Menstrual Disorders Excessive Vaginal Bleeding Secondary Amenorrhea and

Menstrual Disorders: Excessive Vaginal Bleeding, Secondary Amenorrhea and Primary Amenorrhea Betsy Pfeffer MD Assistant Professor Clinical Pediatrics Columbia University Morgan Stanley Children’s Hospital of New York Presbyterian

Normal Menstrual Cycle Days 1 -13 • Hypothalmus-Pituitary – Increased Gn. RH, FSH • Ovary-Follicular Phase – Estrogen produced by granulosa cells – Development of primary follicle – Feedback of E 2 (+ to decrease FSH, - to increase LH) • Uterus-Proliferative Phase – Increased glandular cells and stroma

Normal Menstrual Cycle Days 15 -28 • Hypothalmus-Pituitary – Decreased Gn. RH, FSH, LH • Ovary – Primary follicle becomes corpus luteum – Corpus luteum secretes progesterone x 14 days • Uterus-Secretory Phase – Coiling of endometrial glands – Increased vascularity of stroma – Increased glycogen in endometrial cells
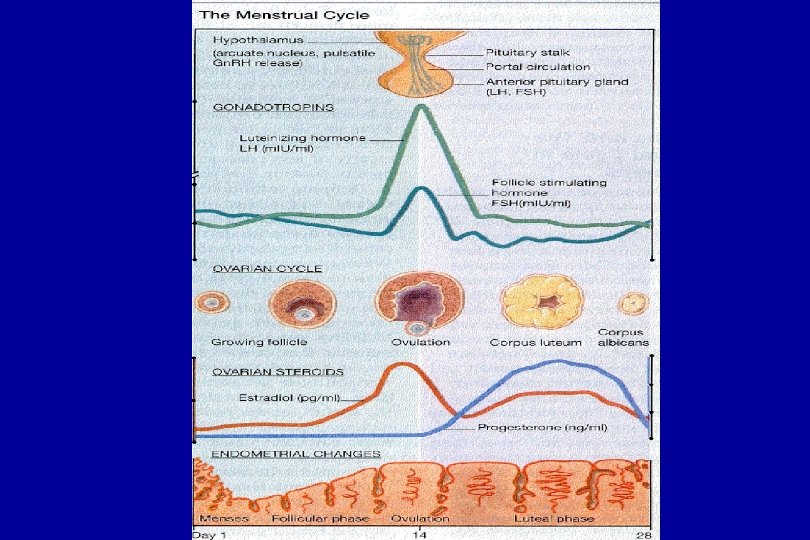
 – Ovulation")
Normal Menstrual Cycle • Average of Menarche is 12. 7 (Tanner 4) – Ovulation occurs in 50% of girls one year post menarche and in 80% by two years • • 21 -40 days long 2 -8 days of bleeding 20 -80 cc blood loss Once cylic menses established it is still normal to have an occasional anovulatory cycle

Anovulatory Cycles • Normal up to gynecologic age of 2 -3 years • Cycles may be long (8 -12 weeks) – If sexually active may be worried about pregnancy • Cycles often short (2 -3 weeks)

Secondary Amenorrhea • Secondary Amenorrhea – No period for 12 -18 months after menarche – Absence of three menstrual cycles in the teen who has already established regular cyclic menses • Oligomenorrhea – Uterine bleeding at prolonged intervals (41 days – 3 months) with normal flow/duration and quantity • Same differential/evaluation for secondary amenorrhea and oligomenorrhea

Normal Menses • Dependant on an intact hypotalamic-pituitaryovarian-uterine axis • Disruption of this axis at any level can lead to amenorrhea/oligomenorrhea

Hypothalamic causes of Secondary Amenorrhea • • • Pregnancy Medications Endocrinopathies Eating disorders Tumors/Infiltrative process/Infections Chronic disease Exercise Stress Idiopathic: abnormal Gn. RH, Kallman’s syndrome: hypogonadotropic hypogonadism (low FSH/LH) anosmia

Endocrinopathies • PCOS: chronic anovulation/hyperandrogenism • HAIR-AN Insulin LH Estrogen FSH Normal/Low Androgen Theca Cells

Endocrinopaththies • Thyroid Disease • Cushings • Late Onset Congenital Adrenal Hyperplasia – Primarily 21 hydroxylase deficiency

