Mid Atlantic Neurodiagnostic Society Annual Meeting Nerve Conduction



 - Anterior")


















 • Clinical presentation may be similar • Eg-")















 • Posterior Interosseous Nerve (PIN) is a branch of the")








 from Chronic")
 and CIDP are acquired demyelinating polyneuropathy. •")






















, there")

 Pre-synaptic NMJ defect Post-synaptic NMJ defect • LEMS and Botulism")

 : Benign")







- Slides: 90
Mid Atlantic Neurodiagnostic Society Annual Meeting Nerve Conduction Studies & Electromyography Board Preparation Gauri Pawar, M. D. , F. A. A. N. Vice Chair for Education Professor and Residency Program Director WVU Neurology
Q 1 - NCS/EMG is useful in the diagnosis of which of the following conditions? • Middle cerebral artery stroke • Cervical myelopathy • Multiple sclerosis • Small fiber neuropathy • Carpal tunnel syndrome
NCS measures the large myelinated fibers • Patients with small fiber neuropathies tend to have normal NCS. • All motor and sensory latencies and conduction velocities are measured from the large myelinated nerve fibers • Large myelinated fibers have the most myelin and least resistance, therefore they have the fastest conduction velocities which are measured by routine NCS • The small myelinated (Aδ and B) and unmyelinated (C) fibers carry somatic pain and temperature sensation along with autonomic information. These are not measured by routine NCS.
NCS/EMG – Helps in the study of • Peripheral Nervous System (PNS) - Anterior horn cell within Spinal Cord (ALS, MND, Polio) - Roots (cervical radiculopathy or lumbosacral radiculopathy, root avulsions) - Plexus (Brachial or lumbosacral – from inflammation, infection, trauma, cancer or post radiation) - Peripheral nerves (large fiber neuropathy, GBS/AIDP, CIDP, MMN, CMT, etc) - Neuromuscular junction (Myasthenia gravis, LEMS, Botulism) - Muscle (muscular dystrophy, Inflammatory myopathies, myositis, toxic myopathy, etc). • Tests are useful in serial comparisons between studies performed on same patients at different times (pre and post surgery for carpal tunnel syndrome or radiculopathies • Tests are useful between 2 patient groups in scientific investigations. • EDX are an extension of the neurological exam. eg: CTS – can be diagnosed clinically, but severity can be better determined by NCS/EMG
Schwann cell & myelin - Myelin sheath is derived from Schwann cell. - It is present on all fast conducting fibers – motor and sensory. - Myelin is composed of concentric fibers of Schwann cell membrane with each Schwann cell supporting a single myelinated axon
Saltatory conduction - Myelinated fibers propagate action potentials by saltatory conduction. - Depolarization occurs at only uninsulated areas called Nodes of Ranvier. - Action potential jumps from one node to next. - Less membrane needs to be depolarized, so less time is required and therefore conduction velocity increases significantly. - Most human peripheral myelinated nerve fibers conduct between 35 -75 m/s.
Q 2 - A 27 year old woman has occasional tingling in her legs. Neurological examination is normal. Nerve conduction studies demonstrate prolonged sensory latencies with high amplitudes in legs and hands. What is the most likely explanation for this finding? • Inherited sensory neuropathy • Cold extremities • Sensory polyneuropathy • Sensory polyradiculopathy • Small fiber neuropathy
Q 3 – If NCS are performed on a cold extremity, which of the following effects may be seen? • Conduction block • Decreased SNAP duration • Increased nerve conduction velocity • Increased SNAP amplitude • Shortened distal latency
Effect of cool temperature while performing NCS • Prolonged distal latency • Slowed conduction velocities • Increase in duration and amplitude of SNAP and MNAP • SNAP are affected more than the MNAP • Maintain temperature of extremities between 32 - 34°C. • Motor and sensory conduction velocities drops between 1. 5 -2. 5 m/s for every 1°C drop in temperature • Distal latency prolongs by 0. 2 ms per 1°C drop in temperature • During repetitive stimulation, CMAP decrement may be reduced if extremity is cold. - Myasthenic patients feel clinically worse in warm weather • Recheck the temperature during the studies since temperature can reduce after initial warming of the extremities.
Temperature effect on RNS - Patient with myasthenia gravis after and before limb warming. - Decremental response is more obvious when the extremity is warmed.
Q 4 - By what age do the nerve conduction velocities reach normal adult values? • 10 years of age • 18 years of age • 3 -5 years of age • 32 weeks of gestation • At birth
Nerve conduction velocities • Nerve conduction velocities are usually half the adult value in full term infants. • As the process of myelination progresses, the normal adult range is reached at 3 -5 years of age. • Conduction velocity of unmyelinated fibers is about 3 -5 m/s. Myelinated peripheral nerve conduction velocities range from 35 -75 m/s. • Conduction velocities are faster in the arms than in the legs (length dependent) - distal nerve segments are tapered and therefore conduct more slowly than proximal segments - distal limb segments are cooler than proximal segments and therefore conduct more slowly • Calculated by distance between the proximal and distal stimulation site divided by the difference of proximal and distal latency. • Conduction velocity calculation reflect the fastest conduction fibers.
