Metro New York New Jersey Pediatric Board Review

Metro New York / New Jersey Pediatric Board Review Course Pediatric Nephrology June 2013 Leonard G. Feld MD Ph. D Levine Children’s Hospital Charlotte, NC

For the Exam Fluid and Electrolyte Metabolism A. Composition of body fluids -Intracellular, extracellular, Electrolytes (sodium, potassium, chloride), Protein B. Acid-base physiology -Normal mechanisms and regulation, Acidosis, alkalosis C. Electrolyte abnormalities - Sodium – Hypernatremia; Hyponatremia; Potassium Hyperkalemia; Hypokalemia; Chloride imbalance D. Disease states, specific therapy - Pyloric stenosis, gastroenteritis, acute renal failure, shock, SIADH, Cystic fibrosis, Dehydration, Hyperosmolar non-ketotic coma

For the Exam Renal Disorders A. B. C. D. E. F. G. H. I. J. Normal function, proteinuria, hematuria, persistent microscopic hematuria, causes of gross and microscopic hematuria, nonhematogenous etiology of red urine, dysuria, Incontinence - Nocturnal, functional, daytime incontinence, Congenital - Renal dysplasia, unilateral multicystic dysplastic kidney, autosomal dominant polycystic kidney disease, autosomal recessive polycystic kidney disease, Juvenile nephronophthisis, Renal agenesis Abnormalities of the collecting system, kidney, and bladder – Hydronephrosis, Hydroureter and megaureter, Ureterocele, Vesicoureteral reflux, Abnormalities of the urethra - Posterior urethral valves, Urethral stricture Hereditary nephropathy - Familial nephritis, Congenital nephrotic syndrome Acquired - Infection of the urinary tract (Pyelonephritis, Cystitis), acute glomerulonephritis, Nephrotic syndrome, Hemolytic-uremic syndrome, Henoch. Schoenlein purpura, Ig. A nephropathy Renal failure - Prerenal failure, Intrinsic renal failure , chronic renal failure, Other - Trauma, renal injuries, Urethral injury, Toxins, Renal stones, Renal tubular acidosis, Hereditary conditions with renal manifestations, Nephrogenic diabetes, insipidus, Cystinosis Hypertension – General, Renal, Vascular, Adrenal, Pheochromocytoma, Cushing syndrome, Miscellaneous causes, Essential hypertension, Administration of drugs, Traction on legs

ANSWERS TO THE CONTENT SPECIFICATIONS • Fluid and electrolyte • Nephrology Leonard. feld@carolinashealthcare. org SUBJECT LINE: NYNJ PEDS

Outline • Fluid and Electrolyte abnormalities – Dehydration • Renal – Hematuria – Proteinuria – Hypertension – Urinary tract infections – Glomerulonephritis

Case 1: Dehydration A 4 mo old infant presents with a four to five day history of low grade fever (38 -38. 5 o. C), numerous watery diarrhea and decreased activity. Since the child refused to take her usual breast milk volume or solid foods, the mother and grandmother substituted non-carbonated soda (Coca-cola, ginger ale, apple juice or orange juice will have ~550 -700 m. Osm/kg H 2 O) with less than 5 m. Eq/L of sodium), and “sweet” (sugar added) iced tea. Over the last 12 hours there were a few episodes of emesis and there were less wet diapers. On examination the child was lethargic, dry mucous membranes, no tears, sunken eyeballs, and reduced skin turgor. Vitals signs were the following: Blood pressure 74/43 mm. Hg; Temperature of 38 o. C, respiratory rate of 36 per minute and pulse of 175 beats per minute. The weight was 6 kg. Weight at the time of her immunization 7 days ago was 6. 6 kg. There were no other significant findings.

Electrolyte Composition of Body Fluid Compartments March 17, 2005

BODY WATER DISTRIBUTION

Clinical Assessment Fluid Deficit Clinical Status Clinical Assessment Thirsty, HR, Normal BP tears, slightly dry mucosa, alert/restless, [urine] Mild ( 5%) 50 cc/kg Compensated Moderate (10%) 100 cc/kg Decompensated Very dry mucosa, < skin turgor, sunken eyes, deep resp, weak pulses, cool extremities, oliguria Severe (15%) 150 cc/kg Shock Intense thirst, BP, cap refill > 3 sec, weak pulses, apnea/rapid breathing, coma, anuria

Maintenance Requirements Body wt 0 -10 kg 10 -20 kg Ø 20 kg TBW 100 ml/kg 1000 ml + 50 ml/kg for each kg > 10 kg 1500 + 20 ml/kg for each kg > 20 kg Na+ 3 m. Eq/kg K+ 2 m. Eq/kg Cl- 5 m. Eq/kg
![Deficit Type of Dehydration based on serum [Na] in m. Eq/L Water Sodium (m.](http://slidetodoc.com/presentation_image/75d34f98117017a80dec1fdde0eb091f/image-11.jpg "Deficit Type of Dehydration based on serum [Na] in m. Eq/L Water Sodium (m.")
Deficit Type of Dehydration based on serum [Na] in m. Eq/L Water Sodium (m. L/kg) (m. Eq/kg) Potassium (m. Eq/kg) Isonatremic [Na] 130 -150 100 -120 8 -10 Hyponatremic [Na] < 130 100 -120 10 -12 8 -10 Hypernatremic [Na] > 150 100 -120 2 -4 0 -4
,")
Laboratory Sodium 124 m. Eq/L, chloride 94 m. Eq/L normal 98 -118 m. Eq/L), potassium 4 m. Eq/L (normal 4. 1 -5. 3 m. Eq/L), bicarbonate (or total CO 2) was 12 m. Eq/L (normal 20 -28 m. Eq/L or mmol/L), serum creatinine 0. 8 mg/d. L (normal ~0. 3 -0. 5 mg/d. L), blood urea nitrogen 40 mg/d. L, blood glucose 70 mg/d. L; complete blood count was normal except for a hemocrit of 38% (normal ~ 36%);
![Hyponatremia • • • Serum [Na+] < 130 m. Eq/L Water shifts into cells](http://slidetodoc.com/presentation_image/75d34f98117017a80dec1fdde0eb091f/image-13.jpg "Hyponatremia • • • Serum [Na+] < 130 m. Eq/L Water shifts into cells")
Hyponatremia • • • Serum [Na+] < 130 m. Eq/L Water shifts into cells – lower ECF volume <125 m. Eq/L – nausea and malaise < 120 m. Eq/L – headache, lethargy, <115 m. Eq/L – seizure and coma