Pituitary causes of Secondary Amenorrhea • Tumor • Infiltrative • Nonneoplastic lesions – Sheehan’s Syndrome: pregnancy related – Simmonds Disease: non pregnancy related – Aneurysm

Ovarian and Uterine causes of Secondary Amenorrhea • Premature Ovarian Failure – Menopause before age 35 – Associated with autoantibodies – Increase in thyroid/adrenal disease – Post chemotherapy/radiation • Asherman’s Syndrome

Secondary Amenorrhea History • • • Menstrual History Sexual History Past Medical History/Surgical History Family History Headaches Galactorrhea Nutritional Status/Dietary History Androgen excess/Symptoms of Thyroid Disease Stress Exercise Medications

Secondary Amenorrhea Physical Exam • • Vital Signs/Ht/Wt/BMI Tanner Stage Goiter Signs of androgen excess: hisuitism, cliteromegly, acne, hair loss Galactorrhea Anosmia Signs of systemic disease Consider pelvic in sexually active teen

Secondary Amenorrhea Laboratory Evaluation • • Rule out pregnancy FSH/LH TSH Consider: Prolactin, DHEAS, Testosterone, 17 – OHP, Cortisol

Secondary Amenorrhea Evaluation • If HCG is negative give progesterone challenge • + withdrawl bleed – endometrium has been primed with estrogen – Suggests anovulation/does not identify the cause • - withdrawl bleed – Hypoestrogenemia : CNS lesion, Ovarian failure, anorexia, Turner’s mosaic – Endometrial damage: Asherman’s

Secondary Amenorrhea Treatment • Treat precipitating cause if it is identified • If due to anovulation induce uterine bleeding every 6 -8 weeks or place on birth control because of increased risk of endometrial cancer and anemia secondary to DUB • Encourage need for birth control if sexually active • Refer to specialist when indicated

Etiology of Excessive Vaginal Bleeding in Teens • Dysfunctional Uterine Bleeding -Etiology of >95% excessive vaginal bleeding in perimenarchal teens w/ normal hemoglobin and normal physical exam • Usually due to anovulation • Diagnosis of exclusion

Dysfunctional Uterine Bleeding • Irregular, prolonged, excessive, unpatterned painless bleeding • Anovulatory cycle • Endometrial in origin • No structural or organic pathology

Differential Diagnosis of Excessive Vaginal Bleeding • Complications of Pregnancy – ectopic, threatened abortion, hydatiform mole • Infections – cervicitis, PID • Endocrine Disorders – hypothyroidism, PCOS, late onset CAH, cushings, androgen producing tumor, prolactinoma

Differential Diagnosis of Excessive Vaginal Bleeding • Blood Dyscrasias – ITP, VWD, Glanzman’s disease, SLE, leukemia liver/renal failure, inherited clotting deficiencies, vit K deficiency • Ovarian Masses – hormonally active cysts, tumor, polyps • Trauma/foreign body • Medications – contraception

DUB in Adolescents • History often unreliable • Hormonal therapy almost always works • Curettage rarely necessary

DUB in Adolescents • • • History Gynecological Age Menstrual History Sexual Activity Method of Contraception Presence of Pain Nausea/breast tenderness Dizziness Symptoms of endocrinopathies Other Bleeding History Medications

DUB in Adolescents physical exam • • • Vital signs Pallor Bruising/Petechiae Murmur/Tachycardia Evaluation for endocrinopathies-hirsuitism, acne, cliteromegaly, goiter, visual fields, acanthosis, galactorrea • Pelvic exam if sexually active

Lab Evaluation • • HCG CBC: hemoglobin and platlets GC/Chlamydia LH/FSH, TSH, 17 - OHP, Prolactin, Testosterone, DHEAS • If Hemoglobin less than 10 – PT/PTT, Von Willebrand’s Ag, Ristocetin Cofactor, Factor X 111 and 1 X, Platlet aggregation studies – Referral to Hematology

