Mentoring the Mentor Stuart White DC DACBN CCN

Mentoring the Mentor Stuart White, DC, DACBN, CCN Whole Health Associates 1406 Vermont Houston, Texas 77006 713/522 -6336 stuartwhite@wholehealthassoc. com www. wholehealthassoc. com 1 www. doctorofthefuture. org

Mentor goals: Ò Ò Ò To declare what is possible and establish a commitment to that possibility Address personal and professional barriers limiting the ability to serve Evolution of vision/mission/ethics that drive success Create immediate action steps to apply learning and growth Construct the round table of applied trophologists 2

Mentoring the mentor: Ò Ò Ò Who are the mentors? – Practitioners Who are we mentoring? – Patients and GAP What’s the purpose? – Optimized life How does it work? – Whatever you learn you teach someone else (anyone else) Who’s is included? – Self selection, you pick yourself 3

Mentoring the mentor: Ò Ò Each participant attends monthly teleconferences (1 hour in duration, 4 th Thursday of month) creating a round table discussion/exploration of the dynamics and details of a nutrition-based holistic practice Each participant chooses how to convey the notes and information to their world and community – no information squandering 4

Review - Distinguish yourself • It is more apparent why people are choosing alternative health care professionals who specialize in a functional approach • No matter you specialty or technique you must distinguish yourself as an expert – people are just seeking to understand they need you to do so • Typically in the healthcare industry people are receiving shallow answers that leave them puzzled with the mystery of “Why is this happening to me? ” and “ What can I do about it? ” • Trends research over 10 years ago identified a number of factors essential to being successful in the nutritional field – one of those was establishing yourself as an expert 5

Review - Explanation as hope • The practitioner’s ability to explain health issues and therapeutic outcomes creates an inflation of understanding in the patient which feels like hope • Today in the professional world there is so much avoidance of ‘giving false hope’ that often we end up offering little hope at all • I propose another model that bolsters hope and expectation and subsequently practices accountability as to whetherapeutic endeavors are achieved or not • As long as the hope that has been instilled is revisited and acknowledged as being accomplished or not the betrayal of false hope can be avoided • So as an example, if a practitioner was describing the potential for nutritional intervention through supplements and diet modification to improve the lipid profile, then s/he would need to revisit to success or failure of the experiment within a reasonable period of time • Our community is starving for legitimate hope, as a starting place, as empowerment to begin, as an idea to act upon • There is genius in hope 6

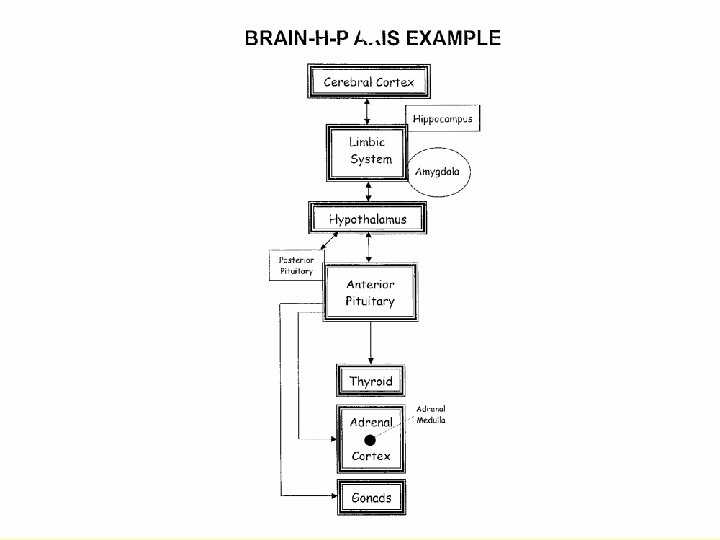
Mentor Considerations HPA Axis and Immune Cytokine Signaling

