Meningococcal meningitis Ooi Phaik Yee Hospital Sungai Buloh

Meningococcal meningitis Ooi Phaik Yee Hospital Sungai Buloh 14/9/13

introduction • Meningitis: clinical syndrome characterized by inflammation of the meninges • Meningococcal meningitis – Caused by Nisseria meningitidis – first described by Vieusseux during an outbreak in Geneva, Switzerland in 1805 • Contagious • High case fatality rate • Persistent neurological deficits

• disease spectrum: – occult sepsis with rapid recovery to fulminant disease • Fatality rate – Before 1920 s: 70% – overall now: 9 to 12% – meningococcal sepsis: 40% • 11 to 19% have sequelae – hearing loss – neurological disability – loss of a limb

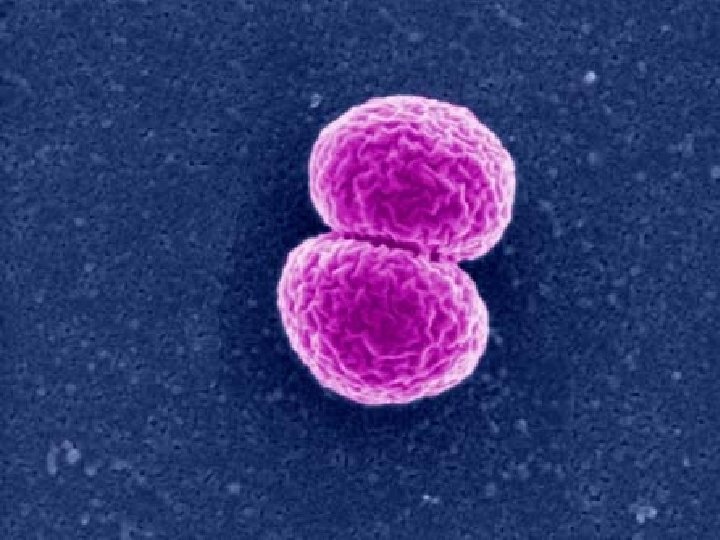
Nisseria meningitidis • Exclusively human, Gram negative, aerobic diplococci • 13 serogroups: A, B, C, H, I, K, L, M, X, Y, Z, 29 E, W 135 • Further classified into 20 serotypes, 10 subtypes & 13 immunotypes • Most infections caused by serogroup A, B, C, Y, W 135

• Capable of changing the genetic material & switching from 1 serogroup to another • Common inhabitant of nasopharynx • 8 -20% of adults are asymptomatic carrier • Mainly affect young children (<7 months) • Also in order child & young adults


Meningococcal disease • 90% is from 3 serogroups: A, B & C – A & C in Asia & Africa – B & C Europe & Americas • All may cause epidemics though the risk differs. • Serogroup A – historically been the main cause of epidemic – still dominates in Africa during both endemic & epidemic periods

• Epidemic rate – Less than 1 -3/100, 000 in developed nations – 10 -25 per 100, 000 in developing countries • cases among infants < 1 month – >50% caused by serogroup B

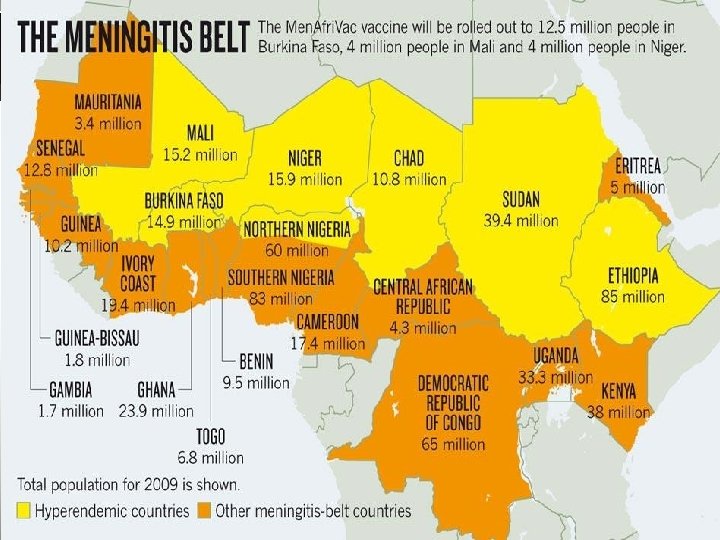
The meningitis belt • World’s highest disease burden • sub-Saharan Africa, stretching from Senegal in the west to Ethiopia in the east • Epidemics occur in seasonal cycles between November & June • Epidemics last 8 -15 years • decline rapidly in rainy season • mechanisms are thought to be related to variations in herd immunity

