Metabolic and Respiratoric Disturbance of AcidBase Balance Acidbase

Metabolic and Respiratoric Disturbance of Acid-Base Balance

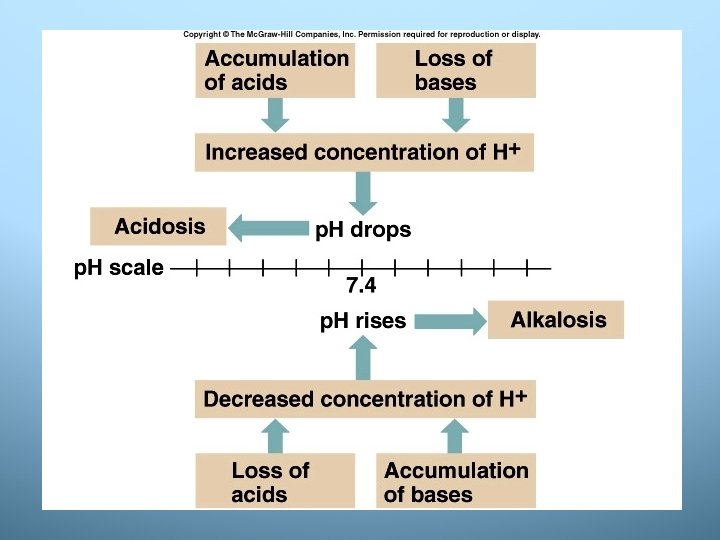
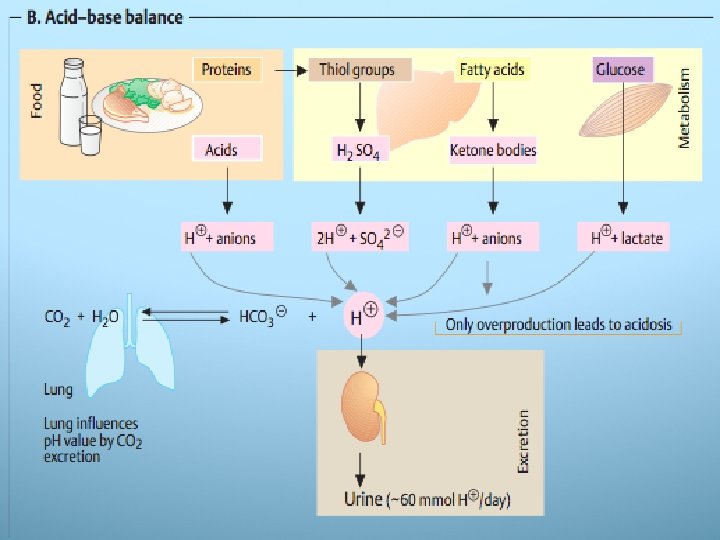
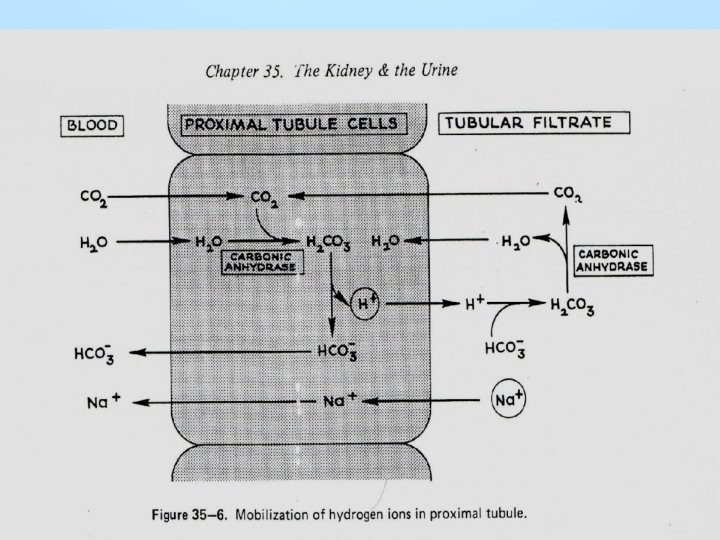
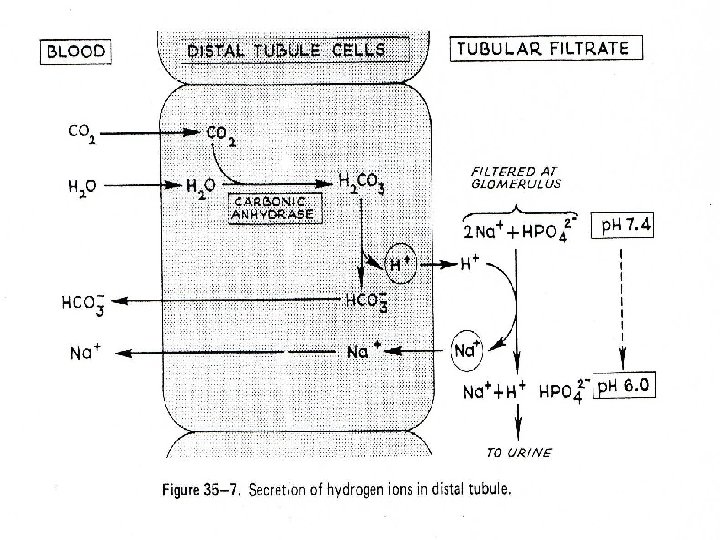
Acid-base balance • The regulation of hydrogen ion – more Hydrogen ions acidic solution lower p. H, vice versa • H+ be added to body fluids from 3 sources: – formation of H 2 CO 3 and some will dissociate into H+ and HCO 3– catabolism of organic substances – dissociation of organic acids on the metabolism intermedia (i. e. metabolism of fat) • The kidneys actively secrete H+ through 3 mechanism: – Na+/H+ exchange – reclamation of bicarbonate – production of ammonia and excretion of NH 4+

