross table view • 5 -7 cm above the of the recto level of the pubic sigmoid area symphysis in the • Demonstrate the midaxillary plane air-fluid level of the recto sigmoid area • PA Axial position • Rectosigmoid • Center it the (Angle Prone) area must be less midline of the body • Film: 10 x 12 cm or superimposition with an angulation 11 x 14 cm crosswise than in the PA of 30 -400 caudad at projection approximate level because of the anterior angulation of the superior iliac CR spines.

Position and film used Structure Shown Central Ray • Supine position • A postevacuation • At the level of the L 4 • Film: 14 x 17 cm radiograph view of or at the level of the lengthwise the colon is taken iliac crest after the procedure is done • If inadequate satisfactory delineation of the mucus the patient may be given hot beverage (tea/coffee) to stimulate evacuation • After care • Patient is advised to drink plenty of water, or laxative is taken to remove excess barium sulfate.

AP – Single Contrast

Double Contrast

Splenic Flexure

Left Lateral Decubitus

Right Lateral Decubitus

Lateral Cross table

0 Angle Prone 30 -40 caudad

Postevacuation
- Slides: 55