Seven Pillars Unified Mechanisms of Health Promoting Physiology

7 Pillars of Healing 7 Unified Mechanisms of Health f. Endocrine/Hormonal f. Glycemic Management fp. H Bioterrain f. Immuno-Inflammatory f. Circulatory Status f. Digestive Potency f. Cellular Vitality 9

Endocrine Hormonal Cellular Vitality Glycemic Management Normal p. H Miracle Digestive Potency Bioterrain Minerals Circulatory Immune Status Inflammatory

Eternal truth Fulfillment is not a goal to achieve, But always a byproduct of sacrifice

1 -The Endocrine Axis f. Most powerful system to activate the rest of body f 7 glandular levels f. PMG’s first, lifestyle modification second, herbs third, HRT last 12

#1 Core Physiologic Principle Stressors Hormonal/endocrine adaptation Glandular fatigue & imbalance Depletion of organ reserve and nutrient/mineral substrates Reduced homeostatic mechanisms Stress hyper/hypo reactivity Altered psychoneuroimmunologic mechanisms Nutrient repletion – target fortification Symptoms – physical/personality modulation Increased glandular strength/resilience Disease diagnosis – chronic progression Restored adaptive mechanisms Medical Intervention – Drugs & Surgery Increased organ reserve – repletion of substrates Death Enhanced physiology/personality 13

15
 Hypothalmex/us(1, 1) Black Currant Seed(1, 1) 16")
Symplex F/M(3, 3) Hypothalmex/us(1, 1) Black Currant Seed(1, 1) 16

The Stress Model § The HPTA is at the heart of the body’s ability to respond to the environment § Cortisol elevation is the result of Corticotrophin Releasing Hormone (CRH) arising from the parvocellular neurons of the paraventricular nucleus (PVN) - this is the ‘master’ stress hormone released in response to the perception of stress § Stressful stimuli are generalized as: § § Physical – pain, trauma, infection, hypotension, exercise, hypoglycemia Psychological – bereavement, fear, personal loss, anger (the perception that God is not in control – something is wrong) § CRH is released into the portal circulation of the Median Eminence and is carried by venous blood to the corticotroph cells of the anterior pituitary where it binds to the cell surface receptors stimulating the release of Adrenocorticotropic Hormone (ACTH) § ACTH reaches the adrenal cortex stimulating the synthesis of Cortisol (glucocorticoid) and also androgenic hormones like androstenidione and DHEA (both may convert 17 to testosterone 17 and DHT in peripheral tissues)

The Stress Model § Cortisol maintains blood glucose during stressful ‘fight or flight’ challenges so that as more metabolic fuel is consumed a critical amount is maintained for brain function and to support the activated survival organs such as the heart, lungs, and skeletal muscle with renewable supply of fuel § Cortisol also participates with Aldosterone (mineralocorticoid) in driving sodium reabsorption from the renal tubules conserving electrolytes and water within the vasculature to provide blood and perfusion pressures to vital organs § Cortisol concentrations rise until it effects negative feedback on the CRH neurons and the pituitary corticotrophs to return blood levels to normal preventing prolonged elevations of CRH, ACTH and cortisol § Chronic stress and maladapted responses to stress alters this mechanism and causes longterm cortisol dysregulation and even ‘cortisol resistance’ 18 18

Cortisol Activation Hypothalamus Paraventricular Nuclei Median Eminence Neurohypophysis Parvocellular neurons of the Paraventricular Nuclei release CRH in response to perceived stress Corticotrophin Releasing Hormone Cortisol elevation provides negative feedback to paraventricular nuclei decreasing CRH Anterior Pituitary “Corticotrophs” ACTH Adrenocorticotropic Hormone Promotes Aldosterone release “mineralocorticoid” Blood/Brain Cortisol Resistance Barrier Adrenal Cortex Cortisol Resistance Adrenal Complex Tyrosine Reduce cortisol resistance Cortisol “Glucocorticoid” Androgenic hormones Androstenidione, testosterone, DHT, progesterone 19