Control of acid-base There are 3 compensatory mechanism of acid-base in the body: 1. The bicarbonate-carbonic acid buffer system in plasma instaneously. 2. Respiratory mechanism take several minutes to hours 3. Renal mechanism take several hours to days
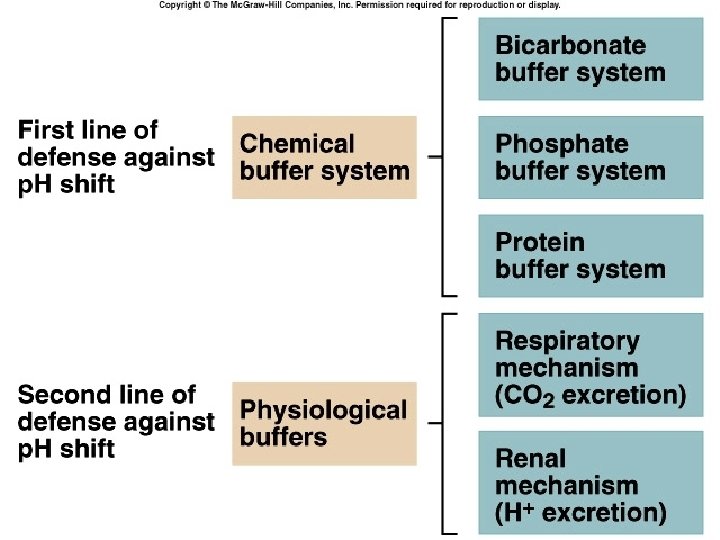

