Menieres Disease DR ABHISHEK BHARDWAJ Introduction Idiopathic endolymphatic

Meniere’s Disease DR. ABHISHEK BHARDWAJ

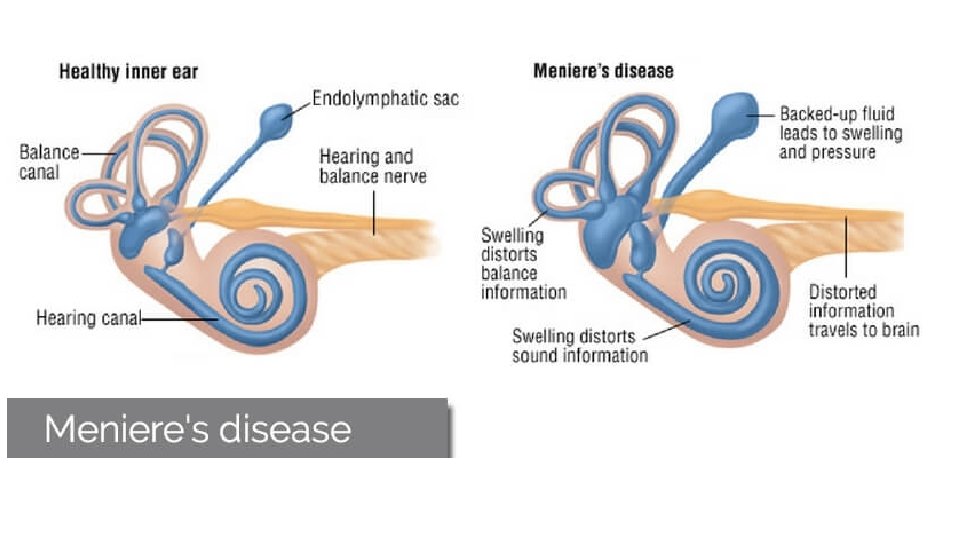
Introduction • Idiopathic endolymphatic hydrops • Prosper Meniere first described the symptom complex in 1861

Epidemiology • More prevalent among whites • Male-to-female ratio approximately 1 • Peak age at onset is in the 40 -50 years • Mode of inheritance can be variable

Etiology • Considered to be idiopathic The possible etiologies include • Antibodies directed against normal inner ear elements • Viral infection • Ischemia of the endolymphatic sac or inner ear

Meniere's syndrome • Many different inner ear or temporal bone diseases, such as syphilis, mumps, Cogan's syndrome, trauma and even chronic suppurative otitis media, can after many years, produce the clinical picture of Meniere's disease.

Pathogenesis • Endolymph is produced by the stria vascularis in cochlea and dark cells in vestibular labyrinth • Endolymphatic duct may act as a valve to regulate endolymph homeostasis

hypoplasia of the endolymphatic sac and duct inadequate absorption of endolymph by the endolymphatic sac endolymphatic hydrops overaccumulation of endolymph

• Schuknecht hypothesis Ruptures in the membranous labyrinth leakage of the potassium-rich endolymph into the perilymph, bathing the eighth cranial nerve and lateral sides of the hair cells High concentrations of extracellular potassium depolarize the nerve cells, causing their acute inactivation decrease in auditory and vestibular neuronal outflow consistent with symptoms

Healing of the membranes is presumed to allow restitution of the normal chemical milieu, with termination of the attack chronic deterioration in inner ear function presumably is the effect of repeated exposure to the effects of the potassium

• Acute attacks are superimposed on a gradual deterioration in sensorineural hearing in the involved ear, typically in the low frequencies initially. • Over time, a reduction in responsiveness of the involved peripheral vestibular system occurs.
 -tinnitus")
Clinical Presentation • Typical history consists of recurring attacks of -vertigo (96. 2%) -tinnitus (91. 1%) -ipsilateral hearing loss (87. 7%). • Tinnitus >nonpulsatile

• Attacks often are preceded by an aura consisting of a sense of fullness in the ear, increasing tinnitus, and a decrease in hearing. • Attacks lasting longer than a day are unusual and if present should cast doubt on the diagnosis.

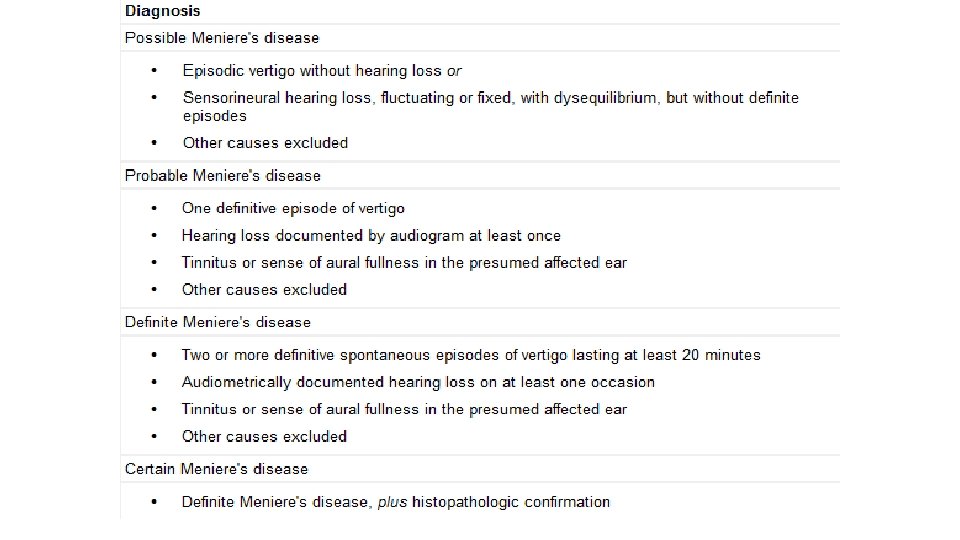
AAO-HNS Criteria for Meniere's Disease Diagnosis