Modulating Cortisol § § § Symplex, Hypothalmex/us – HPA general support Androgen up-regulation Adrenal Complex – 2 -4/day licorice & rehmannia Allergen removal Drenamin – 6/day Dessicated Adrenal – 2 -4/day for acute activation Eleuthero – 2 -4/day Withania Complex – 2/day Vitanox 2 -4/day Detoxification Change of thinking Neuro-emotional release 20 20
 has exploded on the scene and represents")
Modulating Cortisol § Adrenal Complex (1 -2) has exploded on the scene and represents another Medi. Herb homerun § Introduced in 02/09 it has backordered multiple times as Americans have grasped its value as an idea whose time has come § Licorice (250 mg of 7: 1 extract) contains 25 mg of glycyrrhizin the active component that assists cortisone (a less active storage form of cortisol) to convert to cortisol (more active form) § Rehmannia (150 mg of 5: 1 extract) provides immune modulation § Expect modulation in WHR, concentration, sleep quality, reduced muscle tension, relaxability, reduced anxiety 21 § Contraindicated when hypertension results 21

Gut Brain Interface 22

The Bidirectional Gut-Brain Axis Grenham S, Clarke G, Cryan JF, Dinan TG. Brain-gut-microbe communication in health and disease. Front Physiol. 2011; 2: 94. Epub 2011 Dec 7. Pub. Med PMID: 22162969; Pub. Med Central PMCID: PMC 3232439 23

Lymph Tissue • 70% of our immune cells reside in the GI tract. • The development of the intestinal immune system is largely dependent upon exposure to microorganisms. • The gut produces ¾ of the body’s neurotransmitters. • The gut has greater metabolic activity than the liver. Forsythe P, Sudo N, Dinan T, Taylor VH, Bienenstock J. Mood and gut feelings. Brain Behav Immun. 2010 Jan; 24(1): 9 -16. Ochoa-Repáraz J, Mielcarz DW, Begum-Haque S, Kasper LH. Gut, bugs, and brain: role of commensal bacteria in the control of central nervous system disease. Ann Neurol. 2011 Feb; 69(2): 240 -7. Korecka A, Arulampalam V. The gut microbiome: scourge, sentinel or spectator? J Oral Microbiol. 2012; 4. 24

Microbiota Regulate HPA-Axis Development • Commensal microbiota regulate the development of the HPA axis. • “The series of events in the gastrointestinal tract following postnatal microbial colonization can have a long-lasting impact on the neural processing of sensory information regarding the endocrine axis. ” • This concept, based on in vivo findings [in mice], provides evidence of a novel link between indigenous microorganisms and the nervous system and shows a new aspect of the brain-gut axis. Sudo N, Chida Y, Aiba Y, Sonoda J, Oyama N, Yu XN, Kubo C, Koga Y. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J Physiol. 2004 Jul 1; 558(Pt 1): 263 -75 25

Commensal Microbiota Drives Immune Homeostasis • This tissue has the dual task of selectively absorbing nutrients from the intestinal lumen, while preventing microbial entry, infection, or immune activation. • We are so focused on the immune system responding to things, that we forget that 99. 9% of the time, its job is NOT to respond to things. “The gut handles more antigenic material in a single day than the rest of the immune system processes its entire lifetime. ” Michael Ash Handley C. Should acquaintance be forgot… EMBO Reports Vol 5, No 12, 2004 Arrieta MC, Finlay BB. The commensal microbiota drives immune homeostasis. Front Immunol. 2012; 3: 33. 26

A Closer Look Commensal and pathogenic microorganisms Microvillar Extension Antimicrobial peptides Glycocalyx M Cell IEC Nucleus Nucleus DC Peyer’s Patch Lymphoid Follicle Transcytosed microbes are acquired by DCs which activate adaptive immune response Direct sampling of microbial antigen in lumen Artis D. Epithelial-cell recognition of commensal bacteria and maintenance of immune homeostasis in the gut. Nat Rev Immunol. 2008 Jun; 8(6): 411 -20. 27

