Metabolic Response to Stress Injury or Surgery Objectives

Metabolic Response to Stress, Injury or Surgery

Objectives • The effects of trauma /Surgery on metabolism • Consequences of the metabolic response • Determination of calorie and protein requirements during metabolic stress

Metabolism. . . ? · · All chemical reactions involved in maintaining the living state of the cells and the organism Metabolism is closely linked to nutrition and the availability of nutrients i. e Nutrition is the key to metabolism. Food provides a variety of substances that are essential for the building and repair of body tissues, and for the efficient functioning of the body

· Metabolism of substrates and micronutrients is altered by trauma. · After trauma, the body’s hormonal situation changes, increasing the demand for energy, proteins and micronutrients. · If nutritional requirements are not recognized and met during starvation or trauma, there may be a loss of body mass, body protein, and impairment or loss of body functions.
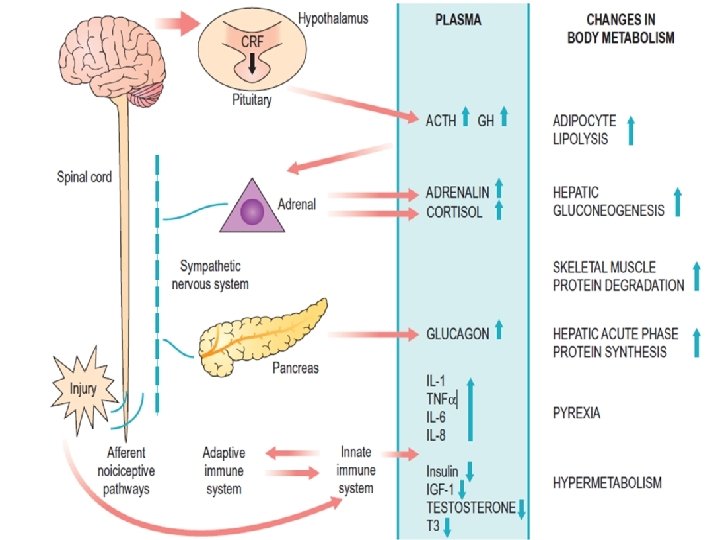

Mediating the Response • The Endocrine System • Pituitary Gland (↑ GH, ↑ ACTH, ) • Adrenal Gland (↑ Cortisol, Aldosterone) • Pancreatic (↑Glucagon, Insulin) • Others (Renin, Angiotensin, Sex hormones, T 4) • The net effect of the endocrine response to surgery is an increased secretion of catabolic

Mediating the Response • Afferent Neuronal impulses from the site of injury Hypothalamus • Efferents to sympathetic Nervous system Adrenal Medulla ↑ catecholamines (tachycardia, hypertension)
")
Mediating the Response • The endothelium, activated leucocytes and fibroblasts produce Cytokines (IL /INF) • These act on their target cells to produce different proteins

Mediating the Response • The Acute Inflammatory Response • Cellular activation • Inflammatory mediators (TNF, IL 1, etc)

Consequences of the Response • Mobilization of substrates

· Trauma/surgery causes major alterations in energy and protein metabolism. · The response to trauma can be divided into the ebb phase and the flow phase. · The ebb phase occurs immediately after trauma and lasts from 24 -48 hours followed by the flow phase. After this, comes the anabolism phase and finally, the fattyreplacement phase.

Phases – Physiological response Injury EBB Hours SHOCK FLOW RECOVERY Days CATAB OLISM BREAKING DOWN ENERGY STORES Weeks ANABO LISM BUILDING UP USED ENERGY

Metabolic Response to Trauma: Ebb Phase • Characterized by hypovolemic shock • Priority is to maintain life/homeostasis Cardiac output Oxygen consumption Blood pressure Tissue perfusion Body temperature Metabolic rate Cuthbertson DP, et al. Adv Clin Chem 1969; 12: 1 -55 Welborn MB. In: Rombeau JL, Rolandelli RH, eds. Enteral and Tube Feeding. 3 rd ed. 1997

· The ebb phase is characterized by hypovolemic shock. · Cardiac output, oxygen consumption and blood pressure all decrease, thereby reducing tissue perfusion. · These mechanisms are usually associated with hemorrhage. · Body temperature drops. · The reduction in metabolic rate may be a protective mechanism during this period of hemodynamic instability.