- Measured between distal and proximal stimulation sites. - Obtained by dividing the distance between the two points of stimulation by the difference in the CMAP latencies. - Because the latency measurement is made to the initial negativity, the CV measurement is that of the fastest conducting fibers. - With axonal GPN, CV can be slow but > 70% of normal value. - With demyelinating GPN, CV is < 70% of normal. - Cool extremity reduces CV. Conduction velocity
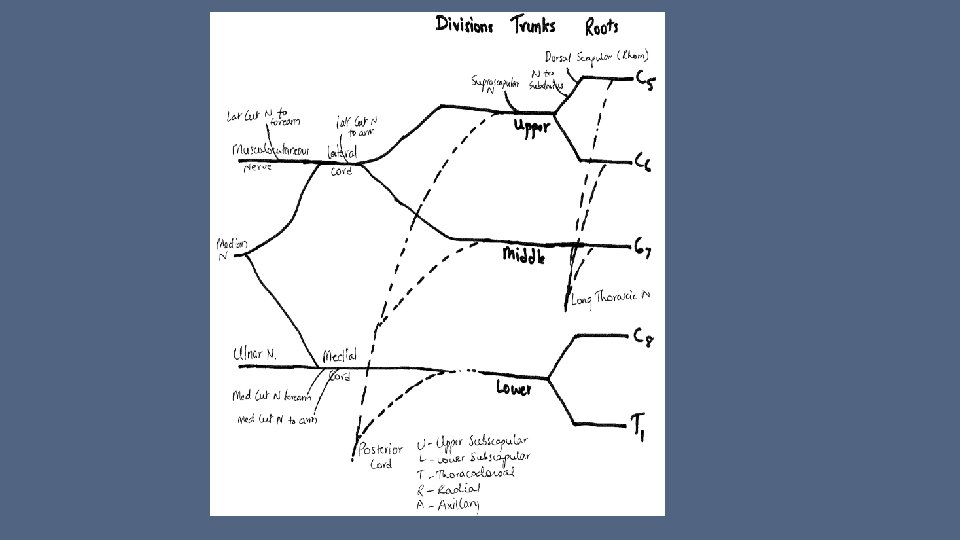
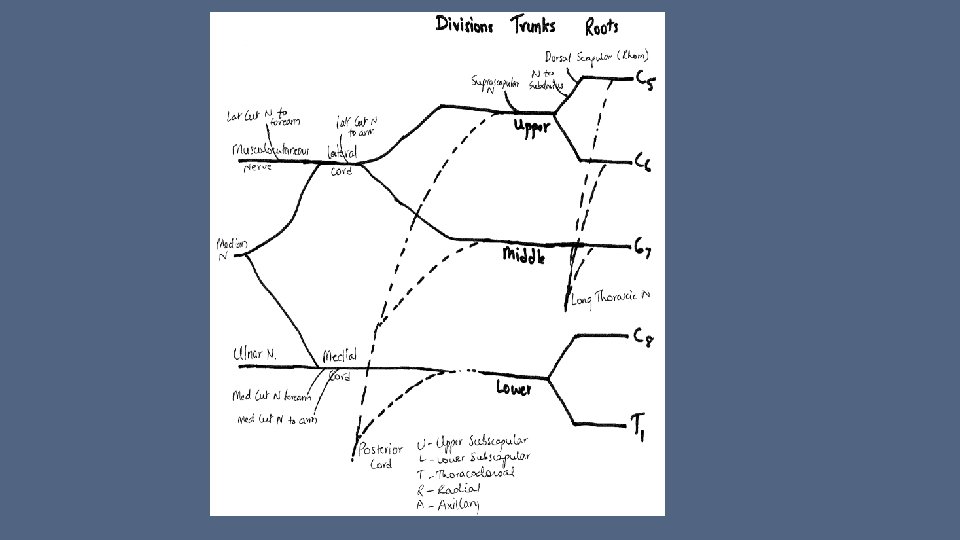
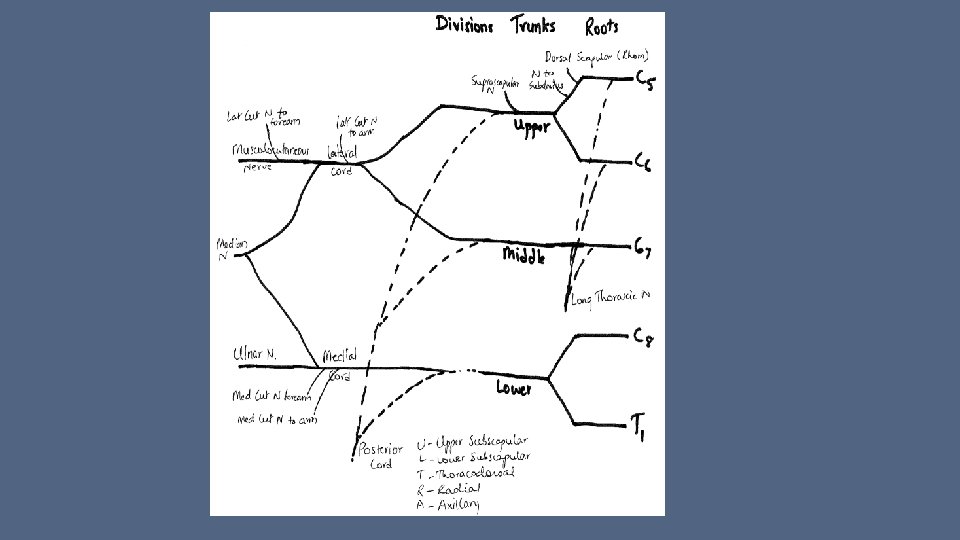
Brachial Plexus • Formed by nerve roots arising from C 5, C 6, C 7, C 8 and T 1 bilaterally • More complex than lumbosacral plexus because of the different trunks, cords, etc • Supply the muscles of the upper extremity. • Easier to remember muscle innervation based on what joint the muscle is acting on eg- Shoulder – C 5 Elbow – flexion C 5 -6, extension C 7 Wrist – flexion C 6 -7, extension C 7 Intrinsic hand muscles C 8 -T 1 • Extensor muscles of upper extremity are all radial innervated except brachioradialis (which is flexor) • All flexors of forearm muscles are median innervated except FCU which is ulnar innervated • All intrinsic hand muscles are C 8 -T 1 and ulnar innervated except for LOAF which is median innervated
Q 5 - A 52 year old carpenter is referred to EMG lab for possible carpal tunnel syndrome. He has no weakness or sensory changes on his examination. In mild carpal tunnel syndrome, which of the following median nerve response is most sensitive in confirming the diagnosis? • F-wave response • Motor conduction velocity • Motor response at the wrist • Palmar sensory response • Needle EMG of abductor pollicis brevis
Q 6 – A 48 year old secretary complains of wrist pain and tingling in her right thumb and index finger. Her symptoms awaken her from sleep but she has a normal neurological examination. Which of the following test is likely to reveal an abnormality? • Distal median motor latency • Peak sensory median latency • EMG of right abductor pollicis brevis muscle • EMG of right flexor carpi radialis muscle • EMG of right cervical paraspinal muscle