Loss of hypertonic Fluid and Sodium from the ECF secondary to Dehydration

Question 1: What is the appropriate parenteral solution A. 5% dextrose + 0. 45% isotonic saline + 40 m. Eq KCl /L B. 0. 45% isotonic saline + 40 m. Eq KCl /L C. 0. 9% isotonic saline + 40 m. Eq KCl /L D. 5% dextrose + 40 m. Eq KCl /L E. 5% dextrose + 0. 2% isotonic saline

Approach For this 6. 6 kg infant Maintenance requirements for 24 hours Water 100 m. L / kg x 6. 6 kg = 660 m. L Sodium 3 m. Eq / 100 m. L x 660 m. L = 20 m. Eq Potassium 2 m. Eq / 100 m. L x 660 m. L = 13 m. Eq For this 6 kg infant with hyponatremic dehydration at 10% Deficits for 24 hours Water Pre-illness weight – Illness weight = 6. 6 – 6 kg = 0. 6 kg = 600 m. L Sodium 10 m. Eq x 6. 6 kg = 66 m. Eq Potassium 8 m. Eq x 6. 6 kg = 53 m. Eq

Points on Hypernatremic Dehydration

Hypernatremia – SLOW and CLOSE Key points: look quiet then irritable on stimulation; may look better than % of dehydration based on weightd Fluid selection: 5% dextrose + ¼ isotonic saline (~30 -40 m. Eq/L of Na) + 20 m. Eq KCl /L • 1 st 24 hrs: 24 hrs of Maintenance + ½ deficit • 2 nd 24 hrs: 24 hrs of Maintenance + ½ deficit • Close monitoring of serum sodium every 2 -3 hours. Some have suggested using a higher [sodium] – 0. 45% isotonic saline or even isotonic saline to restore ECF volume then moving to a lower • sodium containing solution to restore the water deficit. This approach may also reduce the possibility of dropping the serum sodium too quickly and preventing neurological problems.

Hematuria Case: Susan is an 8 year old noted on routine exam to have moderate hematuria on dipstick. She has an unremarkable past medical history. Family history is negative in the parents and siblings for any renal disease. History of hematuria is unknown. A repeat urine in one week is still positive and a urine culture showed no growth.

Question 2: Which of the following test is the next step in the evaluation? A. VCUG and urine culture B. Renal sonogram and urine calcium to creatinine ratio C. Urology referral D. CBC and Direct Coombs E. Recheck in two years

More on Hematuria • Repeat a first AM void following restricted activity , perform a microscopic on a fresh urine • Check the family members • If there is still blood without protein, casts, crystals, normal BP with or without a strong family history, no further work-up is generally required. However a renal sonogram and urine calcium to creatinine ratio • Caveat - Family anxiety because of the connotation of blood and cancer in adults.

Glomerular v. Non-glomerular bleeding • Glomerular – oliguria, edema, hypertension, proteinuria, anemia • Non-glomerular – dysuria, frequency, polyuria, pain or colic, hx exercise – crystals on microscopic – mass on exam – medication history - sulfas, aspirin, diuretics

Initial evaluation of the patient with hematuria • • All patients: BUN, creatinine, kidney and bladder ultrasound, urine calcium to creatinine ratio Who should be worked up – Presence of proteinuria and/or hypertension , – History consistent with infectious history, HSP, systemic symptoms, medication use or abuse, strong family history of stones or renal disease/failure. – Persistent gross hematuria – Family anxiety - limit evaluation • Probable glomerular hematuria – C 3, ASO titer – possible: hepatitis, HIV, SLE serology , SSD – renal biopsy – not for persistent microscopic without proteinuria, decreased renal function, and/or hypertension • Probable non-glomeurlar hematuria – – urine culture, urine Ca/creatinine ratio possible: hemoglobin electrophoresis, coagulation studies, isotope scans, Flat plate, CT, ? ? IVP, cystoscopy

Pearls for Hematuria • Hematuria may be an important sign of renal or bladder disease • Proteinuria (as we will discuss) is the more important diagnostic and prognostic finding. • Hematuria almost never is a cause of anemia • The vast majority of children with isolated microscopic hematuria do not have a treatable or serious cause for the hematuria, and do not require an extensive evaluation. So a VCUG, cysto and biopsy are not indicated.

More Pearls • Urethrorrhagia – boys with bloody spots in the underwear – Presentation – prepuberal ~ 10 yrs – It is painless – Almost 50% will resolve in 6 months and > 90% at 1 year; it may persist for 2 yrs – Treatment – watchful waiting in most cases • Painful gross hematuria – usually infection, calculi, or urological problems; glomerular causes of hematuria are painless.

More Pearls – gross hematuria • Gross hematuria is often a presentation of Wilms’ tumor • All patients with gross hematuria require an imaging study. • If a cause of gross hematuria is not evident by history, PE or preliminary studies, the differential includes hypercalciuria or SS trait • Cysto is rarely helpful

Case 3 • 7 year old boy developed gross tea colored hematuria after a sore throat and upper respiratory infection. No urinary symptoms but urine output was decreased. He complained of mild diffuse lower abdominal pain. There is no fever, rash or joint complaints. Past med history was unremarkable but had intermittent headaches for two years. • On exam he was well (afebrile) with a BP of 95/65 m. Hg, no edema, some suprapubic tenderness and red tympanic membranes. The mother thinks that a similar episode occur on vacation a few months ago. • Urinalysis shows 20 RBCs/hpf, 5 -10 WBCs, 100 mg/d. L of protein, rare cellular and hyaline casts. Serum creatinine is 0. 8 mg/d. L, C 3 100 (normal).