Metabolic Response to Trauma: Flow Phase • Catecholamines • Glucocorticoids • Glucagon • Release of cytokines, lipid mediators • Acute phase protein production Cuthbertson DP, et al. Adv Clin Chem 1969; 12: 1 -55 Welborn MB. In: Rombeau JL, Rolandelli RH, eds. Enteral and Tube Feeding. 3 rd ed. 1997

Key catabolic elements of flow phase · · Hypermetabolism Alterations in skeletal muscle protein Alterations in Liver proteins Insulin resistance
")
Metabolic Response to Trauma Endocrine Response Fatty Deposits Fatty Acids Liver & Muscle (glycogen) Glucose Muscle (amino acids) Amino Acids

· Endocrine response in the form of increased · catecholamines, glucocorticoids and glycogen, leads to mobilization of tissue energy reserves. These calorie sources include – fatty acids and glycerol from lipid reserves, – glucose from hepatic glycogen (muscle glycogen can only provide glucose for the involved muscle) and gluconeogenic precursors (eg, amino acids) from muscle.

· The response to trauma includes a breakdown of muscle tissue. · This mechanism provides amino acids for gluconeogenesis and for synthesis of proteins involved in immunologic response and tissue repair. · However, this process can lead to a loss of body mass, most notably body protein.

· Prolonged metabolic stress without provision of adequate calories and protein leads to impaired body functions and ultimately malnutrition.
 24 20 16 12 8 4")
Metabolic Response to Trauma 28 Nitrogen Excretion (g/day) 24 20 16 12 8 4 0 10 20 Day Long CL, et al. JPEN 1979; 3: 452 -456 s 30 40

· Previous slide illustrates nitrogen losses in relation to trauma. · With respect to protein, the greater the trauma, the greater the effect on the nitrogen balance. · Similar to metabolic rate, patients experience nitrogen losses according to the severity and duration of the trauma.

Severity of Trauma: Effects on Nitrogen Losses and Metabolic Rate Nitrogen Loss in Urine Major Cirugía mayor Surgery Quemadura Moderate to Severe moderada a grave Burn Severe Sepsis grave Infection Infecci ón Sepsis Cirugía Elective electiva Surgery Basal Metabolic Rate Adapted from Long CL, et al. JPEN 1979; 3: 452 -456

· The graph illustrates that severity of injury correlates to increasing urinary nitrogen loss and increasing energy needs. · Elective surgery being least traumatic and the lowest nitrogen loss in urine, whereas burn results in an increase in basal metabolic rate and urinary loss of nitrogen.

Estimation of energy requirements · There a wide variety of methods for estimating energy requirements. · Common methods include indirect calorimetry and the Harris-Benedict Equation.

· Indirect calorimetry is based on calculating heat production by measuring oxygen consumed and carbon dioxide produced, through analysis of exhaled gas or use of pulmonary catheters.

· The Harris-Benedict Equation calculates basal energy requirements for healthy people · It has also been applied to sick patients through the use of correction factors for stress and activity. · The simplest estimate of adequate energy intake for patients in metabolic stress is the “rule of thumb” of 25 -30 kcal/kg body weight per day.

Determining Calorie Requirements • • • Indirect calorimetry Harris-Benedict x stress factor 25 -30 kcal/kg body weight /day x activity

Metabolic Response to Starvation and Trauma: Nutritional Requirements Injury Stress Factor Minor surgery 1. 00 – 1. 10 Long bone fracture 1. 15 – 1. 30 Cancer 1. 10 – 1. 30 Peritonitis/sepsis 1. 10 – 1. 30 Severe infection/multiple trauma 1. 20 – 1. 40 Multi-organ failure syndrome 1. 20 – 1. 40 Burns 1. 20 – 2. 00 Activity Factor Confined to bed 1. 2 Out of bed 1. 3 Example: Energy requirements for patient with cancer in bed = BEE x 1. 10 x 1. 2 ADA: Manual Of Clinical Dietetics. 5 th ed. Chicago: American Dietetic Association; 1996 Long CL, et al. JPEN 1979; 3: 452 -456

