Menopause HRT Hormone Replacement Therapy Do Dr Gazi
 Doç. Dr. Gazi YILDIRIM Yeditepe Üniversitesi Hastanesi Kadın")


 Age At Menapause And Expected Life Age at menopause 1850 1900 1950")






 �Sleep disturbances �Mood disturbances. �Somatic symptoms:")







…lessons learnt from WHI �Is NOT risk free �NOT cardioprotective �CAN")
















 • Basic science,")





 �Mechanism of Action: SERM that selectively stimulates")
 �Approved in Women for 2 � prevention of osteoporosis � osteopenia")




- Slides: 48
Menopause & HRT (Hormone Replacement Therapy) Doç. Dr. Gazi YILDIRIM Yeditepe Üniversitesi Hastanesi Kadın Hastalıkları ve Doğum AD
Reproductive Aging Oocytes and Follicles �Process begins in embryonic life. � 20 weeks gestation - 6 - 7 million follicles. �At birth - 1. 5 -2 million follicles �At menarche - 300, 000 - 400, 000 follicles �Follicular atresia continues throughout life. �Follicular loss accelerates when the total number of follicles is ~25, 000 �When follicles are sufficiently depleted (<1000), menopause occurs.
Menopause Facts �Average at menopause: 51 years � (1% at age 40, 5% after age 55) �Factors impacting age at menopause � Maternal age at menopause � Tobacco use � SES/ Education � Alcohol use � Body Mass Index �Factors that probably don’t impact on age at menopause � OCP use � Parity � Race � Height
Age (years) Age At Menapause And Expected Life Age at menopause 1850 1900 1950 Date 2000 *Projected estimate. Federal Interagency Forum on Aging-Related Statistics. Indicator 2: Life Expectancy. Available at: http: //www. agingstats. gov/tables%202001/tables-healthstatus. html. Accessed 1/3/02. US Department of Health and Human Services. Healthy People 2010. Washington DC: January 2000. 2050*
Stages of Reproductive Aging
Reproductive Stage Miscarriage Rate / month 25% 12% Pregnancy Rate / month 20 30 37 40 Age in years 45
Reproductive Aging Hormonal Changes Hypothalmus Gn. RH FSH Inhibin B + Normal Ovary
Reproductive Aging Hormonal Changes Hypothalmus Gn. RH FSH Estradiol / Inhibin B + Aging Ovary
Reproductive Aging Hormonal Changes Hypothalmus Gn. RH FSH Estradiol / Inhibin B + Menopausal Ovary
Diagnosing Perimenopause �Clinical diagnosis based on menstrual cycle pattern. �Early follicular phase FSH and symptoms may help solidify diagnosis. �Rule out hypothyroidism, depression etc.
Perimenopause -- Symptoms: Highly Variable �Vasomotor instability (85%) �Sleep disturbances �Mood disturbances. �Somatic symptoms: �Fatigue, palpitations, headache, increased migraine, breast pain and enlargement. �Oligo- Anovulation �heavier or irregular cycles.
Estrogen Deprivation Related Problems Estrogen Secretion Short-term Symptoms Development of subclinical disease Long-term Diseases Hot flushes Mood, sleep, and/or acute cognitive changes Urogenital symptoms Cardiovascular disease Osteoporosis Cognitive decline (Alzheimer’s disease) 40 45 50 Age (years) 55 60 65 70 75
Menopausal Symptom Prevalence of Hot Flushes
Sleep Disturbance in Peri/Postmenopausal Women ↑ reports of difficulty sleeping 1 Waking up repeatedly 1 Kravitz, Menopause 2003 Falling asleep 2 Kravitz, Sleep 2008
Managing Perimenopause Goals: �Patient education �Prevention of endometrial cancer �Individualized symptomatic relief �Menstrual control �Minimizing hot flashes �Mood disturbances
Managing Perimenopause Symptom Relief Menstrual Cycle Control Birth Control Endometrial Cancer Prevention Hormonal contraceptives (oral or ring) +++ +++ Cyclic progestin therapy +/- - ++ Progesterone IUD - +/- +++ EPT ++ - - +++
Hormone Therapy Risks VTE e Strok cer n a C reast s t i f e n e B Cognition CVD Risk QOL nefit e B l a t e l e Sk trol n o C m o t Symp B Weighing Risks vs Benefits Adapted from: Writing Group for the Women’s Health Initiative. JAMA. 2002; 288: 321 -333.
WHI Hormone Trials
Menopause Hormone Therapy (MHT)…lessons learnt from WHI �Is NOT risk free �NOT cardioprotective �CAN harm �Aged �Remote from last menstrual period �Overweight/obese �Existing pre morbidities
MHT & Breast Cancer Risk Current Understanding: • Estrogen alone Rx in hysterectomized population is deemed relatively safe for breast tissue • Type of progesterone (natural progesterone preferred over synthetic) and regimen (cyclic preferred over continuous) merit consideration.