1. Buffer system • The p. H value is kept constant by buffer system that cushion minor disturbances in the acid base balance • Buffer pairs: weak acid and a base • Bicarbonat buffer: – sodium bicarbonate (Na. HCO 3) and carbonic acid (H 2 CO 3) maintain in 20 : 1 = HCO 3 - : H 2 CO 3 Buffer Acid Conjugate base Main buffering action Hemoglobin Proteins HHb HProt Hb. Prot- Phosphate buffer Bicarbonate H 2 PO 4 - HPO 42 - erythrocytes Intracellular, extracellular Intracellular, renal CO 2 H 2 CO 3 HCO 3 - extracellular
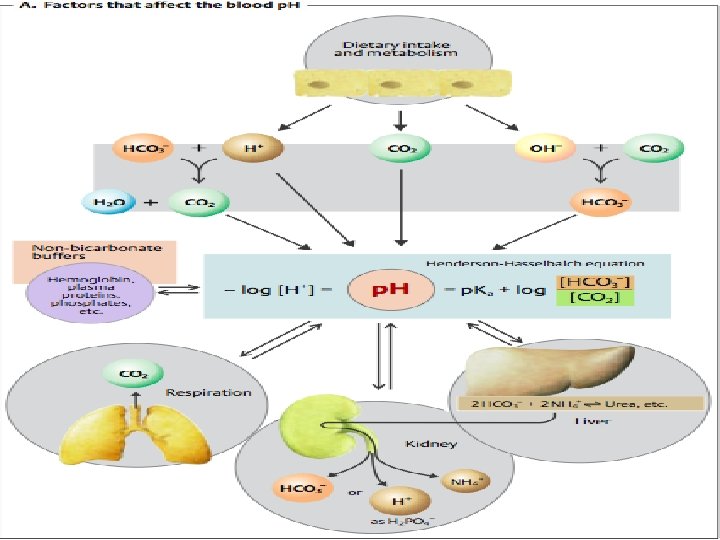

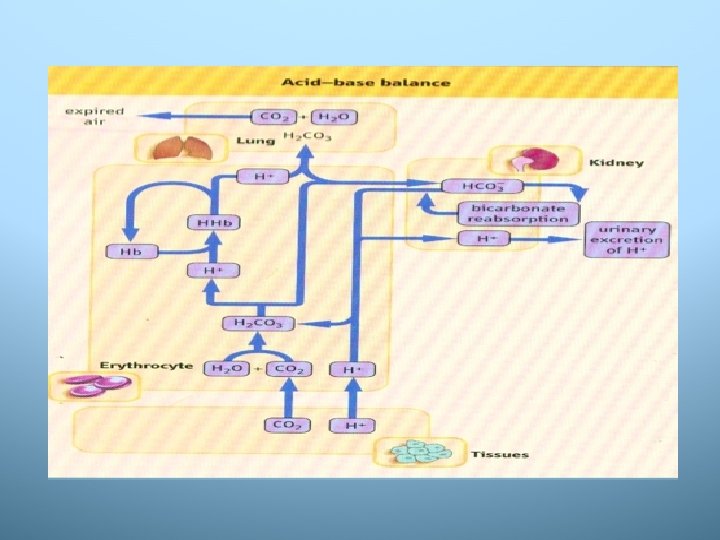
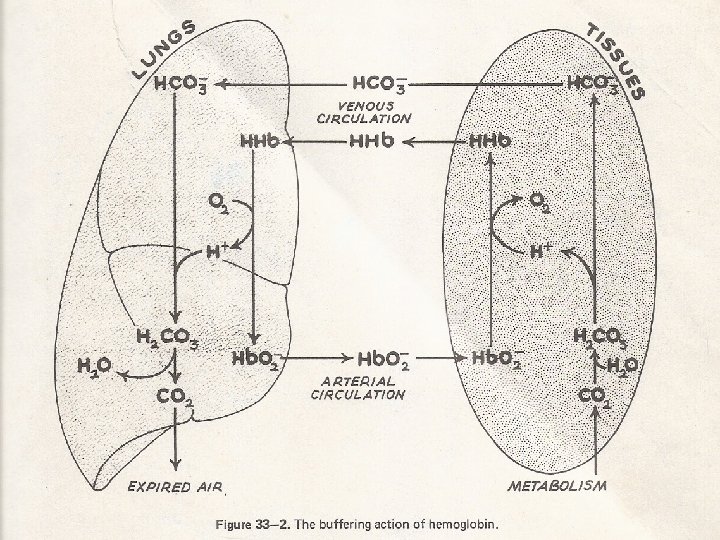
2. Respiratory mechanism • Lung: control exchange of CO 2 and O 2 between the blood and the external atmosphere • Only work with volatil acid (H 2 CO 3) • p. H in the body can be adjusted by changing rate and depth breathing • CO 2 + H 20 H 2 CO 3 H+ + HCO 3 -

