Meningococcal infection Part 2 n Lecturer Bynda Tatyana

Meningococcal infection Part 2 n Lecturer Bynda Tatyana

Meningococcal infection n Meningococcal infection is an acute infectious disease characterized by a variety of clinical forms, from nasopharyngitis to extensive forms such as meningococcemia, meningitis, meningoencephalitis, and more rarely with involvement of other organs and systems.

Susceptibility n Susceptibility is high in children 6 months - 5 years old. n The highest incidence - in Africa, especially in Central and Western (so-called "meningitis belt").

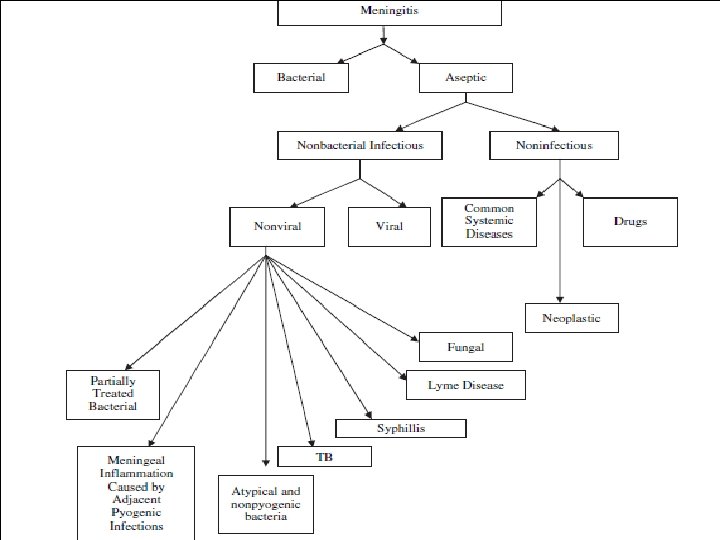
Definition Meningitis is the inflammation of the membranes surrounding the brain & spinal cord, including the dura, arachnoid & pia matter.

Meningitis

Incidence n Meningitis can occur at all ages but it is commonest in infancy. While 95% of the cases take place between 1 month 5 years of age. n It is more common in males than females.

Meningitis Disease often begins acutely and characterized by n sudden rise of body temperature, n severe headache, n vomiting without nausea and expressed hyperesthesia.

Meningitis The patient’s posture is usually typical: he is lying on his side with head tossed back and legs flexed to the abdomen.

Examination q Meningismus - check for nuchal rigidity with passive neck flexion (gives 'involuntary resistance).

Meningitis Stiffness of the occipital muscles develops very early (usually during the first 24 or 48 hours), and Kernig’s and Brudzinsky’s signs become positive. n
")
Brudzinski sign (hip & knee flexion with neck movement)
")
Kernig sign (extend knee with hip flexed)

Meningeal syndrome n suppression of skin rephlexes. n The abdomen is retracted.
, constant protrusion")
Meningitis n At children of early age - symptoms of suspension (L'essage), constant protrusion of fontanelle and tendency of the child to stretch neck to the back.

Meningitis In newborns and small infants, the classic symptoms of fever, headache, and neck stiffness may be absent or difficult to detect, and the infant may only appear slow or inactive, or be irritable, have vomiting, or be feeding poorly. As the disease progresses, patients of any age may have seizures.

Meningitis Red dermographism is very common Herpes often occurs on the lips.
, neutrophilosis with")
Meningitis n The blood shows marked leukocytosis (up to 20– 40· 109/l), neutrophilosis with a shift to the left, aneosinophilia; the ESR is considerably increased.

Meningitis n In lumbar puncture spinal fluid flows under increased pressure (300– 500 mm H 2 O). n During the first day of illness it may be transparent or slightly opalescent, but later becomes turbid and purulent.
 and a considerable protein content (up to")
Meningitis It displays marked neutrophilosis (neutrophilous pleocytosis) and a considerable protein content (up to 1– 2 g/l, or 1– 2 %); sugar content is lowered.

Meningitis n Bacterioscopy shows meningococci within and out of cells; n but microbiological investigation - culturing of spinal fluid - is a more reliable means of revealing meningococci.