Question 3: The most likely cause of the gross hematuria is: A. B. C. D. E. Myoglobinuria Urinary tract infection Obstructive uropathy Ig. A nephropathy Benign familial hematuria

Ig. A • IGA nephropathy – Boys > girls – Mostly normotensive, with persistent microscopic hematuria – Chronic glomerulonephrits – up to 40% of primary glomerulonephritis – Complement studies are nl, some inc Ig. A – Prognosis – not so good if > 10 yrs of age, proteinuria, reduced GFR, hypertension and no macrohematuria

Glomerular Non-glomerular Urinalysis Dysmorphic RBC Cellular casts Brown/tea color Bright red Clots Crystals Protein + + ++ + + - History Family Hx of ESRD Systemic disease Nephrolithiasis Trauma Symptomatic vomiting + + - + + + Physical Hypertension Systemic signs Edema Abdominal mass Genital bruising ++ + + - + + +

Red or Tea colored/ Brown Urine Fresh Centrifuged Urine Sample Sediment Red with Red Cells Hematuria Supernatant Red without Red Cells Hemoglobinuria* Myoglobinuria * Hemoglobinuria will have a red or pink hue to the serum NOTE: If there is no red sediment, no RBCs and a clear supernatant, consider other causes such as urates, bile pigments, beets, porphyria, some medications, etc.

Question 4 On routine physical examination, an 8 -yearold boy is found to have microscopic hematuria. The first step in your evaluation should be. A. Examine the urine sediment B. Order an renal ultrasound C. Obtain a voiding cystourethrogram D. Perform a CBC in the office E. Order an ASO titer and C 3

Question 5 An 8 -year-old boy presents with tea colored urine. He has very mild edema. History of strep infection about 2 weeks ago. The work-up should include all the following except. A. Complement studies B. Serum creatinine C. Urinalysis for protein D. Monitor blood pressure and urine output E. Obtain a renal ultrasound
 with low C 3")
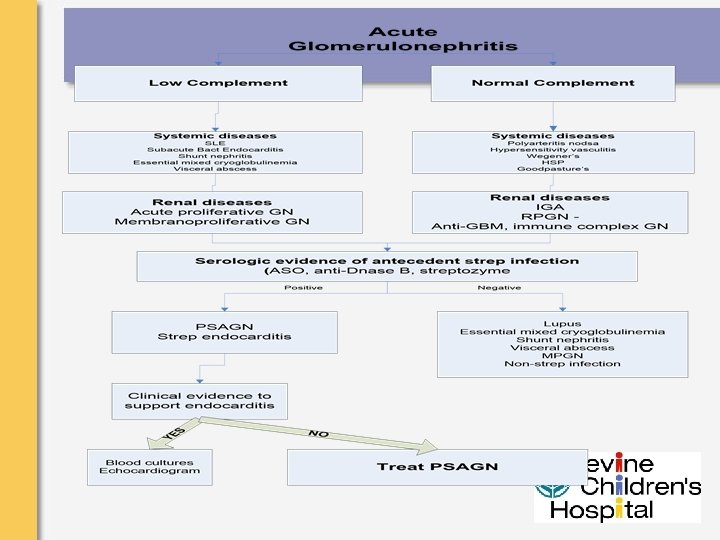
Acute glomerulonephritis: clinical • May be clinically asymptomatic (? 90%) with low C 3 and hematuria • Usually within 3 weeks after strep infection – mean about 10 days • Periorbital, peripheral edema • Hematuria - coke-colored, tea-colored, reddish/brown • Nonspecific findings such as abdominal pain, malaise, anorexia, headaches, pallor
 – most common • Acute Postinfectious")
Acute glomerulonephritis: DD • Acute Poststreptococcal glomerulonephritis (PSAGN) – most common • Acute Postinfectious or nonstreptococcal postinfectious glomlerulonephritis 9 AIAGN) – Bacterial: endocarditis (low C 3), shunt nephritis (low C 3), pneumococcal pneumonia, etc. – Viral: hepatitis B, infectious mononucleosis, varicella, etc, – Parasites: • Other: SLE (low C 3), membranoproliferative GN (low C 3), hyperthyroidism, HSP (nl C 3)

Acute glomerulonephritis: evaluation/ treatment • Evaluation – – ASO, C 3, C 4 Renal function Evaluation for hypertension and oliguria Magnitude of proteinuria • RX – supportive – Admission for hypertension, oliguria, impaired renal function, nephrotic syndrome • Prognosis: C 3 normalizes by 12 weeks, hypertension and other abnormalities resolve by 2 -3 months, hematuria may persist for 6 -24 mo

Proteinuria Case 6: John is an 12 year old noted on a basketball team physical to have 2+ protein on dipstick. There are no recent illnesses. He has an unremarkable past medical history and he is not taking any medications. Family history is negative in the parents and siblings for any renal disease.

Question 6: Which of the following is the best approach? A. B. C. D. E. Obtain a 1 st AM urine for protein Perform a complete biochemical profile Obtain a C 3, ASO and ANA Refer for a renal biopsy Schedule a renal sonogram and VCUG

What does Orthostatic Proteinuria mean? Protein Excretion

More on Proteinuria • Repeat a first AM void following restricted activity, perform a microscopic on a fresh urine; also an alkaline p. H may give a false positive result • If there is still protein perform a more formal orthostatic test. If orthostatic, no further work-up is generally required, although no indemnification from subsequent renal disease.