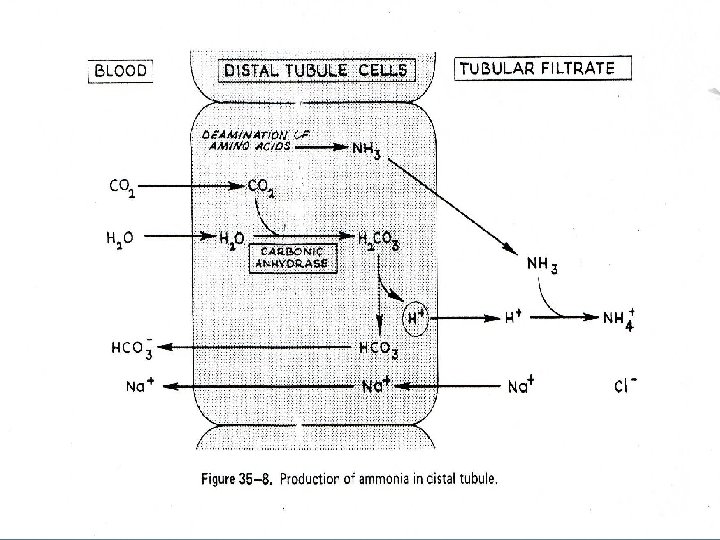
3. Renal mechanism • Most effective regulator of p. H • If kidneys fail p. H balance fails • The kidney help through 3 mechanism: – The recovery of bicarbonate, which is filtered into the tubules – The excretion of hidrogen ions against the gradient to acidify the urine – The excretion of ammonium ion (NH 4)+

Plasma bicarbonate concentration • Is controlled by kidneys and erythrocytes • Erythrocytes and renal tubular cells contain a high activity of zinc-containing enzyme (carbonic anhydrase = carbonic dehydrase) catalysis the conversion of CO 2 + H 2 O H 2 CO 3 H+ + HCO 3 • Kidneys regulate plasma HCO 3 - by: – filtered HCO 3 - is completely reabsorbed by the tubulus – HCO 3 - is regenerated in the distal tubule to replace that which has been utilized by the presence of non volatil acids within extracellular fluids as a consequence of metabolic processes

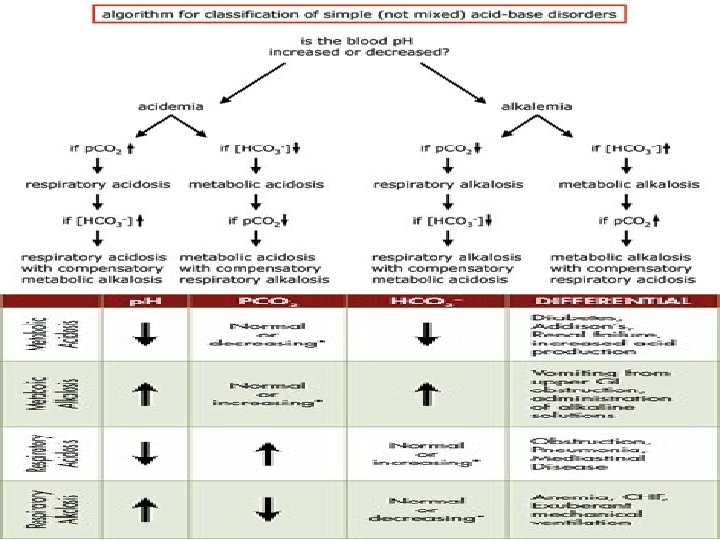
Respiratory and metabolic compensation in acid-base disorder • Normal p. H plasma 7, 4: ratio HCO 3 - = 20 CO 2 • Classification of the clinical disorders of the acid – base balance: 1. Respiratory acidosis 2. Respiratory alkalosis 3. Metabolic acidosis 4. Metabolic alkalosis