• In most patients, only one ear is affected in the early stages of Meniere's disease. • Unfortunately, the second ear eventually becomes involved in about half of the patients with this condition.

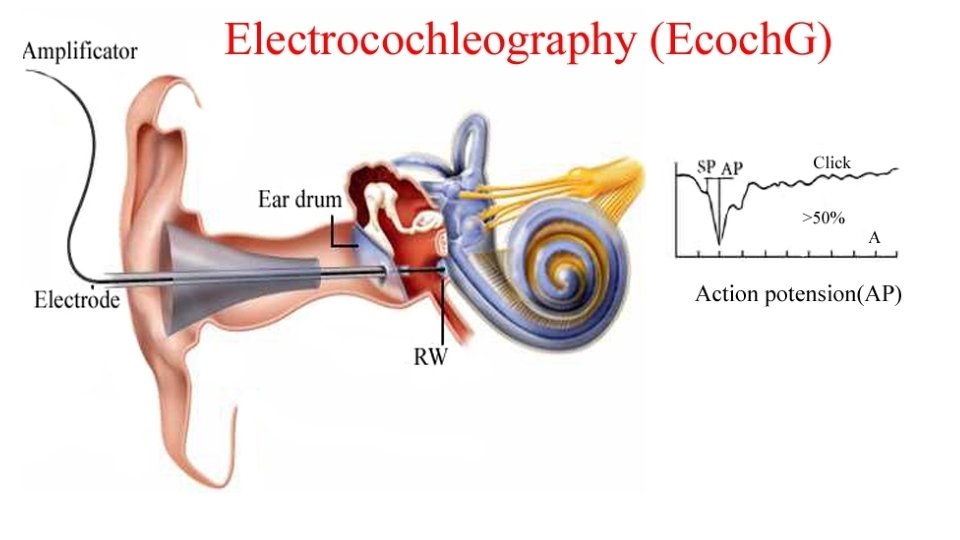
Investigations • Electronystagmography -Electrooculographic recordings of eye movements after caloric and rotational stimulation • Electrocochleography -increased summating potential and SP/AP ratio -low specificity -infrequently used

• Dehydrating Agents -eg. urea, glycerol, furosemide -goal is to reduce the volume abnormalities in the inner ear and produce a measurable change in response

VEMP

• Vestibular Evoked Myopotentials -generated by playing loud clicks in the ear, which move the stapes footplate and stimulate the saccule -disynaptic pathway that passes through the vestibular nuclei and then to synapses that relax the sternocleomastoid muscle

• Saccule is the second most common site affected by hydrops • Ears affected by Meniere's disease have elevated VEMP thresholds with flattened tuning • Limited diagnostic value owing to the large individual variation

Treatment • Currently, almost all proven therapies are directed at relieving vertigo, which usually is the most distressing symptom • Salt restriction -restrict salt intake to 1 mg or 1. 5 -2 mg per day.

• Vasodilators Betahistine, an oral preparation of histamine • Diuretics – Bendroflurozide, Dyazide, Chlorthalidone • Carbonic anhydrase inhibitors such as acetazolamide

• Symptomatic Treatment -Antivertiginous medications, antiemetics, sedatives, antidepressants, and psychiatric treatment • Local Overpressure Therapy (? ? ? ) eg. Meniett device -handheld air pressure generator that the patient self-administers -device requires a ventilation tube to be placed in the tympanic membrane before initiation of therapy

• Intratympanic Injection with either dexamethasone or gentamicin -Gentamicin is predominantly vestibulotoxic and acts by destroying the dark cells of the secretory epithelium, thus decreasing endolymph production.

• Endolymphatic Sac Surgery • -first described by Portmann in 1926 • -may result in a reduction in vertigo attacks but has no benefits for the auditory symptoms. Several variations - Simple decompression -wide decompression that includes the sigmoid sinus -cannulating the endolymphatic duct -endolymphatic drainage to the subarchnoid space -drainage to the mastoid removal of the extraosseous portion of the sac

• Nerve Section of the vestibular nerve -retrosigmoid approach -middle fossa approach -retrolabyrinthine approach • Labyrinthectomy -uniform destruction of hearing and vestibular function

• Patients who have no further vertigo attacks and little tinnitus – so called burnt-out Meniere's disease.

THANK YOU
- Slides: 33