Determination Normal Range Syndrome meningism Viral meningitis Bacterial meningitis Colour colourless milk, greenish Transparency transparent turbid Cells count (in 1 -10 1 ml) lymphocytes 80 -85 % neutrophils 3 -5 % 1 -3 20 -1000 -15000 80 -85 % 3 -5 % 80 -100 % 0 -20 % 0 -60 % 40 -100 % Protein, g/l 0, 16 -0, 45 0, 33 -1, 0 0, 66 -16, 0 Pandi reaction “-” “+“, “++” “+++“, “++++ cerebrospinal pressure 200 -250 200 -300 0, 16 -0, 24 130 -180

n The gravity and course of meningococcal infection differ in various patients. n The clinical manifestations are also quite varied. n Especially grave are encephalitic, septic (meningococcemia) and hypertoxic forms.
.")
Encephalitis: is the infection of brain tissue (cortex and medulla).

n The encephalitic form is seen mainly in infants and has a prevalence of cortical symptoms, namely n mental disturbances, n convulsions, n focal phenomena (paresis, paralysis). n The meningeal symptoms may be trivial.
 form all the symptoms are weakly expressed, including the")
n In the rudimentary (abortive) form all the symptoms are weakly expressed, including the meningeal. n The changes in the cerebrospinal fluid may be insignificant and transitory.
 form of MI has a sudden turbulent onset and is")
n The hypertoxic (fulminating) form of MI has a sudden turbulent onset and is characterized by severe toxemia (uncontrollable vomiting, convulsions, mental confusion, cardiovascular weakness). n The patient soon becomes comatose. n Meningeal symptoms are sharply pronounced or, on the contrary, rudimentary. n Death usually ensues within 12 to 24 hours after the onset. Swelling of the brain and protrusion of the cerebellar tonsils into the great foramen is one of the frequent causes of death.

n The fulminating form may develop as the Waterhouse - Frederickson syndrome which is the signs of an acute renal insufficiency. n Multiple petechial rashes and hemorrhage into the skin (resembling livers) are characteristic. n The arterial pressure falls progressively, the pulse is rapid and hardly palpable. Cyanosis, vomiting (often with blood) and convulsions are other signs. The patient dies in 16– 30 hours after the onset of the disease unless an urgent and effective therapy is given.

Meningococcal meningoencephalitis The disease develops when the inflammation passes to the matter of the brain. Since the first days of the disease encephalitic signs predominate: n focal character of manifestations (that is direct correlation between an area in the brain and the systems or organs involved), n pathological reflexes, n stable paresis and paralysis, n affection of the cranial nerves, n psychic disturbances, and drowsiness.
 is also one of")
n Meningococcal meningitis in combination with meningococcemia (a mixed form) is also one of the extensive forms. n This is the most frequent form of meningococcal infection in children. n In this pathology clinical manifestations of meningococcemia appear a bit earlier than the involvement of the maters.

Features peculiar to meningitis in infants n Onset of the disease is accompanied with high temperature, general restlessness, vomiting, and refusal to suckle. n There is marked hyperesthesia of the integuments and frequent dyspeptic disturbances. n Infants cry loudly. n Meningeal symptoms and red dermographism are often mild or absent. n Tension and protrusion of the unossified anterior fontanel are apparent at the beginning of the disease.

Features peculiar to meningitis in infants n In the newborn the course of meningitis as a rule is atypical. n High temperature, convulsions or tremor, and general muscular hypertension develop. n Meningeal symptoms are absent or become apparent only with further the disease course. n Even with modern methods of treatment mortality remains high among the newborns and infants less than three months old.