1. Respiratory acidosis: p. H decrease • Caused by an increase in carbonic acid relative to bicarbonate impairs respiration (pneumonia, emphycema, congestive failure, asthma, or in depression of the respiratory center as by morphine poisoning) • Compensatory: increase in bicarbonate reabsorption and increase the excretion of H+ by the kidney • Symptom: breathlessness, lethargy and disorientation, tremors, convulsion, coma
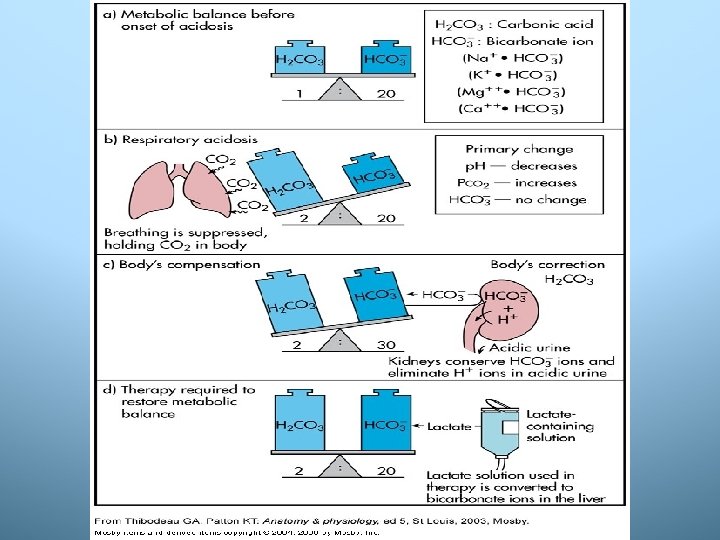

Kompensasi tubuh terhadap asidosis respiratorik adalah: • Sistem buffer darah: peningkatan H 2 CO 3 dalam plasma segera diubah dalam sel darah merah dengan bantuan enzim karbonat anhidrase menjadi HCO 3 -, kemudian dikeluarkan kembali ke dalam plasma untuk meningkatkan garam bikarbonat sehingga menjadi seimbang. • Sistem paru-paru: tergantung pada berat ringannya gangguan dan kemampuan individu yang tersisa, peningkatan kandungan H 2 CO 3 berusaha merangsang pusat pernafasan di hipotalamus untuk hiperventilasi. • Sistem ginjal: meningkatkan kadar HCO 3 - dengan cara ginjal menghemat pengeluaran HCO 3 - dan mengeliminasi ion H+ dari tubuh lewat urine yang lebih asam. Untuk tujuan ini, ginjal melakukan: • ekskresi ion H+, retensi ion Na+ di tubulus proksimal • ekskresi ion H+, retensi ion Na+ di tubulus distal • ekskresi ion H+, retensi ion Na+ serta pembentukan ammonia di tubulus distal Jika usaha kompensasi berhasil dinamakan asidosis resiratorik terkompensasi. Sebaliknya jika tidak dapat dikompensasi dinamakan asidosis respiratorik tidak terkompensasi.

2. Respiratory alkalosis: p. H increase * Caused by hyperventilation, there is a decrease in the carbonic acid fraction (hypocapnea) with no corresponding change of bicarbonate * Most common acid-base imbalance * Occurs in pulmonary disease and congestive heart, fever, anemia, chirrhosis * Compensatory: decreases bicarbonate reabsorption (excreting bicarbonate) and retaining H+ by the kidneys


Kompensasi tubuh terhadap alkalosis respiratorik adalah: • Sistem buffer darah: kelebihan ion HCO 3 - dimasukkan ke dalam sel darah merah untuk diubah menjadi H 2 CO 3 dengan bantuan enzim karbonat anhidrase. Asam karbonat yang terbentuk dikeluarkan ke dalam plasma sehingga keseimbangan dapat ditingkatkan. • Sistem paru-paru: tergantung pada berat ringannya gangguan yang dialami dan kemampuan paru-paru yang tersisa, jika masih memungkinkan berusaha meningkatkan kandungan asam karbonat melalui pelambatan ventilasi (hipoventilasi). • Sistem ginjal: mengurangi kadar HCO 3 - dengan cara ginjal menghemat pengeluaran ion H- dan mengeliminasi ion HCO 3 - dari tubuh lewat urin sehungga menjadi basa. Untuk tujuan ini, ginjal melakukan: • ekskresi ion H+, retensi ion Na+ di tubulus proksimal • ekskresi ion H+, retensi ion Na+ di tubulus distal • ekskresi ion H+, retensi ion Na+ serta pembentukan ammonia di tubulus distal Jika usaha kompensasi berhasil dinamakan alkalosis resiratorik terkompensasi. Sebaliknya jika tidak dapat dikompensasi dinamakan alkalosis respiratorik tidak terkompensasi.

