MENOPAUSE DONE BY ANMAR MAGHARBEH Menopause is a

MENOPAUSE DONE BY: ANMAR MAGHARBEH

• Menopause is a retrospective diagnosis , it is defined as 12 months of amenorhhea. • The average at menopause is approximately 51 years. Happens gradually with irregular anovulatory cycle • Peri menopause or climacteric. It is the time period from when the ovaries start to fail until 12 months after the last menstrual period. • Premature menopause is defined as menopause that occurs between the age of 30 and 40 years. • Premature ovarian failure : menopause before age of 30

SYMPTOMS • • Hot flushes Night sweats Mood swings Urogenital atrophy

DIAGNOSIS The diagnosis of menopause is mainly a clinical diagnosis. Symptoms include : menstrual irregularities , amenorrhoea, and vasomotor symptoms. The use of serum endocrine tests such as hormone levels are of little value in the perimenopausal years as they are unpredictable due to the hormonal variations that frequently occur in association with episodic and irregular ovulatory cycles. An elevated serum FSH in association with a low serum oestradiol may be suggestive of menopause,

NON-PHYSIOLOGICAL MENOPAUSE Premature ovarian insufficiency If menopause occurs before the age of 40 years it is defined as premature ovarian insufficiency (POI), occur also sometimes called premature ovarian failure (POF), or premature to menopause. It is thought in approximately 1% of women under 40 years Causes : Primary Chromosome anomalies (e. g. Turner’s, fragile X) Autoimmune disease (e. g. hypothyroidism, Addison’s, myasthenia gravis) Enzyme deficiencies (e. g. galactosaemia, 17 a-hydroxylase deficiency) Secondary Chemotherapy or radiotherapy Infections (e. g. tuberculosis, mumps, malaria, varicella)

IATROGENIC MENOPAUSE medical treatments and menopause after cancer treatment Gn. RH is given in a constant high dose, it desensitizes the Gn. RH receptor and reduces LH and FSH release. Drugs that are Gn. RH agonists (e. g. buserelin and goserelin) can be used as treatments for endometriosis and other gynaecological problems surgical menopause Bilateral salpingo-oophorectomy (BSO) may also be performed prophylactically for women at high risk of inherited malignancies such as breast and ovarian cancer, with BRCA 1 and 2 gene mutation screening.
 Vasomotor symptoms,")
EFFECTS OF THE MENOPAUSE BY TIME OF ONSET Immediate (0– 5 years) Vasomotor symptoms, (e. g. hot flushes, night sweats) Psychological symptoms (e. g. labile mood, anxiety, tearfulness) Loss of concentration, poor memory Joint aches and pains Dry and itchy skin Hair changes Decreased sexual desire Intermediate (3– 10 years) Vaginal dryness, soreness Dyspareunia Urgency Recurrent urinary tract infections Urogenital prolapse Long term (>10 years) Osteoporosis Cardiovascular disease Dementia

MANAGEMENT Diet and lifestyle regular exercise, stopping smoking and reducing alcohol consumption

NON-HORMONAL APPROACHES considered in the management to reduce symptoms of hot flushes when hormones are contraindicated or unwanted

Alternative and complementary treatments: These groups of treatments are widely available but most of them Lack sufficient scientific evidence.
 • Acupuncture • Reflexology • Magnetism •")
Complementary drug-free therapies (delivered by a practitioner) • Acupuncture • Reflexology • Magnetism • Reiki • Hypnotism Herbal/natural preparations (designed to be ingested) • Black cohosh (Actaea racemosa) • Dong quai (Angelica sinensis) • Evening primrose oil (Oenothera biennis) • Gingko (Gingko biloba) • Ginseng (Panax ginseng) • Kava kava (Piper methysticum) • St John’s wort (Hypericum perforatum) ‘Natural’ hormones (designed to be ingested or applied to the skin) • Phytoestrogens such as isoflavones and • red clover • Natural progesterone gel • Dehydroepiandrosterone (DHEA)

Non-hormonal treatments for vasomotor symptoms : Clonidine Beta-blockers : Propanolol Alpha-adrenergic agonists Modulators of central neurotransmission : Venlafaxine Fluoxetine Paroxetine Citalopram Gabapentin

HORMONAL REPLACEMENT THERAPY Oestrogen only : • In women with a uterus, oestrogen-only therapy is associated with a significantly increased risk of developing endometrial hyperplasia and cancer. • Used in women who had hysterectomy. • Natural conjugated: Premarin • Synthetic: Estradiol Valerate(Estrofem)

Combined hrt : • Sequential combined regimens • Continuous combined regimens

Sequential combined regimens : The addition of Progestogen to Estrogen therapy reduces the risk of endometrial disease, but regimens should usually include at least 10 days in each monthly cycle.