Carpal Tunnel Syndrome • Median palmar sensory response is the most sensitive electrophysiological test for diagnosis of CTS. • Median nerve entrapment is the most common compressive neuropathies. • In most cases, the most common site of compression is the carpal tunnel • Associated with numbness/paresthesias in the first 3 or 3. 5 digits, weakness of thenar eminence of the hand, invariably affects the dominant hand, depending on severity may affect the shoulder but neck is not involved. • Symptoms are worsened by flexion/extension of the wrist (during sleep, driving, holding a book/phone the symptoms can be exaggerated) • Sensation over thenar eminence is spared since this area is innervated by palmar cutaneous sensory branch which arises proximal to the carpal tunnel. • Muscles tested for CTS – FCR, FDI, APB (FCR would be affected in proximal median neuropathy, FDI would be involved in C 8 radiculopathy) • Thenar muscles supplied by Median nerve – LOAF (1 st 2 lumbricals, opponens pollicis, APB, FPB)
Median Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 7 – 53 year old woman in a MVA complains of acute neck pain radiating down her right upper extremity. She complains of numbness in the right 4 nd and 5 rd digits. She notices weakness in her hand has weakness in her grip strength. NCS performed 1 week after her injury of bilateral upper extremities are within normal limits. What is the localization of lesion in this patient? • Brachial plexus • Muscle • Neuromuscular junction • Peripheral nerve • Proximal to dorsal root ganglion
Q 8 – A 19 year old male is brought to the ER following a ATV accident. He has no sensations from C 7 level and cannot move any of his extremities. One week later patient has a normal NCS. What is the localization of lesion in this patient? • • • Brachial plexus Muscle Neuromuscular junction Peripheral nerve Proximal to dorsal root ganglion
Radiculopathy • Lesions proximal to dorsal root ganglion will present with sensory loss on examination but sensory NCS will be normal. • Q 8 - Woman with MVA had C 8 and or T 1 radiculopathy with numbness in 4 th and 5 th digits. - The ulnar sensory response is normal in patients with radiculopathy even when they have sensory loss. - To confirm a radiculopathy, one needs to perform needle EMG to see if there is denervation of muscles supplied by C 8 -T 1 roots • It may take 3 -5 weeks before one can see denervation changes on needle EMG. It is beneficial to wait to assess these patients or repeat a study at a later date/time.
PNS - Primary motor neuron resides within the spinal cord. - Primary sensory neuron (dorsal root ganglion –DRG) resides outside the spinal cord. - DRG is a bipolar cell. It’s proximal process forms the sensory root and the distal process forms the peripheral sensory nerve.