THE MAIN DIAGNOSTIC SIGNS OF MI 1. Taking history: if there has been a contact with a patient with nasopharyngitis or a meningococcus carrier. 2. The onset is acute or sudden with marked toxicosis developing quickly. 3. Meningeal syndrome is always marked. 4. A characteristic feature is an early hemorrhagic rash with necrosis in the center, star-shaped. 5. Lethal outcome is due to the development of lifethreatening complications: cerebral edema and infectious-toxic shock with acute adrenal failure.

n CBC Investigations n Blood culture n Gram staining n LP - D/r, C/s (color, leukocyte count, differential, glucose, protein) n Electrolytes n PCR (polymerase chain reaction) n Coagulation profile n liver and kidney function n Chest X-ray n CT (Computed Tomography) / MRI (magnetic resonance imaging) n Blood gases n EEG n ECG

Diagnosis n Latex particle agglutination: detects presence of bacterial antigen in the spinal fluid. Useful for detection of H. influenzae type b, S. Pnemoniae, N. Meningitidis, E. Coli. n Concurrent immuno-electrophoresis (CIE)-used for rapid detection of H. influenza, S. pneumoniae & N. meningitides. n Smears: taken from purpuric spots may show meningococci in Meningococcaemia. n DNA sequences: are helpful in identifying bacteria

Diagnosis n CSF picture is quite diagnostic of the kind of meningitis present.

LABORATORY DIAGNOSIS If meningitis is suspected, lumbar puncture is performed. In studying liquor, elevated pressure (up to more than 200 -250 (conventional) millimeters water-column), cytosis up to several thousand per 1 µL (microliter), protein contents up to 0. 66 -2 g/L are revealed. Sugar and chloride content may decrease.

LABORATORY DIAGNOSIS 2. Complete blood count shows leukocytosis, a shift to the left to myelocytes, elevated ESR. The degree of these changes is proportional to the severity of the disease.

If meningitis is suspected, lumbar puncture is performed Contraindication for LP n. Increase intracranial pressure. n. Unstable patient. n. Skin infection at site of LP. n. Thrombocytopenia. n. Papilloedema.

COMPLICATIONS OF M I EARLY LATE n Infectious-toxic shock n Affection of intellect n Hypertension n Edema of the brain syndrome n Hydrocephaly (disseminated intravascular clotting) n Epileptic syndrome n Paralysis and n Acute adrenal failure paresis n Cerebral hypotension n Hearing disturbance n Subdural effusion n Ependymitis n DIC-syndrome

DIFFERENTIAL DIAGNOSIS Differential diagnosis is made with n n n the diseases accompanying by marked toxicosis and eruption, namely: The grippe (influenza), Typhoid fever, Hemorrhagic vasculitis, Measles, scarlet fever, yersiniosis, meningitis of other etiology, and Subarachnoid hemorrhage.

TB Fungal Lyme Partially Treated Bacterial Viral CSF finding < 300 < 500 > 1000[ < 1000 Leukocytes/mm 3 < 10– 20% < 10% > 85– 90% 20– 40% Polymorphonuclea r cells > 200– 300 > 100– 200 < 100 60–> 100– 150 N or < 100 Protein (mg/d. L) < 40 N < 40 UD to < 40 N Glucose (mg/d. L) < 0. 4 N Blood-to-glucose ratio < 30% < 40% - ≥ 80% > 85% - Positive smear < 30% > 30% - < 90% > 95% Rare Positive culture Mycobacterium tuberculosis Histoplasma and Cryptococcus antigen, India ink for Cryptococcus Borrelia burdgorferi antibodies 16 S RNA, bacterial Enterovirus, DNA herpesvirus PCR or other methods

Pre-hospital stage of treatment n Catheterization of the vein. n Antibacterial therapy: Cephtriaxonum - 100 mg/ kg/day, each 12 hours. Cephotaximum - 200 mg/kg/day. each 8 hours. Levomycetin sodium succinate by 25 mg/kg (a single doze) intravenously. n Glucocorticoids - Prednisolon, Hydrocortison or Dexazonum by 2 -3 mg/kg by Prednisolon – without ITS, n 5 mg/kg — at ITS of 1 degree, n 10 mg/kg- at ITS of 2 degree, n 15 -20 mg/kg - at ITS of 3 degree.

Pre-hospital stage of treatment n Infusive therapy by saline solutions or n n rheopolyglucin for stabilization of CBV (Circulating Blood Volume). Inotropic drugs (dopamine) - for hemodynamics support. Antipyretics. Furosemide - 1 -2 mg/kg. For seizures - Diazepam.