3. Metabolic acidosis: p. H decrease u. Caused by decreasing of bicarbonate concentration in plasma u. Occurs in uncontrolled diabetes with ketosis, excessive of vomiting or diarrhea, renal disease, poisoning by an acid salt u. Symptom: headache, lethargy, nausea, vomiting, diarrehea u. Compensatory: through hyperventilation (increase ventilation), renal excretion of H+ if possible (H+ into cells, K+ out of cell)
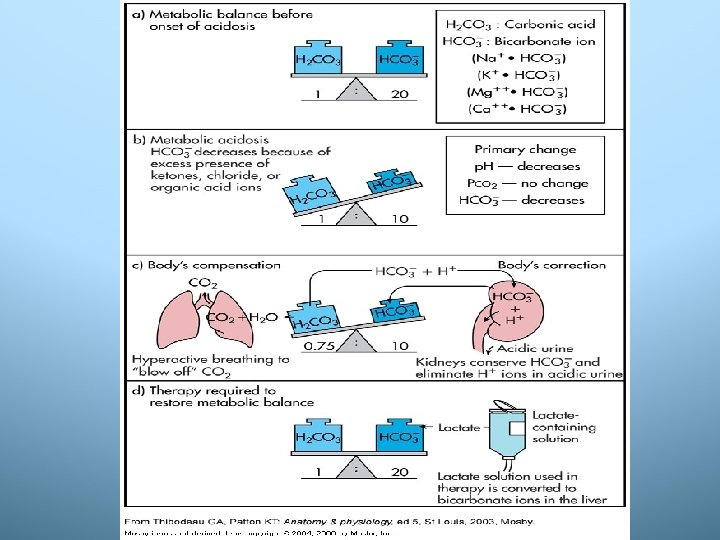

Kompensasi tubuh terhadap asidosis metabolik adalah: • Sistem buffer darah: H 2 CO 3 melepaskan H+ ke sistem dapar lain supaya kandungan garam bikarbonat dapat ditingkatkan. • Sistem paru-paru: H 2 CO 3 meningkat sehingga terjadi peningkatan p. CO 2 yang mengakibatkan pusat pernafasan di hipotalamus dirangsang sehingga terjadi hiperventilasi. Melalui cara ini diharapkan kadar asam karbonat dapat menurun. • Sistem ginjal: ginjal meningkatkan garam bikarbonat secara retensi Na+ di tubulus proksimal dan distal, sehingga kandungan garam bikarbonat meningkat, dan mengeliminasi H+ dari tubuh lewat urin yang lebih asam. Jika usaha kompensasi berhasil dinamakan asidosis metabolik terkompensasi. Sebaliknya jika tidak dapat dikompensasi dinamakan asidosis metabolik tidak terkompensasi.