Plexopathy v/s radiculopathy (Brachial or lumbosacral) • Clinical presentation may be similar • Eg- In brachial plexopathy, proximal arm weakness may be related to C 5 -6 radiculopathy or plexopathy. • SNAP will be normal in radiculopathy • SNAP will be abnormal in plexopathy • Paraspinal muscles are abnormal in radiculopathy
Q 9 - Neurogenic thoracic outlet syndrome affects what region of the brachial plexus? • Posterior cord • Medial cord • Thoracodorsal nerve • Upper trunk • Lower trunk
Thoracic outlet syndrome. • Affects lower trunk of the brachial plexus. • Earliest and most common electrophysiological sign – small medial antebrachial cutaneous (MABC) sensory nerve action potential. • MABC nerve arises from the medial cord • NCS- abnormal ulnar sensory - abnormal median and ulnar motor.
Q 10 - Winging of scapula is seen with damage to which of the following nerves? • Long thoracic • Upper subscapular • Lower subscapular • Thoracodorsal • Axillary
Scapular winging • Long thoracic nerve innervates the serratus anterior muscle. • Winging of the scapula results when the patient pushes against a wall, especially with the shoulder adducted. • There may also be inability to abduct the arm beyond 90 degrees.
Q 11 - The thoracodorsal and subscapular nerves arise from which of the following structure in the brachial plexus? • Upper trunk • Lower trunk • Lateral cord • Medial cord • Posterior cord
Posterior cord of the Brachial plexus • Upper subscapular nerve • Lower subscapular nerve • Thoracodorsal nerve • Radial nerve • Axillary nerve
Q 12 - A 32 year old man presents with 3 month history of right upper extremity weakness following a fall. Nerve conduction studies show decreased radial and median sensory amplitudes. EMG shows fibrillation potentials in the biceps and deltoid muscles. The lesion can be localized to which area of the brachial plexus? • Lateral cord • Lower trunk • Medial cord • Posterior cord • Upper trunk
Upper trunk brachial plexopathy • Weakness of the proximal upper extremity muscles • Abnormal SNAPs in radial and median nerves • Biceps is innervated by musculocutaneous nerve which arises from upper trunk/lateral cord • Deltoid is supplied by axillary nerve which arises from upper trunk/posterior cord
Q 13 - Anterior interosseus nerve arises from which of the following nerves? • Radial • Axillary • Ulnar • Musculocutaneous • Median
Anterior interosseus nerve • Anterior interosseus nerve is a branch of the median nerve. • It has no cutaneous innervation. • Innervates 3 muscles- flexor pollicis longus, pronator quadratus, and FDP muscle to digits 2 and 3. • In a complete lesion to the nerve, patient is unable to make the “OK” sign.
Median Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 14 - A 52 year old man presents with a wrist drop. Needle EMG shows abnormalities of the extensor indicis, extensor carpi ulnaris and brachioradialis muscle. What is the site of lesion in this patient? • C 7 radiculopathy • Posterior cord of the brachial plexus • Posterior interroseus nerve • Radial nerve at the axilla • Radial nerve at the spiral groove
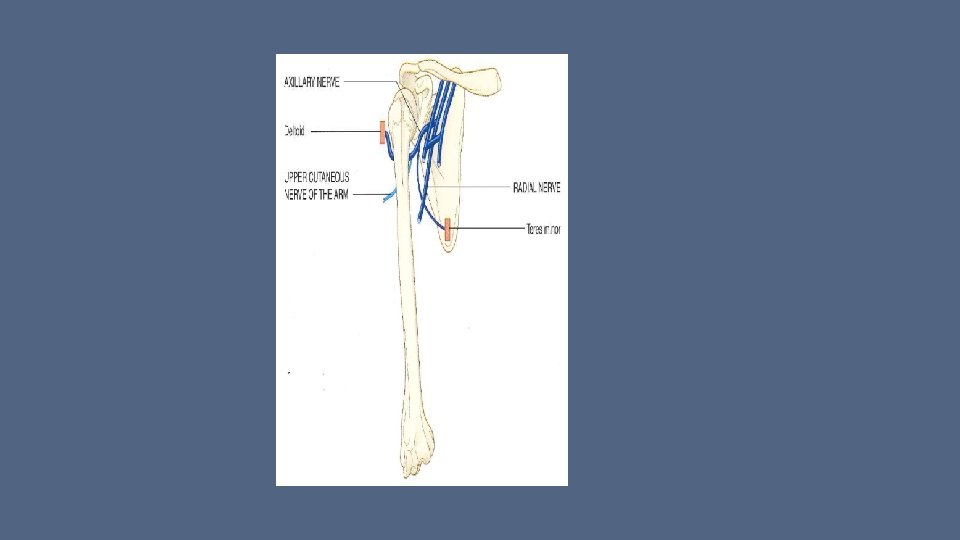
Radial neuropathy • Saturday night palsy • The radial nerve supplies the triceps proximal to the spiral groove • If triceps is spared and the brachioradialis is involved then the lesion is at the spial groove.
Radial Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 15 - “Finger drop” is seen with damage to which of the following nerves? • Median nerve • Ulnar nerve • Posterior interroseus nerve • Musculocutaneous nerve • Axillary nerve
Posterior Interosseous Nerve (PIN) • Posterior Interosseous Nerve (PIN) is a branch of the radial nerve. • The extensor carpi radialis longus gets branches directly from radial N and is spared in PIN lesions. • The extensor carpi ulnaris gets innervation from PIN. • All finger extensor muscles are weak in PIN lesion causing “finger drop”.