Prevalence of meningococcal Meningitis

• major epidemics of meningococcal disease in Asia – China 1979 & 1980 – Vietnam 1977 – Mongolia 1973 -1974 & 1994 -1995 – Saudi Arabia 1987 – Yemen 1988 • Europe & the Americas – lower incidence of epidemics

Transmission & risk factors • Direct contact or via droplets from respiratory or throat secretions • Average incubation period: 4 days (2 -10 days) • household risk if exposed: increase by 400800 x • Transmission highest in 1 st week • Humoral immunity • Incidence highest in 6 -24 months of age • Some may be carrier for many years before becoming ill

Risk factors • Risk factors – Asplenia – Deficiency of properdin – Deficiency of antibody-dependent, complement mediated immune lysis – Household crowding – Active & passive smoking – Antecedent URTI (mycoplasma pneumonia or virus) – Chronic underlying illness • hepatic failure, SLE, multiple myeloma – HIV

Clinical menifestations

Clinical manifestations • 2 forms of meningococcal disease – Meningitis & meningococcal septicemia • Invasive meningococcal disease – Bacteremia without shock (acute mild meningococcemia) – Bacteremia with shock but no meningitis (fulminant meningococcemia) – Shock & meningitis – Meningitis alone – Chronic benign meningococcemia

Meningococcal meningitis • Hematogenous spread • 50 -55% of pts w meningococcal disease • Similar to other acute purulent meningitis

Signs & symptoms • • • Intense headache Fever Stiff neck Nausea Vomiting Photophobia Lethargy, drowsiness Rash Altered mental status ( elderly) Prolonged course w fever

Young children: signs • Subacute infection, progresses over several days • Irritability • Projectile vomiting • Seizures – usually with a focal onset – typically during the first few days • Infants – may have insidious onset – stiff neck & other classic signs may be absent

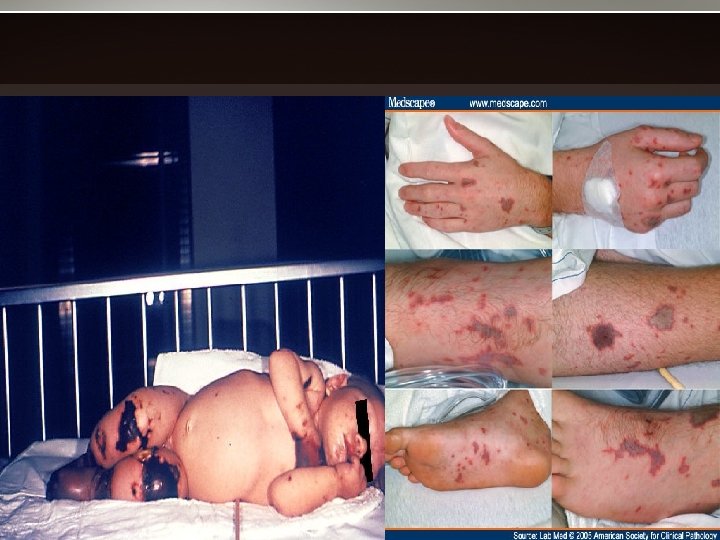
signs • nuchal rigidity • lethargy, delirium, coma, convulsions • only 70% has classic triad of fever, neck stiffness, & change in mental status. • petechial or purpuric rash – 12 -18 H after onset – 62% in >30 yo, 81% in younger pts – usually on the trunk, legs, mucous membranes, & conjunctivae – Occasionally on the palms & soles – may progress to purpura fulminans, associated with multiorgan failure


Nuchal rigidity

• meningococcal septicemia – Less common – rapid circulatory collapse & hemorrhagic rash. • Waterhouse-Friderichsen syndrome – widespread petechial hemorrhages – Hemorrhagic adrenalitis – septic shock – disseminated intravascular coagulation (DIC) • Neurologic sequelae – sensorineural deafness, mental retardation, spasticity & seizures
")
• <1% can present with – Spiking fever (over days to several weeks) – Arthralgia – Arthritis – Recurrent rash (chronic benign meningococcemia) • 20% later developed meningitis