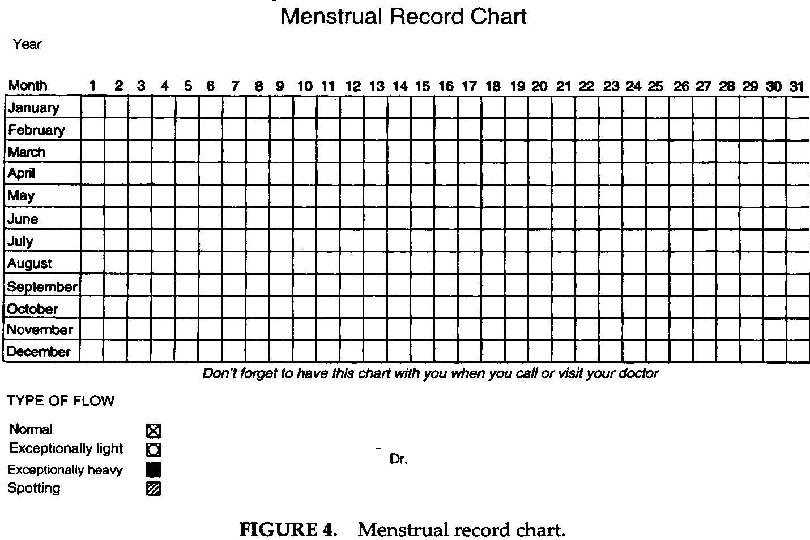
Mild DUB in Adolescents hemoglobin >11 • • • Reassure Iron supplementation Menstrual calendar Phone follow-up in one week Follow-up 3 months unless continues bleeding Contraception if sexually active

Moderate DUB in Adolescents Hemoglobin 9 -11 • Low dose monophasic OCP – – 2 -4 tabs a day until bleeding stops Then once a day Allow withdrawal bleed when Hemoglobin >11 Cycle for at least 6 months • Iron when on one OCP/day • Progesterone only pills: Aygestin better than Provera • Close follow-up

Severe DUB in Adolescents Hemoglobin < 9 and/or Massive Hemmorhage • • Hospitalize Fluid resuscitation Blood transfusion rarely needed Premarin 25 mg IV q 4 -6 hours (max 4 doses) Monophasic OCP q 6 h then tapered to qd Iron Continue OCP 6 months

Etiology of Acute Menorrhagia Requiring Hospital Admission Other 7% Primary Coagulation Disorder-19% DUB-75%

DUB in Adolescents Goals • • • Correct hemodynamic imbalance Prevent uncontrolled bleeding loss Correct anemia Replace iron storees Encourage contraception for the sexually active teen

Primary Amenorrhea • Primary Amenorrhea – No uterine bleeding by age 16 – No secondary sex characteristics by age 14 – SMR 5 for one year and no uterine bleeding – No uterine bleeding four years after breast development

Etiology of Primary Amenorrhea • Primary amenorrhea w/o breast development but w/ normal genitalia – Turner’s Syndrome/Mosaicism – Structurally abnormal X chromosome – Gonadal dysgenesis – 17 alpha hydroxylase deficiency (normal stature, hypertension, hypokalemia, sexually infantile) – Hypothalamic failure due to inadequate Gn. RH
 but absent")
Etiology of Primary Amenorrhea • Primary amenorrhea w/ breast development (SMR 4) but absent uterus – Testicular Feminization – Congenital absence of the uterus (Rokitansky Syndrome). Associated with renal and skeletal anomolies

Etiology of Primary Amenorrhea • Primary amenorrhea w/o breast development and w/o uterus – RARE – Usually male karyotype w/ elevated gonadotropin levels and low testosterone. Produce enough MIF to inhibit develpoment of female internal genital structures (17, 20 -lyase deficiency, agonadism, 17 alpha hydroxylase deficiency w/ 46 XY karyotype)
 and w/ uterus")
Etiology of Primary Amenorrhea • Primary amenorrhea w/breast development (SMR 4) and w/ uterus – Same evaluation as for secondary amenorrhea – Imperforate Hymen – Turner’s Mosaic

Primary Amonorrhea Physical exam • Blood Pressure/Height/Weight • Tanner stage • Signs of gonal dysgenesis: Webbed neck, low set ears, broad shieldlike chest, short fourth metacarpal • Pelvic exam – Imperforate hymen – Transverse vaginal septum – Absent uterus

Primary Amenorrhea Evaluation • • FSH/LH Testosterone Karyotype Pelvic Ultrasound

Primary Amenorrhea Treatment • Turner’s Syndrome – growth hormone first – estrogen replacement later • Rokitansky Syndrome – vaginoplasty • Testicular Feminization – remove gonads – Estrogen replacement – Vaginoplasty • Enzyme Defects – hormone replacement – remove gonads if Y chromosome is present
- Slides: 40