Causes of Proteinuria • Transient – fever, emotional stress, exercise, extreme cold, abdominal surgery, CHF, infusion of epinephrine • Orthostatic – Transient or fixed / reproducible • Persistent – – – Glomerular disease: MCNS, FSGS, MPGN, MN Systemic: SLE, HSP, SBE, Shunt infections Interstitial: reflux nephropathy, AIN, hypoplasia, hydronephrosis, PKD

Question 7 A four-year boy presents with a 5 -day history of swollen eyes and “larger ankles”. On exam he has periorbital and pretibial edema. The most appropriate tests include all the following except. A. Urinalysis B. Blood tests for total protein and albumin C. Serum creatinine D. Sedimentation rate E. Serum complement (C 3)
 • Urine protein to creatinine ratio – – – Normal: Mild to")
Definitions (Pearl) • Urine protein to creatinine ratio – – – Normal: Mild to moderate: Heavy or severe: < 0. 2 (< 0. 15 adolescents) 0. 2 to 1. 0 > 1. 0 • Persistent proteinuria: present both in the recumbent and the upright posture; even in this situation, proteinuira is less during recumbency March 17, 2005
 – mean age")
Nephrotic Syndrome • Primary Nephrotic Syndrome: – Minimal change disease (~75%) – mean age 4 yrs • No hematuria, nl C 3, no hypertension, nl creatinine – – Membranoproliferative GN (~ 5 -10%) FSGS (5 -10%) Proliferative GN, Mesangial proliferation Membranous nephropathy • Secondary Nephrotic Syndrome: – SLE, HSP, diabetes mellitus, HIV, vasculitis, malignancy (lymphoma, leukemia), drugs (heroin, inteferon, lithium), infections (toxo, CMV, syphilis, hepatitis B and C)etc. • Congenital/Infantile Nephrotic Syndrome: – Finnish-type congenital nephrotic syndrome, Denys-Drash syndrome – Diffuse mesangial sclerosis, Nail-patella syndrome

Nephrotic Syndrome - RX Corticosteroid treatment • Induction therapy: – Exclude active infection or other contraindications prior to steroid therapy. – Oral prednisone or prednisolone at 60 mg/m 2/d (~2 mg/kg/d) daily for 4 weeks. • Maintenance therapy (following above induction therapy) – Oral prednisone or prednisolone at 40 mg/m 2 (or ~1. 5 mg/kg) given as a single dose on alternate days for 4 weeks. – NOTE: Some nephrologists recommend daily induction steroid treatment for 6 weeks, followed by alternate day maintenance therapy for another 6 weeks. • Relapse therapy – For infrequent relapses, Prednisone 60 mg/m 2/d (~2 mg/kg/d) given as a single morning dose until proteinuria has resolved for at least 3 days. – Following remission of proteinuria, prednisone is reduced to 40 mg/m 2 (or ~1. 5 mg/kg) given as a single dose on alternate days for 4 weeks. Prednisone may then be discontinued or a tapering regimen. Frequently relapsing nephrotic syndrome is defined as steroid-sensitive nephrotic syndrome with 2 or more relapses within 6 months or more than 3 relapses within a 12 -month period.

Hypertension

Hypertension Question 8: David is a 10 year old boy first noted to have an elevated blood pressure of 123/85 during a annual physical examination. Pt has a long history of learning and behavioral issues. He has a previous history of headaches that were evaluated with a CT scan of the brain and sinuses. On following evaluation in one week, his BP is 126/86 mm. Hg with a weight > 99%ile for age and a height at ~50 th %ile.

Question 8: What is the most appropriate initial testing for this child? A. Renal mag-3 flow scan B. Electrolytes, BUN, Creatinine, Bicarbonate C. Renal Sonogram with doppler D. Urinary screening for drugs E. 24 hour urine for catecholamines

BP Classification Grade of hypertension Definition Appropriate next step “White-coat” hypertension BP levels >95 th percentile in a physician's office or clinic, but normotensive outside a clinical setting Readings may be obtained at home with appropriate family training or with the assistance of a school nurse, or with the use of ambulatory BP monitoring (ABPM) Normal < 90 th %ile Pre-hypertension >120/80 mm Hg should be considered pre-hypertensive or 90 -95%ile Additional readings may be obtained at home with appropriate family training or with the assistance of a school nurse Stage I hypertension 95 th -99 th %ile + 5 mm. Hg Organize a diagnostic evaluation in a non-urgent, phased approach Stage II hypertension Average SBP or DBP that is >5 mm Hg higher than the 99 th percentile Organize a diagnostic evaluation over a short period of time in conjunction with pharmacological treatment Hypertensive urgency and emergency Average SBP or DBP that is >5 mm Hg higher than the 95 th percentile, along with clinical signs or symptoms Hospitalization and treatment to lower the blood pressure

Estimate of Hypertension Estimate without height adjustment 1. If systolic BP equals or exceeds 100 + 2 times pt age in yrs 2. If diastolic BP equals or exceeds 70 + pt age in yrs Estimate with height adjustment 1. If systolic BP at 95 th %tile for age and sex Add 4 mm. Hg to the value at the 50 th %tile 2. If diastolic BP at 95 th %tile for height Add 2 mm. Hg to the value at the 50 th %tile

Evaluation of Hypertension

Indications for Treatment • • • Symptomatic hypertension Secondary hypertension Hypertensive target-organ damage Diabetes (types 1 and 2) Persistent hypertension despite nonpharmacologic measures

Pharmacologic Therapy for Childhood Hypertension • The goal for antihypertensive treatment in children should be reduction of BP to <95 th percentile, unless concurrent conditions are present. In that case, BP should be lowered to <90 th percentile. • Severe, symptomatic hypertension should be treated with intravenous antihypertensive drugs.