Other infections due to N meningitidis • Compartmentalized metastatic infections • Pericarditis – Early (first few days): may demonstrate organism – Late (1 -2 weeks): sterile • Septic arthritis – late onset, after resolution of meningococcemia – Isolated, spontaneous • Others: – cellulitis, endophthalmitis, conjunctivitis, pneumonia, siadenitis, pelvic inflammatory disease

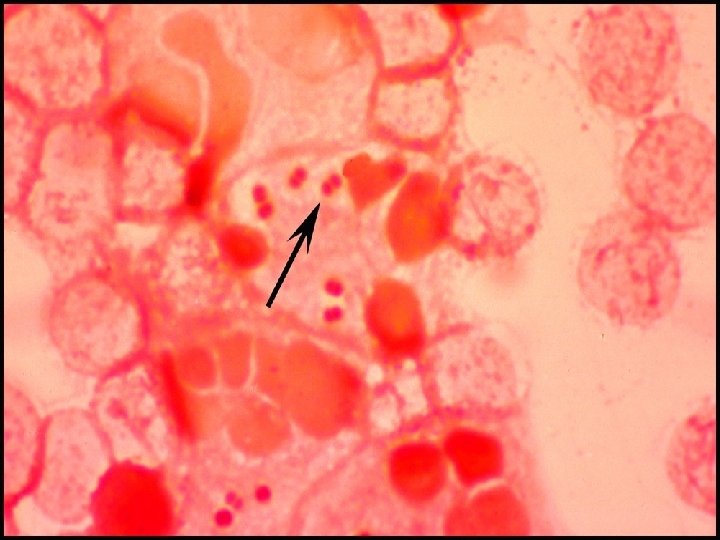
diagnosis • Gram Stain – positive in 70 -90% – GRAM NEGATIVE DIPLOCOCCI both inside & outside of polymorphonuclear cells • Direct antigen detection w latex agglutination • Culture from CSF – Positive in 80% • PCR – Not affected by prior initiation of antibiotics – sensitivity 97% & specificity 99. 6% – available within 2 H • Meningococcemia: skin biopsy

• Meningitis: only CSF generally positive • Body fluid may be positive in early onset compartmentalized infections • Blood culture – during febrile episodes are not consistently positive – Usually negative when afebrile

Antigen testing • Latex agglutination: detect capsular antigen of meningococcal serogroups A, B, C, Y, W 135 • Rapid, serogroup specific but not reliable • Negative GN or Ag detection does not rule out meningococcal disease

In clinical practice…. • Empirical treatment: based on the most likely organism • Institute antibiotics ASAP after LP • Avoid delays • Yield increased if specimen is examined ASAP – eg CSF should be examined within 1 H • CSF sterilization may occur more rapidly after initiation of parenteral antibiotics • complete sterilization within 2 H
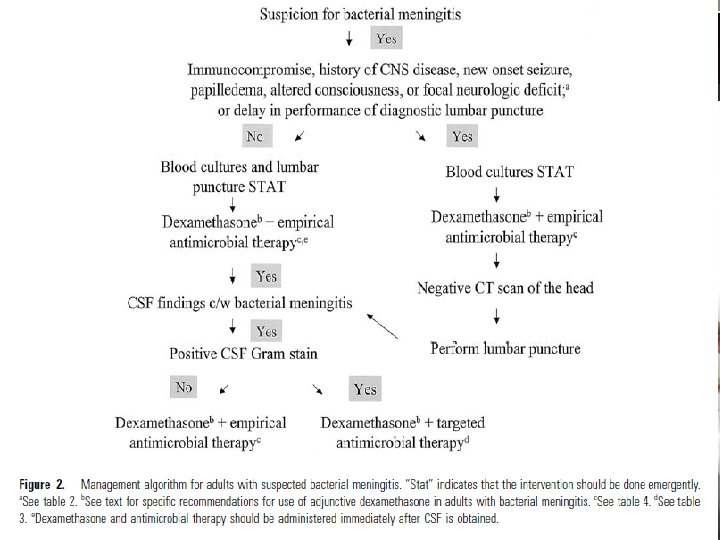