Treatment in hospital: Supportive therapy: n Maintain fluid & electrolyte balance as required n Transfuse whole blood, PRC, FFP or platelets as required. n Maintain temperature control n Monitor OFC n Fresh frozen plasma- contains clotting factors and plasma proteins. Is used to reverse coagulapathes. PRC- packed red cells, the same as packed cells.

Treatment n Ampicillin 300 mg/kg/day+ n Initial till results of n Chloramphenicol C/S are known 75 -100 mg/kg/day IV n Probable/Proved n Penicillins Meningococci 300. 000 U/kg/d IV q 4 h until 5 -7 d after normal temperature

Treatment in hospital: Antibiotics of a reserve: n Cephtriaxonum - 100 mg/ kg/day, each 12 hours. n Cephotaximum - 200 mg/kg/day each 8 hours. n At presence ITS - Levomycetin sodium (Chloramphenicol) succinate - 100 mg/kg/day.

Treatment in hospital: In case of severe form and necessity of protection from nosocomial infection in addition aminoglicosides of 3 -rd generation prescribed. Amykacin up to 20 mg/kg/day, Nethylmycinum 4, 5 -7, 5 mg/kg/day.
 Neonates, age in days Antimicrobial agent 0")
Total daily dose (dosing interval in hours) Neonates, age in days Antimicrobial agent 0 - 7 8 - 28 Infants and children Adults Amikacinb 15 20 mg/kg (12) 30 mg/kg (8) 20 30 mg/kg (8) 15 mg/kg (8) Ampicillin 150 mg/kg (8) 200 mg/kg (6 - 8) 300 mg/kg (6) 12 g (4) Aztreonam . . . Cefepime . . . Cefotaxime 100 -150 mg/kg (8 - 12) Ceftazidime 100 150 mg/kg (8 12) Ceftriaxone Chloramphenicol . . . 25 mg/kg (24) . . . 6 8 g (6 8) 150 mg/kg (8) 6 g (8) 150 - 200 mg/kg (6 -8) 225 - 300 mg/kg (6 - 8) 8 12 g (4 6) 150 mg/kg (8) 6 g (8) 80 - 100 mg/kg (12 - 24) 4 g (12 24) 75 100 mg/kg (6) 4 6 g (6)c . . . 50 mg/kg (12 24) Ciprofloxacin . . 800 1200 mg (8 12) Gatifloxacin . . 400 mg (24)d Gentamicinb 5 mg/kg (12) 7. 5 mg/kg (8) Meropenem . . . Moxifloxacin . . . 7. 5 mg/kg (8) 120 mg/kg (8) 6 g (8) . . . 400 mg (24)d Nafcillin 75 mg/kg (8 12) 100 150 mg/kg (6 8) 200 mg/kg (6) 9 12 g (4) Oxacillin 75 mg/kg (8 12) 150 200 mg/kg (6 8) 200 mg/kg (6) 9 12 g (4) Penicillin G 0. 15 m. U/kg (8 12) 0. 2 m. U/kg (6 8) 0. 3 m. U/kg (4 6) 24 m. U (4) 10 20 mg/kg (12 24)e 600 mg (24) 7. 5 mg/kg (8) 10 20 mg/kg (6 12) 60 mg/kg (6) 30 45 mg/kg (8 12) Rifampin Tobramycinb TMP-SMZf Vancomycing . . . 5 mg/kg (12). . . 20 - 30 mg/kg (8 - 12) . . . 30 - 45 mg/kg (6 - 8)

Duration of therapy Microorganism Neisseria meningitidis Haemophilus influenzae Streptococcus pneumoniae Streptococcus agalactiae Duration of therapy, days 7 7 10 - 14 14 - 21 Aerobic gram-negative bacilli 21 Listeria monocytogenes 21 Tunkel A, Hartman B et al. Practice Guidelines for the Management of Bacterial Meningitis. Clinical Infectious Diseases 2004; 39: 1267 -1284 / IDSA Guidelines.