4. Metabolic alkalosis: p. H increase • Caused by increasing of bicarbonate concentration in the plasma with no change or relatively smaller change in the carbonic acid fraction. • Occurs in the ingestion of large quantities of alkali (ulcer disease), pyloric stenosis, excess vomiting , severe dehydration. • Symptom: hyperactive reflect, tetany, atrial tachycardia, respiration slow and shallow • Compensatory: to a decrease in the ventilation rate of carbonic acid (the body responds by depressing the respiratory center hypoventilation increases the retention of carbonic acid)
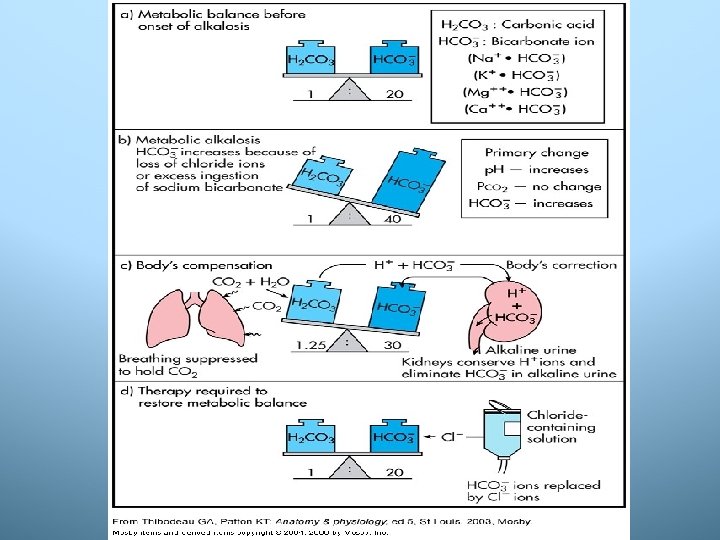

Kompensasi tubuh terhadap alkalosis metabolik adalah: • Sistem buffer darah: garam bikarbonat yang meningkat berusaha menerima ion H+ dari sistem buffer lainnya untuk meningkatkan asam karbonat, sambil menurunkan garam bikarbonat. • Sistem paru-paru: meningkatkan asam karbonat untuk mengimbangi kenaikan komponen garam karbonat dengan meretensi CO 2 melalui penekanan pusat pernafasan, sehingga frekuensi pernafasan diperlambat (hipoventilasi). • Sistem ginjal: berusaha mengurangi ekskresi ion H+ sehingga ekskresi garam bikarbonat meningkat, proses pengasaman urin berkurang (mengeliminasi ion HCO 3 - dari tubuh melalui urin), pembentukan ammonia di tubulus distal ditekan. Jika usaha kompensasi berhasil dinamakan alkalosis metabolik terkompensasi. Sebaliknya jika tidak dapat dikompensasi dinamakan alkalosis metabolik tidak terkompensasi.
 • Function: –")
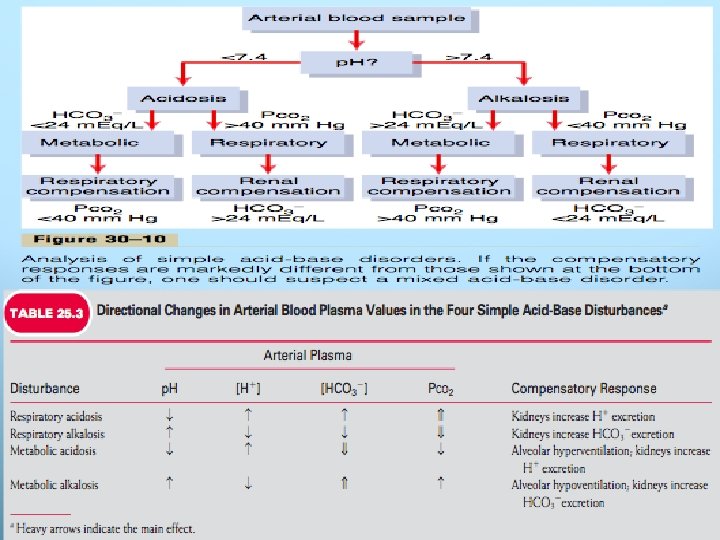
Blood Gas Analysis • Using arterial blood ABG (Arterial Blood Gas) • Function: – To determine if patients is well oxygenated – To determine the patients acid-base The relationship between Pa. O 2 and Sa. O 2

ABG Interpretation • p. H • HCO 3 (The primary change in HCO 3 metabolic) • PCO 2 (The primary change in CO 2 respiratory)

ABG Interpretation Acidemic & Alkalemic refer to the p. H change only. Acidosis & Alkalosis refer to entire clinical and biochemical picture If the p. H changes, compensation occur Metabolic compensation occurs for a metabolic acidbase disturbance and vice versa, and in such cases PCO 2 & HCO 3 move in the same direction
- Slides: 35