Paracellular Transport Artis D. Epithelial-cell recognition of commensal bacteria and maintenance of immune homeostasis in the gut. Nat Rev Immunol. 2008 Jun; 8(6): 411 -20. 28

Transcellular Pathways Degradative route 90% Non-degradative route <10% 29

The Gut in Action Intestinal lumen Epithelium Lamina propria Artis D. Epithelial-cell recognition of commensal bacteria and maintenance of immune homeostasis in the gut. Nat Rev Immunol. 2008 Jun; 8(6): 411 -20. 30

Just the Right Balance Ma cro Antigen Phagocytosis pha ge on Pathogen/food-derived lipid/protein/nucleic acid r rfe e t In s lam nf e kin to TLR 4/CD 14/MD 2 ^^^^^ Innate immunity y yc B cell or at m Humoral adaptive immune response Th 2 Cell-mediated adaptive immune response Il-4 I Differentiation IL-10 T cell (Th 0) DC Ma TGF-β cro IL-1β Antigen presentation IFN-γ NK cell Treg IL-12 Th 1 IFN-γ IL-6 TNF-α pha ge IL-8 Thomas S, Przesdzing I, Metzke D, Schmitz J, Radbruch A, Baumgart DC. Saccharomyces boulardii inhibits lipopolysaccharide-induced activation of human dendritic cells and T cell proliferation. Clin Exp Immunol. 2009 Apr; 156(1): 78 -87 31

TJ Disassembly Resulting in Unremitting Immune Activation via Leaky Gut Fasano A. Leaky gut and autoimmune diseases. Clin Rev Allergy Immunol. 2012 Feb; 42(1): 71 -8. 32
 or food antigens (gluten, casein) through")
Leaky Gut’s One-Two Punch Translocation of microbial (LPS) or food antigens (gluten, casein) through gut O&NO damage Antibodies confuse self with pathogenic antigens (antigen mimicry) Antibodies and autoimmunity Leaky gut Local and system inflammation Maes M, Kubera M, Leunis JC. The gut-brain barrier in major depression: intestinal mucosal dysfunction with an increased translocation of LPS from gram negative enterobacteria (leaky gut) plays a role in the inflammatory pathophysiology of depression. Neuro Endocrinol Lett. 2008 Feb; 29(1): 117 -24. 33

Food Allergens 34

Determining Food Allergies Blood type sensitivities Eat For Your Blood Type, D’Amatto Most food allergies are delayed sensitivity reactions – difficult to objectively determine § Elisa Act lymphocyte response assay Dr. Russell Jaffe § § Serammune Labs, Virginia, 800/525 -7372 Elimination is the most accurate and labor intensive - 2 week elimination then reintroduce and watch for 4 days for reactions § Histaminic Reactions (rash, red eyes, serous secretions) vs. Immune Activity (fever, catarrhal, lymphatic congestion, aching) § Basic 4 allergies that most complicate healing process – wheat (gluten), corn, soy, milk (casein) § – Additionally suspect chocolate, peanuts, tomatoes, 35 beef 35

Food Allergies – Now & Later Immediate response within hours or next day Delayed responset 2 -7 days later Histaminic Immunological – viral, bacterial, parasitic Red, burning eyes, serous secretions (clear) Colds & Flu – WBC mediated response Tiredness, sleepiness Achiness Headaches Catarrhal, phlegm (colored) Mood changes, irritability Fever Rashes, hives Eczema Nausea, cramps, diarrhea Emesis Loss mental accuity Elevated C-reactive protein, SED rate, AA: EA ratio 36 36

Allergic Events schematic Tissue/cell structures Blood/lymph fluids Infectious process Irritation leading to infestation Viron Gut lumen Gut lining Allergens Foreignness Immune 37 response 37