Urinary Tract Infections

Case 9 • A 4 mo old girl presents with low grade fever, mid-lower abdominal pain and nighttime-incontinence. She is not eating well. Prior visits she had normal blood pressure, urinalysis and excellent growth. Urinalysis shows hematuria, 30 mg/d. L of protein, leukocyte esterase and positive nitrite. Urine culture is obtained. 56

Question 9: What is the most likely bacterial cause of her urinary tract infection? A. B. C. D. E. Proteus mirabilis E. coli Coagulase positive Staphlococus Alpha hemolytic Streptococcus Klebsiella pneumoniae

Bacteriology /Pathogenesis UTI - 1 • Most Common - E. Coli, coliforms • Virulence Factors • adherence to uroepithelium by P-fimbriae • endotoxin release • Pyelo vs cystitis - 80 to 20% 58

Bacteriology /Pathogenesis UTI 2 • Perineal / urethral factors – uncircumcised - 10 -20 x risk – ? Urethral caliber (infant girls) – other myths such as bubble bath, wiping techniques • Low Urinary factors – dysfunctional voiding ; constipation • Other - indwelling catheters, congenital anomalies, Vesicoureteral reflux, sexual activity 59

Diagnosis • Leukocyte test and nitrite test • Urine culture > 40 -50, 000 CFU/m. L • Pyuria - not on recurrent UTIs 60

Clinical Issues • Lower tract - frequency, urgency, enuresis, dysuria • Upper tract - fever - nearly all in boys under 1 year of age; females peak in first year but still significant through the first decade • Asymptomatic bacteriuria - low risk 61

Radiological Evaluation • Renal ultrasound - anatomy, size, location, echogenicity • DMSA (2 nd choice glucoheptanate SGH) - cortical integrity, photopenic regions, differential function, abscess • CT scan - abscess • VCUG – not the current standard for first UTI; radionuclide for follow-up or siblings • IVP - NO WAY 62

AAP SEPT 2011 Practice guidelines • DX: Urinalysis with pyruria and culture with 50, 000 col/ml single organism by SPA or cath • Treat for 7 -14 days • Ultrasound for all with febrile UTI • VCUG only with abnl Ultrasound, or other findings to suggest atypical or complex issues • VCUG – after 2 nd febrile UTI • No Abx prophylaxis unless VUR grade V

Grades of Reflux 64

Reflux Recommendations “the simple way” • GRADES I - III Antibiotics • GRADES IV - V Surgery • Although endoscopic approach is gaining favor over open reimplantation 65

Treatment • Oral – SMX-TMP, Amoxicillin/Clavulanate – Cefuroxime, cefprozil, cefixime, cefprodoxime • Parenteral – Neoates: Ampicillin / Gentamicin – Older Children: • Advanced level cephalosporin • Beta lactam + beta lactamase inhibitor • Aminoglycoside (+ ampicillin) 66

Case 10: Case History • A 12 mo old girl is diagnosed with the first febrile UTI. She is not eating well. UA shows pyuria and bacteria. Urine culture is obtained and shows > 100, 000 colonies of E. Coli. Antibiotics are given. Feld - 10/98 67

Question 10: What is the most appropriate next step? A. B. C. D. E. Perform a DMSA renal scan Refer to urology for cystoscopy Perform a renal sonogram and VCUG Perform urodynamics and flow studies Repeat urine culture in 3 months

Glomerulonephritis / Acute renal failure

Case 11 • A 3 year old boy was attending summer camp. Five days later he presents with diarrhea, abdominal pain and appear pale. His mother finds out that there was cook out at camp. On examination the child is pale and is unable to void. His laboratory testing in your office shows a WBC of 26, 000, hemoglobin of 8 g/d. L, platelets 98, 000, Serum creatinine of 1 mg/d. L, BUN 54 mg/d. L, urinalysis with large blood, 100 mg/d. L of protein. 70

Question 11: What is the most likely diagnosis? A. B. C. D. E. Henoch Schoenlein Purpura Post streptococcal glomerulonephritis Ig. A nephropathy Acute pyelonephritis Hemolytic uremic syndrome

Clinical prodrome • Diarrhea prodrome 1 -15 days • Abdominal pain – may be confused with ulcerative colitis, appendicitis, rectal prolapse, intussusception • Pallor • Irritability, restlessnes • Edema – after rehydration • Oliguria/anuria

HUS: Clinical manifestations • • • Thrombocytopenia Hemolytic anemia Renal failure Neurologic (irritability, seizure, CVA) Pancreatitis (IDDM) and colitis Hypertension

HUS: Pathogenesis • Endothelial cell damage occurs secondary to toxin injury via binding to glycolipid receptor or lipopolysaccharide absorption.

HUS: Differential diagnosis • Other forms of acute Glomerulonephritis / renal failure • Vasculitis • Urosepsis • Renal vein thrombosis • Coagulopathy (DIC)

Conservative management • Fluid restriction to <insensible losses plus urine output • Foley catheter – limit to 24 -48 hrs • Blood transfusion / platelets • Routine use of antibiotics controversial • Diuretics • Nutrition

Surgical Complications • • Toxic megacolon Rectal prolapse Colonic gangrene Intussusceptions Perforation Strictures Mimic appendicitis, IBD

BONUS 1 John is a very dedicated weight lifter and started to take a creatine supplement. He asks you to explain the physiologic effects of creatine on his body. Which is the best explanations about creatine? 1. Creatine which is synthesized in the liver and kidney, is transported through the blood to be taken up by high energy demand of the brain and skeletal muscle. 2. Creatine supplementation affects hydration status and heat tolerance during exercise leading to muscle cramping and diarrhea 3. Creatine supplementation does improve physiological response to resistance exercise, increasing the maximal force production of muscles in men, not women. 4. Pasteurized cow's milk contains lower levels of creatine than human milk 5. Creatine has been shown to improve cognitive performance in young athletes.