Q 16 - Martin Gruber anastomosis is seen between which nerves? • Axillary and radial • Median and ulnar • Ulnar and radial • Radial and median • Musculocutaneus and radial
Martin-Gruber anastomosis • It occurs in 15 -30% of the population • Communicating branch from the median nerve, usually from anterior interroseus, to the ulnar nerve in the forearm. • It supplies most commonly the FDI, followed by adductor pollicis and ADM.
Q 17 - The median nerve innervates which of the following muscles? • Extensor pollicis longus • Extensor pollicis brevis • Abductor pollicis longus • Abductor pollicis brevis • Extensor digitorum longus
• Median nerve innervates the abductor pollicis brevis • Radial nerve innervates extensor pollicis longus, extensor pollicis brevis, abductor pollicis longus, extensor digitorum longus
Q 18 - Axillary nerve supplies which of the following muscles? • Biceps brachii • Teres minor • Teres major • Pectoralis minor • Pectoralis major
• Biceps brachii - musculocutaneous • Teres minor - axillary • Teres major – lower subscapular • Pectoralis minor – Medial and lateral pectoral • Pectoralis major- lateral pectoral nerve (Lat cord)
Q 19 – A 62 year old male started noticing trouble getting up from a couch about 7 days ago. His weakness worsened over past 2 days where he has trouble ambulating. Examination reveals lower extremity weakness with areflexia and near normal strength in his upper extremities. He notes having diarrheal illness about 2 weeks prior to his symptom onset. Based on the NCS finding, which of the following is the likely diagnosis in this patient? • Guillian Barre syndrome • Myasthenia Gravis • Limb girdle muscular dystrophy • Amyotrophic lateral sclerosis • Chronic inflammatory demyelinating polyneuropathy.
Q 20 – An 18 year old woman developed difficulty holding her head up over the past 6 months. She has some upper extremity weakness and distal lower extremity weakness along with areflexia all over. Based on the NCS shown, patient has which of the following clinical condition? • Amyotrophic lateral sclerosis • Chronic inflammatory demyelinating polyneuropathy • Facioscapulohumeral muscular dystrophy • Hereditary motor and sensory neuropathy • Myasthenia Gravis
Q 21 – Which of the following best distinguishes Guillian-Barre syndrome (AIDP) from Chronic inflammatory demyelinating polyneuropathy (CIDP)? • Abnormalities on lumbar puncture • Findings on Sural nerve biopsy • Interval from symptom onset to disease plateau • Results of nerve conduction studies • Response to treatment with IVIG