TAKING ANTIBIOTICS STOPS if: n The general condition has become better. n Meningeal and intoxication signs have disappeared. n The body temperature is stable. n Normalization of the CSF: cytosis does not exceed 50 -100 cells per 1 µL, and 100% of the cells are lymphocytes. n If pleocytosis is neutrophilic, introduction of antibiotics is continued in the same dose for another 2 -3 days.

Treatment in hospital: n Detoxycation with saline or water solutions 2: 1. n Saline solutions include: crioplasm, albumin, rheopolyglucin, saline. n Water solution is isotonic glucose. n In case of meningitis amount of liquid for infants must not exceed 50 ml/kg/day, and not more then 20 -30 ml/kg in one infusion.

Treatment n Correction of temperature of the body; n Hyperpyrexia: Tepid sponging, correction of dehydration. n Anticonvulsants – 0, 5 % seduxen (Diazepam) 0, 3 -0, 5 mg/kg i/m or i/v. Can be repeated q 4 hours as required. n Cerebral edema: *I. V Mannitol 1 g/kg in 20 -30 mins 6 -8 hourly given for first few days.

Steroids : Anti-inflammatory agents n First dose should be given 1 hr prior to starting antibiotics. n Dexamethazone: 0. 15 mg / kg / dose, given IV every 6 hr for 4 days. n Corticosteroids (prednisolon) for 3 -5 days: n in case of meningitis, meningoencephalitis - 1 -5 mg/kg/day in 2 doses; n in case of meningococcemia typical 5 -10 mg/kg/day in 2 -4 equal doses; n in case of fulminant meningococcemia prednisolon – 10 -20 mg/kg/day, hydrocortisone - 20 -30 mg/kg/day in 4 equal doses;
 heparin 50 -100 U/kg every 6 hrs.")
n Anticoagulants for haemorrhagic syndrome (according coagulogram) heparin 50 -100 U/kg every 6 hrs. n Acetazolam (diacarb) + asparcam, the dose is selected depending on expressiveness of hypertensive syndrome.

n Syndromic therapy is performed according to corresponding standards. n In the period of convalescence in case of meningitis, meningoencephalitis: nootropic drugs and vitamins of group B.

CRITERIA OF DISCHARGE FROM THE HOSPITAL OF CONVALESCENTS n Complete clinical recovery n Normalization of findings of laboratory tests n Negative results of 2 bacteriological studies of nasopharyngeal mucus for meningococcus. n The investigation is made three days after treatment with antibiotics and interval of 12 days between the tests.

Prognosis n Prognosis is usually good with early detection and prompt antibiotic therapy. n However bad prognosis either mortality or morbidity will occur among untreated cases, late recognition, infant less than 6 months, seizures occurring more than 4 days into therapy, or occurrence of coma.

Prognosis n It depends on the age of the patient, the duration of the illness, complications, microorganism & immune status. n The prognosis is worse for patients at the extremes of age (ie ( , <2 y, >60 y) and those with significant comorbidities and underlying immunodeficiency. n Patients presenting with an impaired level of consciousness are at increased risk for developing neurologic sequelae or dying.

Prognosis n A seizure during an episode of meningitis also is a risk factor for mortality or neurologic sequelae. n Acute bacterial meningitis is a medical emergency and delays in instituting effective antimicrobial therapy result in increased morbidity and mortality. n The prognosis of meningitis caused by opportunistic pathogens depends on the underlying immune function of the host as may require lifelong suppressive therapy.
 by erythromycin, chloramphenicol, sulfonamides for 3 -5 days")
Prophylaxis n Chemoprophylaxis (sanation of carriers) by erythromycin, chloramphenicol, sulfonamides for 3 -5 days or Rifampin ( 20 mg/kg/dose every day for 4 days). n Quarantine for 10 days, looking after contacts with one bacteriological test of nasopharyngeal culture.

SPECIFIC PROPHYLAXIS Active immunization of meningococcal vaccine is carried out. There is a monovalent vaccine (A), bivalent vaccine (A and C), and quadrivalent vaccine (A, C, Y, W-135), which cause multiplication of antibodies and prevention from the disease since the 5 th day after introduction.
- Slides: 62