BONUS 2 A 6 year old boy presents with recurrent episodes of brownish urine that developed coincidental with URIs. His urinalysis during the episodes reveals red blood cell casts and small protein. His complement levels are normal. His hepatitis B screen is normal. The MOST likely diagnosis is: 1. Post Strep AGN 2. Ig. A nephropathy 3. Membranoproliferative glomerulonephritis 4. Membranous nephropathy 5. Wegener’s granulomatosis

SOME QUICKIES • Unilateral multicystic dysplastic kidney – MOST COMMOM CAUSE OF ABDOMINAL MASS IN NEWBORN – ULTRASOUND AND VCUG to DETERMINE CONTRALATERAL DISEASE • Polycystic Kidney Disease – Autosomal recessive – bilateral enlarged kidneys with microcysts (Potter’s – pulmonary hypoplasia); overtime – liver fibrosis and failure – Autosomal dominant – MOST COMMON INHERITED KIDNEY DISEASE; bilateral enlarged kidneys with MACROCYSTS; association with cerebral aneurysm • Hydronephrosis – Usually obstruction; Ultrasound may show enlarged kidney without hydroureter

• Posterior urethral valves – – MOST COMMON CAUSE of OBSTRUCTIVE UROPATHY IN MALES; remember poor urinary stream and palpable bladder • Vesicoureteral reflux – Grades from I to V; VCUG diagnoses REFLUX, Radionuclide (DMSA) scans detect scars ; Surgery for grades IV to V (in general) • UTIs – E. coli most common followed by Klebsiella, Proteus. Males over 1 also have E. Coli then Proteus, Staph – Females > males; greater in uncircumcised; remember constipation may increase incidence of UTIs – DX – culture, cath or mid stream; UA – positive nitrites and leukocytes – 1 st febrile UTI – ultrasound ; VUCG for girls with more than 2 UTI in 6 months; all males

• Hematuria – Rule out hemoglobin and myoglobin – Brown urine – glomerular – look for red cell casts – Lower tract – gross red (possible at end of stream), no casts, possible clots – Rule out hypercalciuria – spot ratio – Common diseases • Ig. A – gross hematuria with respiratory or GI illness • Post Strep AGN – follows throat or skin infection by 10 -21 days, Low C 3 but recovers by 8 -12 weeks, maybe increased ASO titer • HUS – E. coli – 0157: H 7 – MOST COMMON CAUSE OF ACUTE RENAL FAILURE; low platelet count and microangiopathic hemolytic anemia (schistocytes; coombs negative)– cause undercooked meat or unpasteurized milk

• Proteinuria – Rule out Orthostatic Proteinuria; urine protein to creatinine ratio – abnormal above 0. 2 from AM specimen – Nephrotic syndrome – ratio greater than 2 or more the 40 mg/m 2/hr of protein • Minimal change – steroid responsive is MOST COMMON • Usually 2 - 6 yrs with mean of 4 yrs; remember edema is dependent - first eyes than later in day to the legs. • Treatment – prednisone – 60 mg/m 2/day for 4 -6 weeks followed by alternate day steroids for 4 -6 weeks.

• Tubular entities – Diabetes insipidus • X linked or secondary to ADH resistance • Look for dilute urine in face of hypernatremia • Water deprivation test then give IV or intranasal vasopressin – Renal tubular acidosis – normal anion gap – hyperchloremic metabolic acidosis • Proximal or Type II – bicarbonate wasting – Failure to thrive – p. H < 5. 5 – Serum bicarbonate usually less than 18 – Remember FANCONI syndrome is RTA = glycosuria, phosphaturia, and amino aciduria. – Treated with bicarbonate

– Distal or Type I – impaired distal acidification; p. H > 5. 5; may have hypokalemia and hypercalciuria – Look for polyuria, vomiting, nephrolithiasis – Treated with bicarbonate – low dose compared to proximal – Bartter syndrome • Hypochloremic metabolic ALKALOSIS; hypokalemia. • Look for polyuria, failure to thrive, low serum chloride and low potassium – Kidney Stones • Imaging of choice – spinal CT. • Most stones are radiopaque since they contain calcium. Nonradiopaque are uric acid stones. • Cystinuria – increased urinary excretion of dibasic amino acids
 – Evaluation to determine – prerenal (perfusion); renal")
• Acute kidney injury (failure) – Evaluation to determine – prerenal (perfusion); renal (intrinsic) or post renal (obstruction) • Chronic kidney disease – Key items – anemia, growth failure, renal osteodystrophy – Options – dialysis and preferred renal transplantation

Outline – Part 2 • Acute renal failure • Chronic renal failure • More Fluids & Electrolytes • Tubular disorders • Cystic kidney disease

SCENARIO A 6 year boy is diagnosed as having ALL. He is started on chemotherapy and his white blood cell count drops precipitously. The child is discharged and the family is encouraged. However, after two days at home he spikes a temperature to 39 C. The parents contact the heme/ onc fellow who tells them to come to the hospital immediately. On arrival to the ER, the child is a bit lethargic. His BP is 60/40. What is the most important first step in the management of this child? What are the most useful diagnostic tests? What are the possible causes of his condition? How should his condition be treated?
 vs Pre-renal Azotemia • Key maneuver is restore RBF to")
Acute Renal Failure (ARF) vs Pre-renal Azotemia • Key maneuver is restore RBF to distinguish reversible pre-renal state from short-term irreversible • Options – Bolus infusion of crystalloid solutions – Infusion of albumin – Administration of pressors – Administration of antagonists of clinical condition as in anaphylaxis

ARF: Diagnosis Pre-renal AGN ATN Obstruction UA Marginal value Key RTEC RBC casts Marginal value SG >1. 020 1. 0081. 012 1. 008 -1. 012 UNa <20 >40 FENA <1% >1% Uosm >400 200 -400

ARF: Diagnosis • AGN – PSAGN – HSP – SLE – MPGN – Wegener’s March 17, 2005

ARF: Diagnosis • ATN – Unreversed pre-renal azotemia – Nephrotoxic meds – Contrast agents – High calcium, uric acid, phosphate – Rhabdomyolysis (myoglobin) – Intravascular hemolysis (hemoglobin)

ARF: Diagnosis • Obstructive uropathy – PUV – Prune belly – Vesicoureteric reflux – Neurogenic bladder (myelomeningocele) – Megacystis/megaureter – Secondary: stones, fibrosis • Effect of age and gender

ARF: Testing • • • Key labs: BUN, creatinine, K EKG CXRay Renal ultrasound Specific blood tests based on underlying condition

ARF: Management • Urgent issues – Potassium • Calcium • Glucose/insulin • NOT bicarbonate – Blood pressure: parenteral therapy • Labetalol • Nitroprusside – ECF volume

ARF: Conservative Management • Potassium – Diet restriction – Kayexalate • Blood pressure – IV/PO meds • ECF volume – Na restriction – Diuretic use – need for furosemide

ARF: Indications for Dialysis • • Refractory hyperkalemia Refractory hypertension Symptomatic ECF volume overload Symptomatic azotemia – Infection – Bleeding – CNS changes

ARF: Pearls • Pre-renal azotemia and AGN are similar • ATN and post-renal failure are similar • Potassium kills first in ARF

SCENARIO A 6 year boy is seen at a routine physical examination. Although he has no specific complaints, his mother says he has been very listless and his appetite is very poor. He has not been playing well with his friends in play group. Although he is toilet trained he seems to be having more accidents during the night. On examination, he looks a bit pale and tired. His height has fallen from the 50% at his last visit 18 months ago to 10%. His BP is 106/62 mm Hg. What is the most important first step in the diagnosing this child’s problems? What are the likely causes his condition? How should his condition be treated?