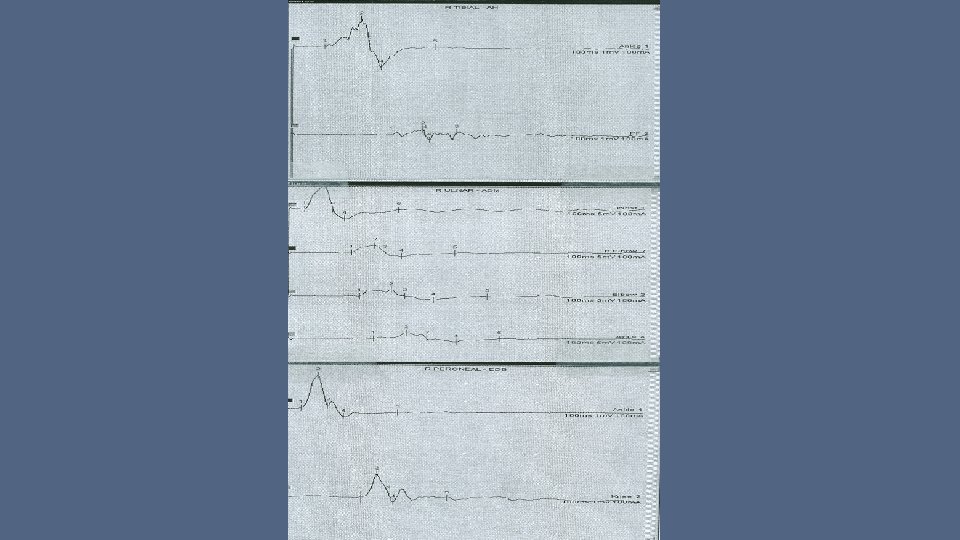
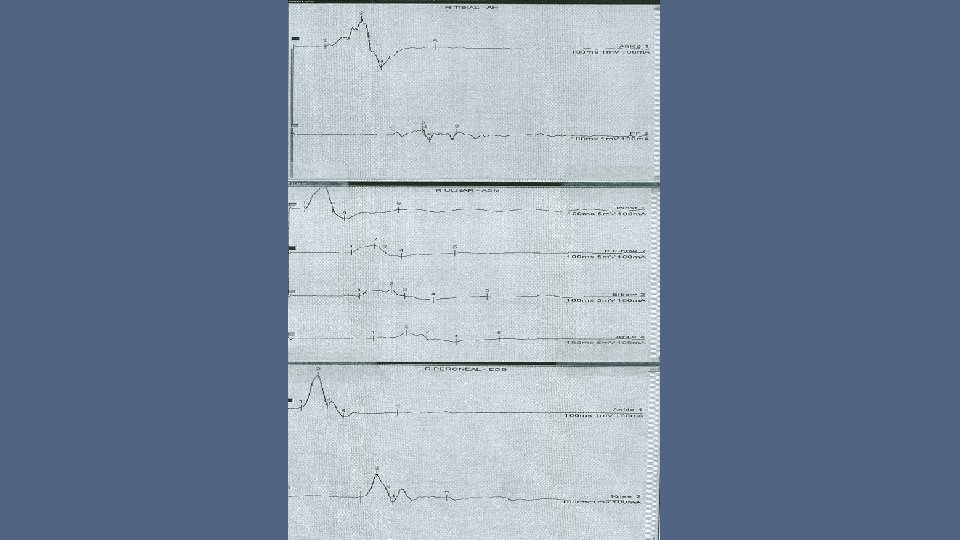
Inflammatory Demyelinating Polyneuropathy • Both AIDP (GBS) and CIDP are acquired demyelinating polyneuropathy. • CSF abnormalities are similar in both • NCS abnormalities are similar in both - Prolonged F-wave latencies (earliest sign in GBS and other generalized polyneuropathies) - Prolonged distal motor latencies - Temporal dispersion on motor action potentials - Conduction blocks (drop of > 50% amplitude between distal and proximal stimulation) • Clinical presentation with interval between symptom onset and disease plateau is main distinguishing factor between AIDP and CIDP. • In AIDP, disease plateaus in about 4 weeks. CIDP has a subacute presentation (3 -6 months)
F waves - F waves are small CMAP’s recorded from the muscle fibers of a single motor unit or a small number of motor units activated by antidromic action potentials that travel centrally along motor axons to the anterior horn cells. - Latency of a F wave is the time required for the action potential to travel antidromically from the site of stimulation to the spinal cord and time to travel orthodromically from the spinal cord to the muscle. - Because F waves travel over long segments of nerve, they are among the most sensitive measure of a diffuse nerve disease (GPN or AIDP).
F wave
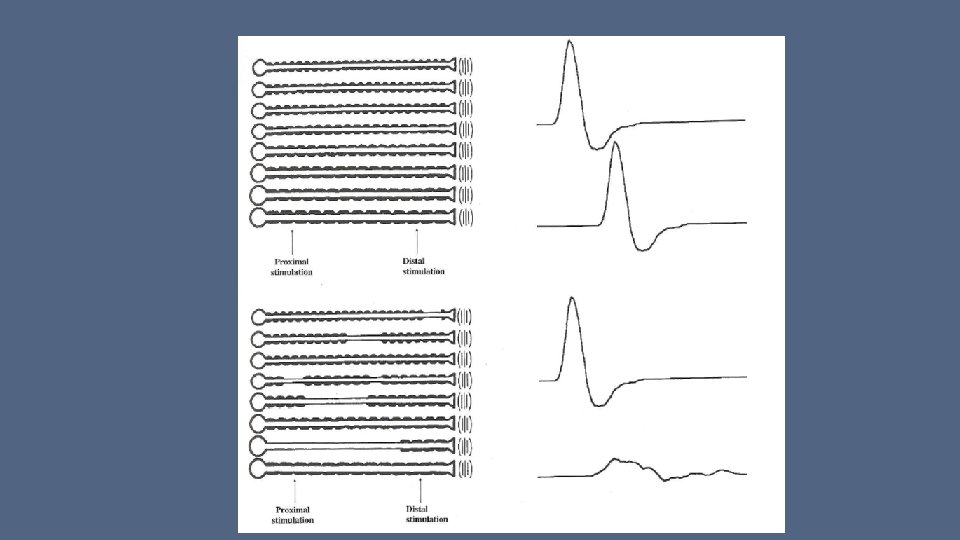
Q 22 – An ulnar motor nerve conduction study shows 50% decreased compound muscle action potential amplitude with stimulation at the elbow compared with stimulation at the wrist. This finding is seen in which of the following conditions? • Carpal tunnel syndrome • Charcot Marie Tooth Disease • Muscle denervation • Conduction block • Martin-Gruber Anastamosis
Conduction block • Seen on motor nerve conduction studies. • Drop of >50% amplitude between distal and proximal stimulation of the motor nerve. • Seen in acquired demyelinating neuropathies • Not seen in hereditary demyelinating neuropathy (CMT)
Q 23 - The median nerve conduction study in a 6 month old baby showed a conduction velocity of 25 m/s in the forearm. This baby has which of the following clinical condition? • Adrenoleucodystrophy • Charcot-Marie-Tooth disease type 1 A • Axonal neuropathy • Mixed axonal and demyelinating polyneuropathy • Normal motor conduction velocity
Normal nerve conduction velocity • Normal nerve conduction velocities in 6 month old child’s upper extremity are around 20 -36 m/s.