Continuous combined regimens : For age of 54, or her periods have stopped more than one year at any age.

Testosterone : given to women with disorders of sexual desire and energy levels who have failed to respond to normal HRT.
 : • Reduces the incidence of vertebral fractures in women")
Raloxifene ( SERM ) : • Reduces the incidence of vertebral fractures in women with osteoporosis. • There is no current evidence of protection against fractures at the hip or at other sites. • Use of raloxifene is associated with reduced risk of breast cancer but : Increased incidence of vasomotor symptoms
 : • has oestrogenic, progestogenic androgenic properties. • It appears")
Tibolone ( livial ) : • has oestrogenic, progestogenic androgenic properties. • It appears to be effective in the treatment of vasomotor symptoms. • Recent data suggest that tibolone may also be associated with an increased risk of breast cancer, but less than that associated with combined oestrogen and progestogen preparations.

ROUTES OF HORMONE THERAPY ADMINISTRATION The two main routes of HRT delivery are oral and Transdermal But Progestogen in the form of levonorgestrel may be administered as an intrauterine releasing system (IUS), Mirena®

BENEFITS OF HRT • Vasomotor symptoms : hot flushes. Improvement is usually noted within four weeks. In most cases, 2– 3 years’ therapy is sufficient • Mood or sleep disturbances: HRT often improve sleep by alleviating night sweats. . • Urogenital symptoms: vaginal dryness, soreness, Paiful sex, and urinary frequency and urgency respond well to estrogens, which may be given either topically or systemically.

Bone : - HRT reduces the risk of spine and hip osteoporotic fractures. - HRT is currently not recommended as a first line for osteoporosis prevention. - While alternatives to HRT are available for the prevention and treatment of osteoporosis in elderly women, estrogen may still remain the best option, particularly in younger and/or symptomatic women. It is cheaper than other alternatives such as bisphonates. The colon : • While the WHI study demonstrated a clear benefit of HRT on the incidence and mortality of colon cancer, • the use of HRT to prevent this malignancy is not indicated.

CONTRAINDICATIONS Absolute contraindications: • suspected pregnancy; • breast cancer; • endometrial cancer; • active liver disease; • uncontrolled hypertension; • known current venous thromboembolism (VTE); • known thrombophilia (e. g. Factor V leiden); • otosclerosis. Relative contraindications: • uninvestigated abnormal bleeding; • large uterine fibroids; • past history of benign breast disease; • unconfirmed personal history or a strong family history of VTE; • chronic stable liver disease; • migraine with aura. . •

SIDE-EFFECTS Side-effects associated with oestrogen: • breast tenderness or swelling; • nausea; • leg cramps; • headaches. Side-effects associated with progestogen: • fluid retention; • breast tenderness; • headaches; • mood swings; • depression; • acne

RISKS OF HORMONE THERAPY Cancer: Breast cancer is without doubt the cancer that attracts most concern from patient Endometrial cancer and ovarian cancer are not considered significant risks with HRT use. Endometrial malignancy risk is largely eliminated if women are given progestogens. Incidence of ovarian cancer does not significantly increase with HRT use.

Cardiovascular disease and stroke most of the effects of HRT on the cardiovascular system when given to younger women are beneficial. deleterious and when given to older women the effects may become the risk is higher in women taking combined HRT Stroke incidence has a similar age effect, with the increased incidence greater in the older woman. The effect is small and is only on the incidence of ischaemic stroke, thought to be an increase of an additional 2 women per 10, 000 women per year when on HRT

Venous thromboembolism: The influence of HRT on the clotting system is similar to that of the oral contraceptive. The background incidence of all VTE in women over 50 is low (approximately 15– 20 per 10, 000) and HRT doubles this risk. There is evidence to suggest that transdermal HRT, through its avoidance of effects on the liver, may not have such a great effect on VTE incidence.