MHT & VTE Risk Age Body Mass Current Understanding: • Advancing age, obesity and individualized profile should be considered when assessing risks for TE in patient being considered for HT
VTE Risk: Drug & Route of HT & Progestin Oral vs. Transdermal E Current Understanding: • Choice of progestin (progesterone preferred to synthetic progestins) and both dose & route of E (low dose transdermal preferred over oral route) can confer risk reduction against TE.
MHT Decision Should Be Based upon Individualized Assessment Risks Benefit � Underlying • ROLE Symptoms THERE IS NO OF atherosclerosis? • Severity �HORMONE Stroke/MI THERAPY FOR • Nature � VTE? CARDIAC PROTECTION � Breast cancer? … does • Skeletal perspective she have a uterus and OR therefore will need E+P COGNITIVE BENEFIT
TANIMLAR
Conclusions with Level of Evidence A Hot flashes • “Standard-dose” estrogen with or without a progestogen markedly lowers the frequency and severity of hot flashes, and lower doses of estrogen are also effective in many women. • Tibolone (a hormonal alternative widely available worldwide but not in the United States) alleviates postmenopausal vasomotor symptoms.
Conclusions with Level of Evidence A Urogenital system • Very low doses of vaginal estradiol relieve symptoms and normalize vaginal atrophy. • Estrogen used vaginally or systemically reduces the symptoms of overactive bladder. • Vaginal estrogen reduces the incidence of recurrent urinary tract infections. • Tibolone improves urogenital atrophy.
Conclusions with Level of Evidence A Bone • Estrogen with or without a progestogen prevents early postmenopausal bone loss and augments bone mass in late postmenopause as effectively as the bisphonates. • Estrogen alone and estrogen plus a progestogen prevent hip and vertebral fractures. • Tibolone significantly reduces vertebral and nonvertebral fractures in osteoporotic women over the age of 60 yr. • Raloxifene, a selective estrogen receptor modulator, improves bone mineral density and reduces vertebral but not hip fractures.
Conclusions with Level of Evidence A Colon cancer • MHT with estrogen plus a progestogen decreases colon cancer risk. Breast • Raloxifene decreases breast cancer risk. • Estrogen and estrogen plus a progestogen increase mammographic density. • Tibolone increases risk of breast cancer recurrence.
Conclusions with Level of Evidence A Sexual function • Physiological amounts of transdermal testosterone increase the number of self-reported, sexually satisfying events per month as well as desire, arousal, responsiveness, and orgasm. • DHEA does not significantly improve sexual function. Venothrombotic episodes • MHT increases the risk of venothrombotic episodes approximately 2 -fold and is multiplicative with baseline risk factors including age, higher body mass index, thrombophilias, surgery, and immobilization. • Raloxifene increases the incidence of venothrombotic episodes.
Conclusions with Level of Evidence A Stroke • Tibolone increases risk of stroke in older but not in younger women. • No increase in stroke occurs with raloxifene. • Hormone use does not reduce stroke incidence in older women with preexisting vascular disease. Endometrium • Estrogen alone without a progestogen causes an increase in endometrial cancer. • Continuous estrogen plus a progestogen does not cause endometrial cancer. • Tibolone does not induce endometrial hyperplasia or carcinoma
Conclusions with Level of Evidence A Gallbladder • Estrogen alone and estrogen plus a progestogen increase the risk of gallbladder disease. Cognition • MHT initiated after age 60 yr does not improve memory
Selected Conclusions with Level of Evidence B Metabolism • Use of estrogen alone and estrogen plus a progestogen in the. WHI was associated with a decrease in the risk for type 2 diabetes. • Initiation of MHTis associated with lesser accumulation of weight, fat mass, and/or centrally located fat mass. Joints • Estrogen exerts a protective effect on osteoarthritis. • Estrogen alone reduces total arthroplasty rate. • Addition of a progestogen to estrogen appears to counteract the beneficial effects of estrogen on arthroplasty rate.
Selected Conclusions with Level of Evidence B Quality of life • MHTproduces an improvement in health-related quality of life through decreased symptoms, sleep enhancement, and, possibly, mood enhancement. Sexual function • Tibolone improves sexual well-being in postmenopausal women presenting with low libido, with greater improvements in desire, arousal, satisfaction, and receptiveness than seen with transdermal estrogenprogestogen therapy.