Lumbar puncture • Typical CSF abnormalities: – Increased opening pressure – Pleocytosis of polymorphonuclear leukocytosis • predominantly neutrophils – Decreased glucose (compare w serum glucose) – Increased protein
")
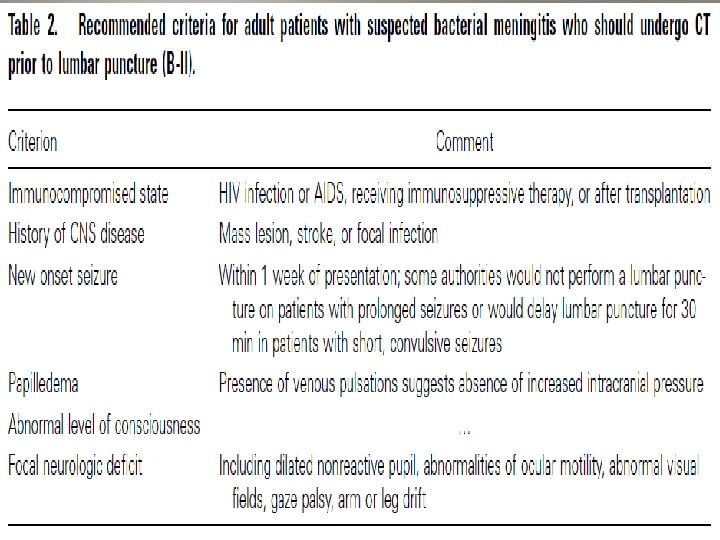
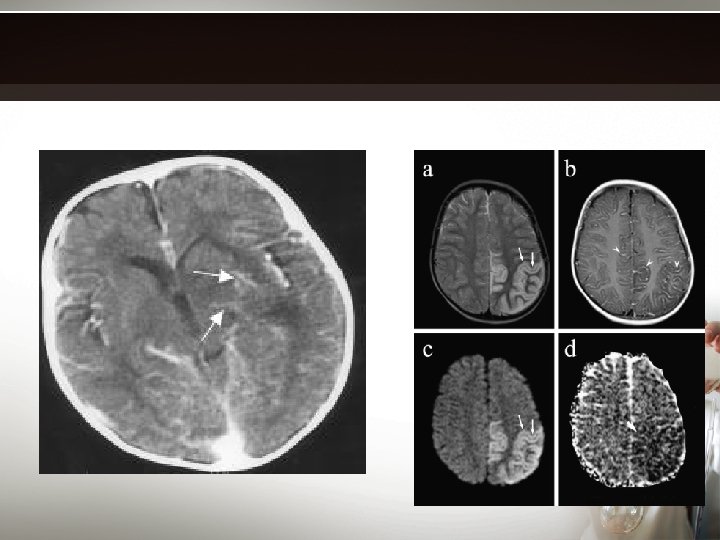
neuroimaging • Contrasted computed tomography – prior to lumbar puncture (? Risk of coning) – Demonstrates meningeal enhancement • Magnetic resonance imaging contrasted – demonstrates meningeal lesions, cerebral edema, & cerebral ischemia


management • Potentially fatal, should be treated as a medical emergency • Admission is necessary though isolation may not be necessary • Important to – Early recognition – Prompt initial parenteral antibiotics – Close monitoring
 • 3 rd generation")
Empirical management for suspected meningitis • Dexamethasone (controversial in adults) • 3 rd generation cephalosporin – ceftriaxone or cefotaxime • +/- Vancomycin • Acyclovir

Adjunctive dexamethasone in bacterial meningitis • Decrease cerebral edema & neuronal injury • Recommended for all suspected pneumococcal meningitis • 0. 15 mg/kg q 6 H x 2 -4 days • 1 st dose 10 -20 min before or at least concomitant with the antibiotics

• Significantly reduce unfavorable outcome & death • to be continued if confirmed S. pneumoniae • Data inadequate to recommend adjunctive dexa in meningitis caused by other bacterial pathogens
 – if penicillin resistance")
Definitive management • Penicillin or Ampicillin • Ceftriaxone (or cefotaxime) – if penicillin resistance • Despite adequate & early treatment, 510% die, typically within 24 -48 H after onset

Prevention

chemoprophylaxis • Prevention of sporadic meningococcal disease of close contacts of infected patients • Eradication of the carrier status • Mass chemoprophylaxis to control large outbreaks are not recommended – multiple sources of exposure & prolonged risk of exposure

• Ciprofloxacin 500 mg in a single dose – easiest option in adults. • Children could receive either – a single IM injection of ceftriaxone, or – 4 oral doses of rifampin over 2 days, according to BW. • commonly used – rifampin, ciprofloxacin, ceftriaxone, minocycline, & spiramycin. • Oily chloramphenicol – in areas with limited health facilities