Generalization of allergen § Milk allergy is primarily casein protein intolerance commonly seen in respiratory and atopic symptoms § Wheat allergy is primarily a gluten protein intolerance commonly effecting GI symptoms and hyper tension & siderosis § Corn allergy is primarily a zein protein intolerance commonly effecting neurological symptoms § Soy allergy is more acquired and therefore can be unlearned commonly effecting acne rosacea and paranasal rashes § Zypan or Betaine HCL (2 -3/meal) will reduce food allergen effects 38 38
: 117")
Plenty of Mediators to Measure Maes M et al. Endocrinol Lett. 2008; 29(1): 117 -124; Haroon E et al. Neuropsychopharmacology. 2012; 37(1): 137 -162. 39

Immune Activation ”Disease Genesis & Perpetuation” Many nutrients & botanicals inhibit the activation of NF-Kappa. B inflammatory gene activation. Omega 3 EFA’s & GLA Vitamin D Grape Seed Extract Propolis Curcumin/Turmeric Resveratrol Lipoic Acid Cholagogues Green Tea Vitamin C Complex Rosemary

Immuno-inflammatory Influence 41

Innate & Acquired Immunity § Primary roles of the healthy immune system are: • Identify potentially injurious and infectious substances • Distinguish self antigens (non-threatening) from non-self (threatening) • Assess the potential level of threat posed by infectious, toxic, or non-self antigens • Mount a response that is appropriate to the level of threat • Repair any damage that ensues from adversarial encounters § Too much response = inflammatory cascades § Too little response = tolerance of danger § WBC is optimal 6 -8, outside optimal range may suggest acute or chronic immune burden, under 4 indicates bone marrow fatigue 42

Immune System – 2 Parts § Generally recognized that there are 2 parts of the immune system § § Innate Immune System – Inborn initial response to eliminate microbes and infections, immediately or within hours – it is not in any locale or organ, it is in the WBC » Each cell is equipped with different mechanisms that allow it to attack and eliminate pathogens from the body demonstrating immune versatility » Non-specific defense against pathogens, activates the complement system of inflammatory response » Identifies self vs. non-self, complement system triggers inflammation and identifies foreign substances, and activates the adaptive immune system – Innate Immune Cells include: » Mast Cells » Natural Killer Cells » Phagocytes – Monocytes, Macrophages, Dendritic cells » Ranulocytes – Neutrophils, Eosinophils, Basophils Adaptive Acquired Immune System – Learned response precisely addressing threat requiring 5 -7 days for adaptive immune modulation to reach full activity and specific lymphocyte presence » Results in TH 1 cellular phagocytosis or TH 2 humoral antibodies » TH 1 responds to living things bacteria, fungus, virus » TH 2 responds to non-living things (and parasites) including food, pollens, bad fats, heavy metals 43 43

Common TH 1 & Th 2 Cytokines § TH 1 § § § TH 2 § § Il-12 IFN – gamma TNF – alpha IL-2 GM – CSF IL-4 IL-5 IL-10 IL-13 § IL-1 and IL-6 (and others) can show both TH 1 and Th 2 influences 44 44

Efflux pumps and bacteria § Milk thistle and Berberine have been found to inhibit the active efflux pump in certain bacteria (Staph) and thus inhibit the germ’s resistance to remediation by drugs and theoretically host immune response as well 45 45

Cytokines – Immune Messages § Immune response results in the release of cytokines meant to direct local and distant immune function § These cytokine messenger molecules also drive HPA status and thus determine global brain status § Cytokines subsequently cause the release of WBC inflammatory mediators to direct the inflammatory process of repair § Therefore immune status and activity determine HPA/brain settings § Hypervigilant or depressed immune states reflect in brain states 46 46

IL-1β, TNF-α, IL-6 Someone you met H P A A X I S P N S S N S Cytokines 47 signal in the brain: - Saturable transporters - BBB leakiness - Localized production - Binding to receptors on afferent nerve fibers - Recruitment of activated cells Cytokines and DOCs NE IL-1β, TNF-α, IL-6 NF-κB Ach GCs Immuno-competent Cell (Macrophage) Raison CL, Lowry CA, Rook GA. . Arch Gen Psychiatry. 2010 Dec; 67(12): 1211 -24. Something you et 47