Lumbosacral plexus • Predominantly contributing roots are L 2, L 3, L 4, L 5 and S 1 bilaterally • L 2, L 3, L 4 forms femoral and obturator nerves • L 4, L 5, S 1 forms the sciatic nerve • Muscles supplied by the Femoral nerve are on the anterior aspect of the thigh • Muscles supplied by the Obturator nerve are on the medial aspect of the thigh • Muscles supplied by the sciatic nerve supply all the muscles on the posterior aspect of the thigh and all of the muscles below the knee. • Sciatic nerve forms the - Peroneal nerve – anterior and lateral aspect of the leg (foot dorsiflexion and eversion) - Tibial nerve – posterior and medial aspect of the leg (foot plantar flexion and inversion) - Sural nerve – sensation from lateral aspect of the foot.
Q 24 – In a patient with foot drop, needle EMG reveals fibrillation potentials in anterior tibialis, peroneus longus and short head of biceps femoris muscles. The medial gastrocnemius, vastus lateralis, gluteus medius and lumbar paraspinal muscles are spared. Where is the most likely pathology in this patient? • L 5 root • Lumbar spinal cord • Peroneal division of sciatic nerve • Tibial division of sciatic nerve • Femoral nerve
Foot drop • Foot drop can be presenting feature with multiple pathologies – myelopathy, lumbosacral plexopathy, radiculopathy (L 5), sciatic neuropathy, peroneal neuropathy, muscle diseases like myotonic dystrophy. • Fibrillation potentials on needle EMG indicates acute denervation in those muscles tested. They are seen in neurogenic or myopathic processes. • Foot drop is seen in L 5 radiculopathy and peroneal neuropathy. • In L 5 radiculopathy foot inverters and evertors are affected along with ankle dorseflexors. • In peroneal neuropathy, only foot evertors are affected along with ankle dorsiflexors.
Sciatic Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 25 - Which of the following would be affected in L 5 radiculopathy, but spared in sciatic neuropathy? • • • Peroneus Longus Tibialis posterior Semitendinosus Tensor fascia latae Semimembranosis
Lumbosacral plexus • L 5 supplies – Tibialis ant Tib post Peroneus longus TFL (tensor fascia latae) Gluteus medius Semitendinosis, semimembranosis and biceps femoris (long and short head) • Sciatic supplies. All hamstring All muscles below the knee via peroneal and tibial nerves • TFL is affected in L 5 radiculopathy but spared in sciatic neuropathy.
Q 26 - A 70 year old woman notices a foot drop after a hip replacement surgery. Examination reveals weakness of the foot dorsiflexion, inversion and eversion with reduced right ankle jerk. NCS shows absent right superficial peroneal sensory potential, reduced amplitude of sural and peroneal motor potential. There is denervation of the right anterior tibialis, posterior tibialis and short head of biceps femoris. What is the most likely diagnosis? • Femoral neuropathy • Lumbosacral plexopathy • Lumbosacral radiculopathy • Sciatic neuropathy • Tibial neuropathy
Sciatic neuropathy • Seen after hip replacement surgery • NCS affecting changes to peroneal and sural component • Needle EMG shows changes to muscles supplied by - peroneal division (tibialis anterior and short head of biceps femoris) - tibial division (tibialis posterior)
Sciatic Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 27 - A 46 year old female gives 5 week history of right thigh pain along with buckling of her right knee. She is noted to have weakness of her hip flexors and knee extensors. Needle EMG shows fibrillation potentials in right vastus lateralis, iliopoas and rectus femoris muscles with normal adductor magnus and anterior tibilais muscles. What is the most likely diagnosis in this muscle? • Mononeurotis multiplex • Right femoral neuropathy • Right lumbar plexopathy • Right obturator neuropathy • Right L 5 radiculopathy.
Femoral neuropathy • Most distinct clinical symptom is buckling of knee since the knee extensors are weak. • Have trouble climbing stairs if hip flexors are weak • Occasionally seen after inguinal hernia repair. • Abnormalities are seen on the needle EMG for hip flexors (Iliopsoas) and knee extensors (quadriceps- rectus femoris, vastus lateralis, vastus medialis, vastus intermedius) • NCS of peroneal, tibial and sural nerves will be normal since they are branches of sciatic nerve. • Need to check femoral NCS • If adductors of the hip are affected (obturator nerve innervated muscles) then it can be related to lumbosacral plexopathy or radiculopathy. • Can distinguish between them by checking the paraspinal muscles which are abnormal in radiculopathy but not in plexopathy.
Femoral/Obturator/Peroneal Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 28 - Which muscle is supplied by the peroneal division of the sciatic nerve? • Tibialis posterior • Short head of biceps femoris • Rectus femoris • Soleus • Abductor digiti quinti
Peroneal Nerve • Supplies the foot evertors and dorsiflexors • Damage causes foot drop • The short head of biceps femoris is the only muscle proximal to the knee innervated by the peroneal division of the sciatic nerve.
Femoral/Obturator/Peroneal Nerve Aids to the examination of the peripheral nervous system – W. B. Saunders 4 th edition
Q 29 – In a 28 year old woman has diplopia and difficulty swallowing over the past 4 months. On exam she has fatiguable weakness and mild proximal weakness. Which of the following abnormality is expected for diagnosis of myasthenia gravis? • 15% decrement on 3 Hz stimulation • 15% decrement on 30 Hz stimulation • 150% decrement on 30 Hz stimulation • 30% increment on 3 Hz stimulation • 150% increment on 30 Hz stimulation
Myasthenia Gravis • On slow or low frequency repetitive stimulation (2 -3 Hz), there is more than 10% increment seen on repetitive stimulation of motor nerve.