Vaccination

Meningococcal vaccine: 3 types • Polysaccharide vaccines – Available >30 yrs ago – bivalent (groups A & C), trivalent (groups A, C & W), or tetravalent (groups A, C, Y & W 135) • outer membrane proteins (OMP) for serogroup B – No polysaccharide vaccines for serogroup B – Used in Cuba, New Zealand & Norway • Meningococcal conjugate vaccine – against group C: since 1999 – Tetravalent A, C, Y & W 135 conjugate vaccines: used since 2005 in Canada, USA & Europe.

Conjugate vs polysaccharide • advantages of conjugate vaccine – higher & more sustainable immune response against group A meningococcus – reduces the carriage & transmission of the bacteria in the throat – expected to confer long-term protection – cheaper – particularly effective in protecting children < 2 yo, who do not respond to conventional polysaccharide vaccines.
 • recommended")
Immunization • Primary vaccination: for older than 2 yrs (2 -55 yo) • recommended for adults & children at high risk • 3 months to 2 yrs under special circumstances (approved by FDA in August 2013) • High-risk persons – – – military recruits contacts to index cases travellers to areas of high incidence or outbreaks patients with asplenia adolescents with HIV infection persons with terminal complement disorders

Malaysian scenario • Vaccines available – Meningococcal A & C – Menomune A , C, Y, W-135 – Mencevax A, C, Y, W-135 • not routinely recommended • compulsory for the Hajj pilgrims & Umrah following the 1987 serogroup A meningococcal disease outbreak. • Since 1988, Malaysian Hajj pilgrims had received the bivalent A & C vaccine • Beginning 2002 Hajj, Saudi health officials require certification of quadrivalent meninggococcal vaccination covering serogroups A, C, Y, & W-135 for all entering pilgrims.

conclusion • Meningococcal meningitis has high mortality & morbidity rate. • All meningitides including the meningococcal meningitis should always be treated as medical emergency. • Early recognition & treatment are mandatory to prevent complications • chemoprophylaxis & mass vaccination to prevent further transmission, in susceptible individuals

Thank you

Meningococcal polysaccharide vaccine • • Quadrivalent: A, C, Y, W-135 Bivalent: A & C Primary vaccination: for older than 2 yrs (2 -55 yo) 3 months to 2 yrs under special circumstances (approved by FDA in August 2013) • Children: 2 doses 3 months apart • Ab response is serogroup specific & independent • Protective levels of ab are usually achieved within 7 days of vaccination

vaccination • Serogroup A polysaccharide: induce ab as early as 3 months of age • Adult: 4 -5 yrs • Serogp C: poorly immunogenic in children • Both serogp A &C: good immunogenicity, clinical efficacy≥ 85%

• Ab level & clinical efficacy reduced markedly during the first 3 yrs of vaccination • Detectable up to 10 yrs of vaccination • Multiple doses of serogroup A or C poly saccharide may cause tolerance • Adverse effects mild – Pain & redness (4 -56%) – Transient fever (4%) • Severe reaction: rare

• Drawback: absence of activity against serogroup B meningococci • Use of group B capsule in a vaccine risks the induction of autoimmunity • Ab response to group B is limited after natural infection hence group B capsular polysaccharide is poor candidate for vaccine replacement.

Conjugated polysaccharide vaccine • Quadrivalent • Induces T cell dependent response • Improve immune response, priming immunologic memory & leading to a booster response to subsequent doses • Long lasting immunity • Induces Herd immunity • 70% expected to be preventable

• • Safe Immunogenic Reduces the nasopharyngeal carriage rate Contraindicated in known allergy to any component of vaccine including the diphtheria toxoid • Routine childhood vaccination not recommended • Relative ineffectiveness in age <2 yo ( highest risk of sporadic disease & realtively short duration of protection)

• Routine vaccination recommended for certain gp w high risk – Autonomic or functional asplenia – Lab personnel & healthcare worker w are routinely exposed to N meningitidis • WHO: mass vaccinate every district in epidemic & alert phase • Single dose of polysaccharide for travelers> 18 months of age to epidemic or high rate of endemic meningococcal disease

revaccination • Persons high risk for infection, particularly children who were first vaccinated < 4 yo • To consider revaccination after 2 -3 yrs if risk still high
- Slides: 66