POST MENOPAUSAL BLEEDING

DEFINITION • Is any unscheduled vaginal bleeding that occurs after 12 months of amenorrhoea in a woman of postmenopausal age. • It is a serious symptom which may indicate the presence of malignant disease in the genital tract, So Every woman with PMB should be assumed to have carcinoma until proven otherwise.

CAUSES OF POSTMENOPAUSAL UTERINE BLEEDING • • • Atrophic vaginitis 60 -80% Estrogen treatments 15 -25% Polyps - endometrial or cervical 2 -12% Endometrial Hyperplasia 5 -10% Endometrial Cancer 10% idiopathic 10%

VAGINAL ATROPHY • It is the most common cause of postmenopausal uterine bleeding. • Is thinning, drying and inflammation of the vaginal walls due to low estrogen levels. This is a benign condition • Clinical features: In addition to postmenopausal bleeding: Vaginal dryness , burning sensation, discharge, itching with increased frequency, urgency , incontinence and urinary tract infections • Treatment: 1. Vaginal moisturizers 2. Estrogen either in form of creams, ring or tablet.

HORMONE REPLACEMENT THERAPY • Any vaginal bleeding in a menopausal woman other than the expected cyclical bleeding that occurs in women taking sequential HRT should be managed • A. . Estrogen- cyclical progsetrone : Estrogene will be given everyday. Progestrone will be given for the last (12_14) days. Bleeding is considered normal if bleeding starts after the nineth day of progesterone use or soon after the progestogen phase. • B. Combined estrogen-progestrone therapy: Breakthrough bleeding is common in the first 3 -6 months , Evaluation of the endometrium is recommended during the first year, if bleeding is heavy, prolonged or if any bleeding occurs after one year of use.
. It accounts for")
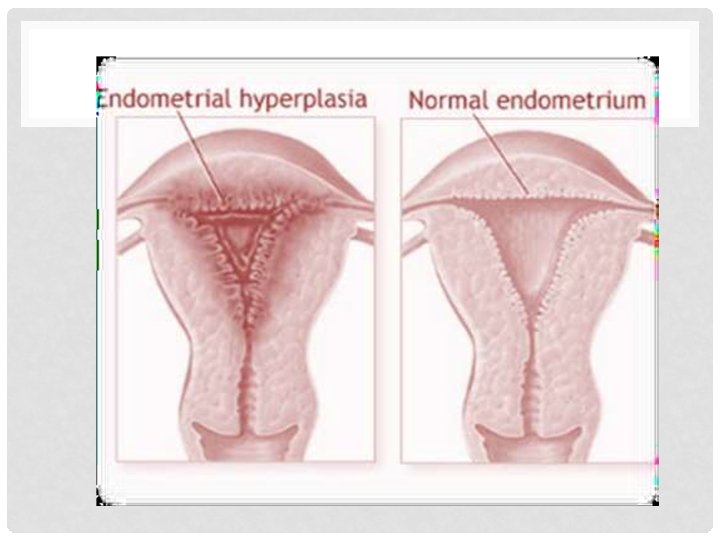
ENDOMETRIAL HYPERPLASIA • Is an abnormal proliferation of the endometrium (glands). It accounts for 5_10 % of PMB. It occurs due to excessive estrogen stimulation. • More than 4 mm is significant. • classification: 1. Hyperplasia without atypia Rx is Progestogens: oral preparation or LNG-IUS (Mirena) 2. Hyperplasia with atypia (premalignant) Rx is Total abdominal hysterectomy with or without BSO. as significant risk of progression to malignancy