Selected Conclusions with Level of Evidence B Endometrium • Sequential estrogen plus a progestogen reduces the risk of endometrial carcinoma compared to estrogen but not as effectively as continuous estrogen plus a progestogen. • Vaginal estrogen in doses of 7. 5 to 25 g twice weekly does not stimulate the endometrium. • Raloxifene reduces the incidence of endometrial carcinoma.
Selected Conclusions with Level of Evidence B Premature menopause • Women with bilateral oophorectomy prior to age 45 are at increased risk of negative effects on the cardiovascular system, bone, cognition, mood, and sexuality. Overall mortality • MHT was associated with a 40% reduction in mortality in women in trials in which participants had a mean age below 60 yr or were within 10 yr of menopause onset.
Selected Conclusions with Level of Evidence B Coronary heart disease (CHD) • Basic science, animal models, and observational studies support the hypothesis that MHT may prevent atherosclerosis and reduce CHD events. • Subgroup analyses suggest that the lack of benefit or increase in CHD risk observed in the overall analysis of the WHI resulted from harmful effects of MHT in older women starting therapy many years after onset of menopause. • Tibolone does not increase the risk of CHD events.
Selected Conclusions with Level of Evidence B • Use of estrogen alone for less than 5 yr may reduce the risk of breast cancer in patients starting therapy many years after the onset of menopause. • Tibolone reduces the risk of developing breast cancer. • Estrogens increase the risk of breast cancer after more than 5 yr of use, particularly in recently menopausal women. • Combined estrogen and progestogen therapy increases the risk of invasive breast cancer, which may occur within 3 to 5 yr of initiation and rises progressively beyond that time.
Future of MHT Target Breast Uterus Hot Flush Vagina Bone E+P SERMs TSECs
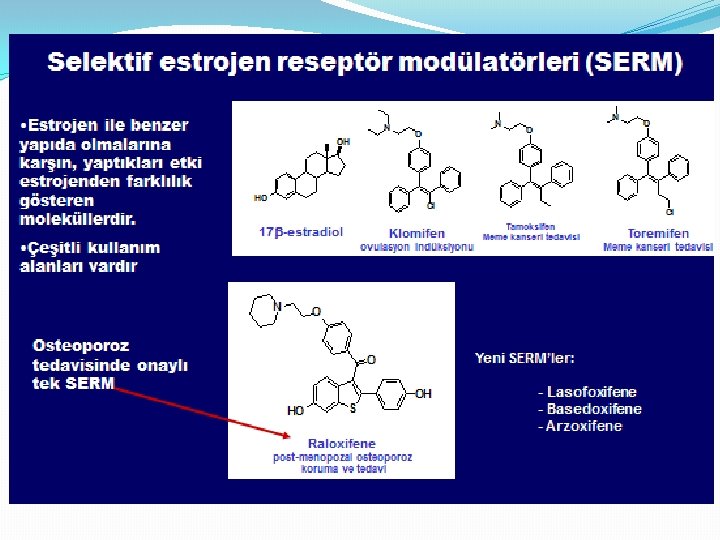
SERM �Clomiphene �Tamoxifen �Toremifene �Droloxifene �Iodoxifene �Raloxifene �Basedoxifene �Ormeloxifene-NEAREST TO IDEAL 40
Raloxifene �Mechanism of Action: selective estrogen-receptor modulator �Benefits � Increases BMD of hip and spine in women 1 �Females: approved for treatment and prevention of osteoporosis in women. �Not approved in males 2 �Narrow study contexts 3, 5 �Was not shown to significantly impact BMD in males 4
TSEC �A TSEC is the partnering of a SERM and other estrogens to achieve clinical results based on their blended tissue selective activity profiles. � One option for a TSEC is the pairing of a SERM(Bazedoxifene) with CEE. 42
Tissue Selective Estrogen Complex �Bazedoxifine/Conjugated Estrogen (Duavee) �Mechanism of Action: SERM that selectively stimulates lipid metabolism and bone, however, has no effect on the uterus and breast. �Benefits � FDA approved for � postmenopausal � moderate/severe vasomotor symptoms prevention of postmenopausal osteoporosis. � Increased hip and lumbar BMD
�Bazedoxifene/Conjugated Estrogen (Cont’d) �Approved in Women for 2 � prevention of osteoporosis � osteopenia � post menopausal vasomotor and sleep disturbances �Men: None of the three major clinical trials included men, despite that estrogen has been demonstrated to play a significant role in bone formation 3, 4, 5.
SPRM Pure agonist abortifacient treshold Pure antagonist Progesterone J 1042 J 867 J 956 Mifepristone (RU 486) Onapristone Asoprisnil (J 867)
prevention of postmenopausal osteoporosis PRIMARY PREVENTION 1. HRT 2. SERMS 3. TIBOLONE 4. Biophosphonate SECONDARY PREVENTION 1. Biophosphonates 2. Calcitonin (>5 yrs menopause) 3. Teriparatide 46
• Promotes bone formation and decreases bone resorption Mechanism of Action Application • First line treatment for osteoporosis in both men and postmenopausal women 1 Bisphonates • Approved in both sexes for the prevention and treatment of osteoporosis Aledronate 2, Risedronate 3 and Zoledronic Acid 4
Bisphonates Drug Route/ Frequency Indicated for which gender Alendronate PO/QDay, QWeek Women Men Risedronate PO/QDay, QWeek, QMonth Women Men Ibandronate Zoledronic Acid Vertebral Fracture RR Hip Fracture RR NE Nonvertebral RR NE PO/QMonth Women IV/Q 3 Month IV/QYear RR = Risk Reduction Women Men NE = No effect demonstrated