Immune Tolerance ”Don’t be so Reactive” § § § If it weren’t for tolerance we would constantly fighting a war with the foreignness everywhere Complex feedback system developed through reactor and moderator substances activating and suppressing immune/ inflammatory response creating an immune capacity of tolerance Net reactor chemistry x net moderator chemistry = immune tolerance Especially strategic to the autoimmune circumstance – goal is to reduce immune burdens and promote immune tolerance and thus reduce immune reactivity Infections, infestations, toxicities, allergens, injuries, inoculations, etc. create a burden teasing out intolerance and excessive reactions 48

Immune mechanisms – schematic Activate acquired immune response s Cell Membrane Foreignness Reactor mediators Tolerance mechanisms moderating acquired immune activation Nuclear Membrane Cytoplasm Nuclear genetic code 49 Gene 49 Activation

Sequential Immune Up-Regulation § § § Especially under the teeth, diverticulosis, severe infections near or in bone, body cavities like sinus, ears, pelvic, intestinal Sequential immune bolstering protocols for one month each at therapeutic dosage – “deep cleaning” Up regulate immune system gradually beginning with Sesame Oil Perles (6/day), followed by Thymex (10/day), then Immuplex (6/day), Congaplex (15/day), Allerplex (15/day), Echinacea (4/day), Astragulus (4/day) Clear infestations with Zymex II (6/day), Multizyme (4/day), Wormwood Complex (4/day) – also treats mycoplasmic infections Finally use Chaparral with high concentration of NDGO (strongest known antioxidant) – will clear systemic infection including bowel 50

51



Establish a Differential Diagnosis: Table 2. 1: Symptoms and Associated Medical Conditions on the MSIDS Map, page 68 “Why Can’t I Get Better? ” Symptoms Possible Medical Conditions Laboratory Testing to Consider Unexplained fevers, sweats, chills, or flushing • Lyme disease (chronic and other bacterial, viral, parasitic, and fungal infections) • Babesiosis • Malaria • Brucellosis • Hyperthyroidism • Hormonal failure (early menopause) • Tuberculosis* • Non- Hodgkin’s lymphoma* • Panic disorders • Autoimmune disorders • Inflammation • CBC with a white cell count • CMP with liver functions • Giemsa stain and malarial smears • Babesia IFA • Babesia WA- 1/duncani titers • Babesia FISH and PCR • Thyroid function tests (TFT’s) • Sex hormone levels • Chest X-ray/PPD • Antinuclear antibody (ANA), Rheumatoid factor (RF) • Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) • Cytokine panel
 According to")
Overview: Lyme & Chronic Disease in the US n n n 1) According to the CDC, chronic disease accounts for 70% of the deaths and 75% of the health care costs in the United States 2) Lyme disease is the number one spreading vector borne epidemic worldwide, and mimics other chronic diseases accounting for an increased burden of those suffering with chronic illness (CDC figures 2103: 10 fold increase in cases) 3) There is confusion regarding the diagnosis and treatment of LD due to 2 standards of care in the US 4) Defining Chronic Lyme Disease: What is it? -the difference between the “surveillance” definition and “real life” in the doctors office. Proposing a new definition: Lyme-MSIDS (Multi. Systemic Infectious Disease Syndrome) 5) Diagnosing Lyme Disease: Problems with serology and seronegative infection
 Treating Lyme")
Overview: Lyme & Chronic Disease in the US n n n 6) Treating Lyme disease: evidence of persistent/chronic borrelial infection & the need for longer treatment courses 7) Chronic infection from Lyme and associated tick-borne diseases drives inflammation. 8) Inflammation is the number one common denominator in all chronic disease. 9) Diagnosing and treating the 3 I's: chronic infection, inflammation and immune dysfunction helps individuals recover their health. 10) Detoxification also plays an important role in improving clinical outcomes. 11) A multifactorial model for chronic disease called MSIDS (Multiple Systemic Infectious Disease Syndrome) will be discussed, showing how multiple factors on the MSIDS map can be addressed to help decrease inflammation and reduce disabling symptoms.
 Infections: a)Bacterial: Lyme disease, Ehrlichiosis, Bartonella, Mycoplasma, Chlamydia,")
Defining Chronic Lyme Disease: Lyme-MSIDS 1) Infections: a)Bacterial: Lyme disease, Ehrlichiosis, Bartonella, Mycoplasma, Chlamydia, RMSF, Typhus, b) Parasites: Babesiosis and other piroplasms, filiariasis, amebiasis, Tularemia, Q-Fever, Tick paralysis giardiasis… 1) c) Viruses: EBV, HHV-6, CMV, W Nile, Heartland v. , Powassan encephalitis and other viral encephalopathies 2) d) Candida and other fungi 2) Immune dysfunction: ANA+, RF+ ↑ HLA DR-4 3) Inflammation: ↑ IL-1, IL-6, TNF-α→ “Sickness syndrome” 4) Toxicity: Multiple Chemical Sensitivity, Environmental Illness, Heavy Metals, Mold, and Neurotoxins 5) Allergies: foods, drugs, environmental… 6) Nutritional & Enzyme Deficiencies/ functional medicine abnormalities in biochemical pathways 7) Mitochondrial dysfunction 8) Psychological disorders 9) Neurological dysfunction 10) Endocrine disorders 11) Sleep disorders 12) ANS dysfunction +/- POTS 13) G. I. disorders 14) Elevated LFT’s 15) Pain syndromes 16) Deconditioning