CKD: Diagnosis • Stages – CKD I: renal injury GFR >90 – CKD II: GFR 60 -90 – CKD III: GFR 30 -60 – CKD IV: GFR 15 -30 – CKD V: ESRD

CKD: Common features • • Impact on growth Impact on bone: osteodystrophy Impact on puberty Impact on development – social and cognitive

CKD: Causes • Non-glomerular – Hypoplasia/dysplasia – Reflux nephropathy – Obstructive uropathy • PUV • Prune Belly • Neurogenic bladder

CKD: Clinical manifestations • Growth failure – Dependent on age of onset – Dependent on level of GFR • UTIs – Pyelonephritis • Electrolyte abnormalities – Pseudohypoaldosteronism – Nephrogenic DI • Neurocognitive disability

CKD: Diagnosis • Structural assessment • Imaging studies – US – VCUG: dye vs radioisotope – DMSA scan – Retrograde studies, etc

CKD: Diagnosis ARF Younger child, abd mass, UTI UA WBC, impaired concentration US, VCUG, DMSA Retrograde studies Cystoscopy, urodynamics

SCENARIO A 15 year old girl comes to the clinic because she has not had her period for the last 8 months. She feels tired all the time at home school and is having a hard time concentrating in school. She is not taking any medications except for occasional NSAIDs for headaches and some vitamins. Her parents are in good health. On examination, her height and weight are normal. Her BP is 162/98 mm Hg. She is pale and has a mild amount of edema in both legs. She has no rash or arthritis. What is the most important first step in diagnosing this adolescent’s problem? What are the most likely causes? How should her condition be treated?
 –")
CKD: Causes • Glomerular – FSGS – HUS – SLE – Membranoproliferative MPGN) – Alport – Ig. A Nephropathy – Membranous nephropathy – NOT diabetic or hypertensive nephropathy

CKD: Clinical manifestations • Growth failure – Dependent on age of onset • Hypertension – Role of ECF volume and PRA • Electrolyte abnormalities – Acute – Hyperkalemia • Edema • Signs of underlying disease

CKD: Diagnosis • Low value of radiology tests • Blood tests – C 3, C 4, CH 50 – ASLO – ANA, ds. DNA, Ro, La, Sm – ANCA – Anti-GBM – Renal biopsy

CRF: Management • Nutritional supplementations – CHO deficiency • Protein restriction – Impact on growth – Effect in more advanced CKD • BP control – Disease progression – ACEI/ARB

CRF: Management • Interference with renin-angiotensin aldosterone axis – Safety of ACEI even with advanced CKD – Role of combined ACEI/ARB – Effect of aldosterone antagonists • Safety issues – Hyperkalemia – Reduction in GFR

CRF: Management • Endocrine treatments – rh. GH • Doubles growth velocity • Minimal risk of progression – Erythropoietin • Nearly always effective • Antibody induced pure red cell aplasia – Calcitriol • IV route • More selective agents

CRF: Pearls • Chronic glomerular diseases have oliguria vs chronic tubular diseases which can have polyuria and sodium loss – Nocturia and enuresis may indicate CRF • Severity of growth failure and neurocognitive deficits are inversely related to age of onset of CRF

CRF: More pearls • Most important feature of nutritional support is to correct low caloric intake • Medication doses need to be adjusted as GFR declines • Almost no form of CRF is a contraindication to transplant

SCENARIO A 10 -day male infant presents with a history of irritability, low grade fever, emesis and diarrhea. Prenatal and family history is non-contributory. On examination the infant is irritable, temp is 38°C, has mottled skin and a capillary refill of 4 sec. The systolic blood pressure is barely palpable and the pulse is 195 beats/min. The anterior fontanelle is flat. Hemoglobin 18 g/dl White cell count 30, 000 Platelets 280, 000 What are key features in the history and examination? What studies would you perform? What is your initial therapy? What is your initial diagnosis (es)?

Electrolyte Disorders: Sodium • KEY function of Na+ – ECF cation – Maintenance of intravascular compartment • Disturbances in ECF volume are secondary to disturbances in Na+ balance • ECF volume assessment is clinical – Reduced – see dehydration above – Increased – pulmonary and/or peripheral edema March 17, 2005

Electrolyte disorders: Sodium Assess ECF Measure serum Na High ECF Normal ECF Low ECF

Electrolyte Disorders: Sodium • • History Source of Na loss Change in body weight Renal response to low ECGF volume – Oliguria – Reduced urine Na+ – Reduced FENA March 17, 2005

Electrolyte disorders: Sodium

Electrolyte disorders: Sodium • Hypernatremia – Risk factors • • Breast feeding Feeding errors Impaired thirst Impaired access to water – Presentation • Irritability, seizures – Treatment • SLOW • HYPOTONIC FLUIDS – 1/5 NS
")
Electrolyte disorders: Sodium • Hyponatremia – Risk factors • • • Feeding errors (Keating) Salmonella diarrhea Increased extra-renal salt loss Pain, anesthesia, post-operative picture Female gender – Presentation • Lethargy, seizures – Treatment • ? SLOW • Correction 25 mmol/L OR 130 mmol/L over initial 48 hr

Electrolyte disorders: Sodium • Bad outcomes • Brain – Hemorrhage and cerebral edema in hypernatremia – Osmotic demyelinating syndrome and acute CNS deterioration in Hyponatremia • DKA – ? Hyponatremia ( 100 glucose mg/dl 1. 6 Na meq/l) – Comparison to hypernatremia

SCENARIO A 4 -week old infant presents with a history of irritability, low grade fever and poor feeding. Prenatal and family history is non-contributory. On examination the infant is irritable, temp is 37°C, has dark skin and a capillary refill of 4 sec. The systolic blood pressure is barely palpable and the pulse is 195 beats/min. The anterior fontanelle is sunken. Hemoglobin 18 g/dl White cell count 30, 000 Platelets 280, 000 What are key features in the history and examination? What studies would you perform? What is your initial therapy? What is your initial diagnosis (es)?