Macronutrients requirements during Stress Carbohydrate • • • At least 100 g/day needed to prevent ketosis Carbohydrate intake during stress should be between 30%-40% of total calories Glucose intake should not exceed 5 mg/kg/min Barton RG. Nutr Clin Pract 1994; 9: 127 -139 ASPEN Board of Directors. JPEN 2002; 26 Suppl 1: 22 SA

Macronutrientes during Stress Fat • • • Should provide 20%-35% of total calories Maximum recommendation for intravenous lipid infusion: 1. 0 -1. 5 g/kg/day Monitor triglyceride level to ensure adequate lipid clearance Barton RG. Nutr Clin Pract 1994; 9: 127 -139 ASPEN Board of Directors. JPEN 2002; 26 Suppl 1: 22 SA

Macronutrientes during Stress · Dietary fat should provide between 20 - 35% of total calories. Maximum recommended infusion rate when administering intravenous lipids is 1. 0 -1. 5 g/kg/day. Serum triglyceride levels in stressed patients should be monitored to ensure adequate lipid clearance.

Macronutrients during Stress Protein • • Requirements range from 1. 2 -2. 0 g/kg/day during stress Comprise 20%-30% of total calories during stress Barton RG. Nutr Clin Pract 1994; 9: 127 -139 ASPEN Board of Directors. JPEN 2002; 26 Suppl 1: 22 SA

· Protein requirements increase during metabolic stress and are estimated at between 1. 2 -2. 0 g/kg/day, or approximately 20% to 30% of the total calorie intake during stress.

Determining Protein Requirements for Hospitalized Patients Stress Level Calorie: Nitrogen Ratio Percent Potein / Total Calories Protein / kg Body Weight > 150: 1 Moderate Stress 150 -100: 1 Severe Stress < 100: 1 < 15% protein 15 -20% protein > 20% protein 0. 8 g/kg/day 1. 0 -1. 2 g/kg/day 1. 5 -2. 0 g/kg/day No Stress

· Calorie-to-nitrogen ratios can be used to prevent lean body mass from being utilized as a source of energy. Therefore, in the non-stressed patient, less protein is necessary to maintain muscle as compared to the severely stressed patient.

Micronutrients · Micronutrients, trace element, vitamin, and mineral requirements of metabolically stressed patients seem to be elevated above the levels for normal healthy people. · There are no specific dosage guidelines for micronutrients and trace elements, but there are plausible theories supporting their increased intake. · The following slide lists some of these nutrients along with the rationale for their inclusion.

Key Vitamins and Minerals Vitamin A Vitamin C B Vitamins Pyridoxine Zinc Vitamin E Folic Acid, Iron, B 12 Wound healing and tissue repair Collagen synthesis, wound healing Metabolism, carbohydrate utilization Essential for protein synthesis Wound healing, immune function, protein synthesis Antioxidant Required for synthesis and replacement of red blood cells

Role of Glutamine in Metabolic Stress • • Considered “conditionally essential” for critical patients Depleted after trauma Provides fuel for the cells of the immune system and GI tract Helps maintain or restore intestinal mucosal integrity Smith RJ, et al. JPEN 1990; 14(4 Suppl): 94 S-99 S; Pastores SM, et al. Nutrition 1994; 10: 385 -391 Calder PC. Clin Nutr 1994; 13: 2 -8; Furst P. Eur J Clin Nutr 1994; 48: 607 -616 Standen J, Bihari D. Curr Opin Clin Nutr Metab Care 2000; 3: 149 -157

· Glutamine is one of the few nutrients included in the category of conditionally-essential amino acids. · Glutamine is the body’s most abundant amino acid and is involved in many physiological functions. Plasma glutamine levels decrease drastically following trauma. · It has been hypothesized that this drop occurs because glutamine is a preferred substrate for cells of the gastrointestinal cells and white blood cells. Glutamine helps maintain or restore intestinal mucosal integrity.

· Arginine is also considered a conditionally essential amino acid.
- Slides: 41