Protocol for stealth pathogens • Sequential Immune Up-Regulation – graduated immune sparing due to reduction of immune burdens • Neuro-endocrine support – HPA support – Symplex F 3 bid, Hypothalamex 1 bid, Black Currant 1 bid • Ongoing hemopoietic and lymph support to assist in the processing of cellular debris and infection remediation • Final amplification of nutritional therapy to promote immune aggression toward sequestered stealth pathogens • This would include the following possibly: • Cat’s Claw Complex 2 bid • Immuplex 3 bid • Sesame Oil 3 bid • Ostrophin 2 bid • Whey Pro Complete 2 scoops daily (source of Ig. G found in colostrum) • Berberine 2 bid or sourced from Gut Flora or Golden Seal • Myrrh tincture 3 droppers twice daily from Weed Botanical • Enzymes to promote cellular cleansing – Multizyme 2 tid, Zypan 2 tid • Ongoing liver support – Livco 2 bid, betacol 2 bid 59

How do we think without proof It would be possible to describe everything scientifically, but it would make no sense; it would be without meaning, as if you described a Beethoven symphony as a variation of wave pressure. Albert Einstein

Principles at work • Sufficient clinical observation allows mechanisms to be revealed that will remove the idiopathic mystery of hypertension and return it to a simple physiological modulation and resultant augmentation in function, balance, tissue fortification and promotes healthy genetic expression • This allows the symptom resolution to occur as a result of system ‘mosaic’ change, and then of course the downstream events occur • The longing in the public is for this sort of detective work to find the cause and make the correction – increasingly food is seen as medicine and people are asking more and more for what foods will change their health patterns 61

Sequential Intervention f By giving hope through discussion of therapeutic rationale and then accountably determine if therapy had efficacy it is possible to initiate activity that may assist a person to make the changes that result in healing f Sequential intervention and accountable follow-up can show what has worked and what may still need to be employed f Promote an understanding of intervention that creates evolutions in individual physiology and show the effect of that intervention f Allow every condition to become a strategic consideration of possible etiology and therapeutic rationale – people are in search of experts – reveal yourself f The comprehensive nature of nutritional therapy means there is always more physiology to optimize and support leaving an individual constantly refining as long as they wish to further improve their status f If the practitioner is accountable s/he will be allowed to experiment with reasonable ideas

Change the world It wants to 63
- Slides: 63