Electrolyte Disorders: Potassium • KEY function of K+ – ICF cation – Transmembrane potential, secretion, neuromechanical coupling • Disturbances in K+ reflect sudden changes in serum concentration and transmembrane ratio • Assessment is linked to cardiac impact of abnormal K+ concentration

Electrolyte disorders: Potassium • Regulatory organs – Kidney secretion • Na+ • Urine flow rate – Adrenal • Aldosterone – GI tract • Transmembrane – – p. H Osmolality Beta adrenergics Insulin • Diet

Potassium • Key tests – BUN, Cr, Na, K, bicarbonate – Urine K useless – Urine Na/K ratio – Hormones • PRA • Aldosterone

Electrolyte disorders: Potassium • Hyperkalemia – EKG • Peaked T waves – Treatment • • • Calcium infusion Glucose/insulin NOT Bicarbonate Kayexalate DIALYSIS

Hyperkalemia: differential diagnosis • No real disease – Increase cells: WBC, polycythemia, thrombocytosis, crush injury – Transmembrane • Renal – ARF – CRF – Liddle’s • Adrenal – Adrenal failure – Congenital adrenal hyperplasia – ambiguous genitalia – Isolated renin abnormalities

Hyperkalemia: Work-up • • BUN, creatinine, Na, K, Bicarbonate PRA Aldosterone Urinary Na/K ratio

Electrolyte disorders: Potassium • Hypokalemia – EKG • U waves – Treatment • Restore ECF volume to 2 hyperaldosteronism • PO potassium – Limitations: tolerance • IV potassium – Limitation: 0. 3 meq/kg/hr – Central vs peripheral IV

Hyperkalemia: differential diagnosis • Systemic – Malnutrition • Adrenal – Adrenal overactivity – Congenital adrenal hyperplasia – Primary renin abnormalities • Renal – DKA – Osmotic diuresis

SCENARIO A 15 month child presents with a history of poor feeding and impaired growth. Prenatal and family history is noncontributory. On examination the infant’s height and weight are below the 5 th percentile. The systolic blood pressure is 102 and the pulse is 110. The rest of the examination is normal. Na 138 Cl 114 Bicarbonate 16 What are key features in the history and examination? What studies would you perform? What is your initial therapy? What is your initial diagnosis (es)?

Electrolyte disorders: acid-base Acid load Acute Chronic-Kidney Proximal Chronic-Kidney Distal Lung Reclaim filtered bicarbonate Regenerate Titrated bicarbonate Large frequent doses 1 -3 mmol/kg/day
![Electrolyte disorders • Anion gap • [Na] – {[Cl] + [HCO 3]} • Normal](http://slidetodoc.com/presentation_image/75d34f98117017a80dec1fdde0eb091f/image-134.jpg "Electrolyte disorders • Anion gap • [Na] – {[Cl] + [HCO 3]} • Normal")
Electrolyte disorders • Anion gap • [Na] – {[Cl] + [HCO 3]} • Normal value: 4 -12 • Impact of serum albumin March 17, 2005

Electrolyte disturbances: RTA • Metabolic acidosis – Normal anion gap -- hyperchloremic • Diarrhea • RTA – High anion gap -- normochloremic • MUDPIES or KUSSMAUL • Key entities: – – – DKA Lactic acidosis Uremia Metabolic disease Toxins

Electrolyte disturbances: RTA • Proximal – Low K – Primary – Secondary • • Glycogen storage Wilson’s, fructose intolerance, tyrosinemia PTH, Vitamin D Cystinosis

Electrolyte disturbances: RTA • Distal – Primary – Secondary • Transplant rejection • Drugs: amphotericin, cisplatinum • Collagen vascular disease

Electrolyte disorders: RTA • Assessment – SMAC: Cl– VBG: Bicarbonate – Urine: calcium, citrate – Urine anion gap: unmeasured cation (NH 4+) – Xrays

Electrolyte disturbances: RTA • Treatment • Proximal – Higher doses of bicarbonate – More frequent dosing – Exacerbation of hypokalemia with Rx • Distal – 1 -3 mmol/kg varying with age and diet – 3 doses – Stabilization of K with Rx

Electrolyte disorders: Fanconi’s Syndrome Complete proximal tubule dysfunction RTA Glycosuria Phosphaturia TRP Amino Aciduria

Electrolyte disorders: metabolic alkalosis • Extrarenal/GI loss of K – CF • Vomiting – NG suction – Pyloric stenosis • Distal GI loss of bicarbonate – Chloride diarrhea • Renal – Bartter’s – Gitelman’s – Apparent mineralocorticoid excess (AME)/licorice

Electrolyte disorders: DI • Central • Nephrogenic • Risk of CNS disease – 1/12 (1/3 X ¼) of loss from ECF – Limited access to water – Altered thirst March 17, 2005

Electrolyte disorders: DI • Central – AVP replacement • Nephrogenic – Adequate water intake – Low solute diet – Hydrochlorothiazide

Electrolytes: Pearls There are three pure renal causes of FTT – azotemia, DI, and RTA causes hyperchloremic acidosis Bartter’s and Gitelman’s differ in calcium excretion – high in former low in latter

Thank you GOOD LUCK
- Slides: 145