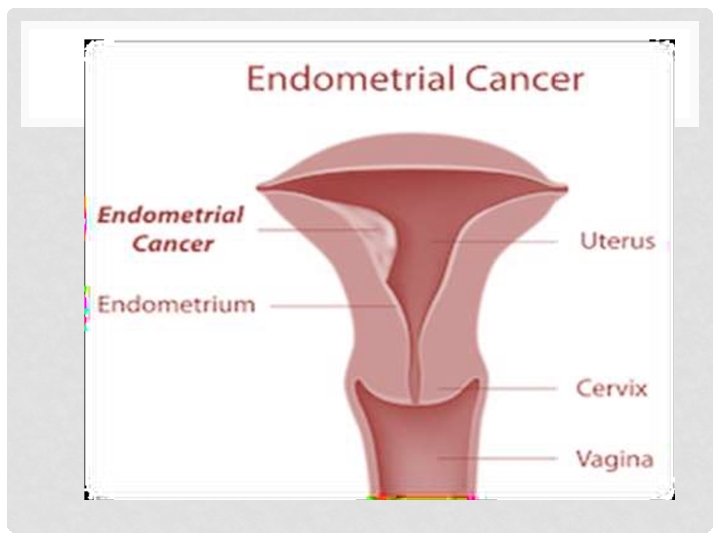
ENDOMETRIAL CARCINOMA • 2 nd most common gynecological cancer. • Is mainly adenocarcinoma arising from the lining of the uterus and is an estrogen-dependent tumor. • Accounts for 10% of postmenopausal bleeding. • 90% of patients with endometrial cancer will present with bleeding. • Has 4 stages: I. Confined to uterine body II. Involves cervix III. Outside uterus but inside the pelvis IV. Extended to blader or rectum

RISK FACTORS OF ENDOMETRIAL CARCINOMA : 1. 2. 3. 4. 5. 6. 7. 8. 9. Early menarche Late menopause Nulliparity Chronic anovulation (P. C. O. S) Obesity (conversion of steroids to oestrone in their peripheral fat) Diabetes mellitus Unoppsed estrogen therapy Tamoxifen therapy (ESTROGENIC ACTIVITY ON ENDOMETRIUM) Personal or family history of: endometrial, ovarian, breast or colon cancer

TREATMENT OF ENDOMETRIAL CARCINOMA • Stage 1 and 2 : total abdominal hysterectomy + bilateral salpingoopherectomy. If resectable surgery followed by chemotherapy • Stage 3 and 4 : radiotherapy If its not resectable neoadjuvant radiotherapy followed by surgery. • High dose of progestin if unfit for surgery. (paliative)

MANAGEMENT I. History II. Examination III. investigations

HISTORY: 1. Details of the bleeding(onset, duration, amount, color, presence of clot, whether it was related to trauma or not). 2. Associated symptoms such as pain, fever or changes in bladder or bowel function might suggest an infective process such as pyometra or the bleeding may be arising from the bowel or bladder. 3. exclude risk factors of endometrial carcinoma.

EXAMINATION 1. General examination: general condition, obesity. exclude signs of malignancy ( weight loss, pale 2. Abdominal examination: for any palpable mass. 3. pelvic examination: • Inspection of the vulva and vagina, particularly looking for atrophy( The vaginal skin looks thin, red and inflamed with areas of pinpoint bleeding). • A speculum examination (cervical polyp and cancer) • A bimanual examination to evaluate uterine size, mobility and the adnexae. 4. Per rectal examination: to exclude colorectal problems.

INVESTIGATIONS 1. Complete blood count 2. Coagulation studies 3. LFT, RFT specific investigations: I. Ultrasound II. CA 125 III. Pippelle smear IV. Dilitation and curetage with biopsy V. Hysterescopy with endometrial biopsy

A- PIPELLE ENDOMETRIAL SUCTION CURETTE. ENDOMETRIAL BRUSH B-VABRA ASPIRATOR
,")
• A tissue sample is taken from the lining of the uterus (endometrium), and is checked under a microscope for any abnormal cells or signs of cancer.

Hysteroscopy • The Gold Standard • Allows Direct Visualization Of Uterine Cavity
: •")
MANAGEMENT OF POST MENOPAUSAL BLEEDING General measures : • Correct general condition(Anti-shock measure): • Hospitalization • • Assessment of blood loss: In some cases the blood volume loss may be excessive , rapid and possibly life threatening. • So rapid restoration of blood volume , vital parameters is followed by local examination to find out the site and source of bleeding • Definitive Treatment : The condition after diagnosis treated according to the underlying cause.

Thank you
- Slides: 47