Neuromuscular junction - Specialized junction between terminal axon and muscle fiber. - When action potential reaches the presynaptic terminal, acetyl choline is released, diffuses across the synaptic cleft and binds to acetyl choline receptors on the muscle membrane. - This binding causes production of end plate potential, which at a certain threshold causes generation of muscle fiber action potential.
Repetitive Nerve Stimulation (RNS) Pre-synaptic NMJ defect Post-synaptic NMJ defect • LEMS and Botulism • Myasthenia gravis • Decremental response at rest with slow RNS at 2 -3 Hz • Exercise for 10 sec or 50 Hz stimulation • Exercise for 60 sec • Incremental response of 150 -200% • Decremental response of >10% • CMAP amplitude on motor NCS can be small • CMAP amplitude on motor NCS is normal
Positive waves &Fibrillations • Seen in neurogenic and myopathic process - Lower motor neuron diseases : Anterior horn cell disease (ALS, Polio) : Radiculopathies : Plexopathies : Peripheral neuropathies, especially axonal - Neuromuscular junction diseases : Myasthenia gravis : Botulinum intoxication - Muscle diseases : Inflammatory, congenital or toxic myopathies : Muscular dystrophy
Fasciculations • Seen in neurogenic process only. - Normal : Benign (fatigue) : Benign with cramps - Lower motor neuron diseases : ALS : Radiculopathy : Peripheral neuropathy - Metabolic disorders : Anticholinesterase medications : Thyrotoxicosis
References: • Electromyography and Neuromuscular disorders - David C. Preston, Barbara E. Shapiro - Edition 2, Elsevier Butterworth Heinemann • Clinical Neurophysiology - Jasper R. Daube - F. A. Davis • Electrodiagnosis in diseases of Nerve and Muscle: Principles and Practice - Jun Kimura - Edition 2, F. A. Davis • Aids to the examination of the peripheral nervous system, W. B. Saunders, 4 th edition
Questions? Thank You
Q 30 – In the resting membrane potential, which ion has the highest intracellular concentration? • Calcium • Chloride • Magnesium • Potassium • Sodium • In the resting membrane potential, potassium has the highest intracellular concentration, followed by sodium, chloride and then calcium.
Q 31 – Which of the testing is most likely to cause a decrement of the CMAP in ADM muscle with repetitive stimulation of the ulnar nerve in Lambert-Eaton myasthenic syndrome? • Repetitive stimulation at 3 Hz • Sustained exercise for 5 seconds • Sustained exercise for 60 seconds • Low frequency (2 -3 HZ) repetitive stimulation of motor nerve causes decremental response in both pre (LEMS) and post synaptic (MG) neuromuscular junction disorders. • Brief sustained exercise and high frequency repetitive stimulation causes incremental response in CMAP amplitude in patients with LEMS.
Neuromuscular junction defects • Post synaptic defects - Myasthenia Gravis – antibodies to acetyl choline receptor - autoimmune, affects women > men, other diseases like thyroid disease associated - Fatigable weakness – worse after activity or towards the end of the day - Diplopia, dysphagia, dysarthria, dyspnea, extremity weakness, normal sensation - In older patients need to exclude underlying malignancy like thymoma • Presynaptic defects - Lambert-Eaton Myasthenic Syndrome (LEMS) –Antibodies to voltage gated Ca channels - Weakness improves somewhat after activity, - Dry mouth (come to visit with water bottle) - Can be associated with malignancy like lung cancer - Infantile Botulism – Within first year or life - Difficulty feeding, poor cry, poor suck, hypotonia, constipation, unreactive pupils
Electrophysiological evaluation of Myasthenia gravis • Perform motor and sensory NCS in one upper and one lower extremity nerves. - CMAP amplitude should be normal. - If CMAP amplitude is low, have the patient contract for 10 seconds and see if the CMAP amplitude improves, that indicates a pre-synaptic NMJ defect. • Perform repetitive nerve stimulation and exercise testing, preferably on a weak muscle as discussed earlier. • Perform needle EMG on distal and proximal muscles. - In severe myasthenia, the MUAPs may be small, short and polyphasic. Recruitment is normal or early. - Needle EMG can exclude denervating disorders or myotonic discharges, which may display abnormal decremental response on RNS. • Perform single fiber EMG (SF-EMG) if above tests are normal with very strong clinical suspicion. - Examine extensor digitorum communis for jitter and blocking - Normal SF-EMG in a weak patient excludes NMJ defect.
Technical factors influencing NCS/EMG • Physiological factors - Temperature - Age - Height - Proximal v/s distal segment - Anomalous innervations • Non-physiological factors - Stimulus artifact - 60 Hz interference - Co-stimulation of adjacent nerves - Electrode placement for motor studies - Antidromic v/s orthodromic stimulation - Limb position and distance measurement - Sweep speed and sensitivity - Distance between recording electrode and nerve (set differently per lab and reference value table)