Memory Screening Testing Protocols for Detection and Monitoring



")






 in 2003, National Memory Screening enables")

 (Voluntary Participant Survey")
")


 Sex Male 1, 257")
 GP-Cog - General Practitioner assessment of Cognition 1369 45% Mini-Cog")


 ROC for Univ. Kentucky ADRC Clinic Cases Schmitt et al.")
 Benefit of a true")
 – ($C x")


 • Also detect: fronto-temporal")
 • CRT is widely used academically")
 and age on the audience-based continuous recognition test")
 and age in 868 individuals on the continuous")
 and age in 868 individuals on the continuous")
 • • • Test to screen for")


 (males, females separated) - Number of subjects")

 1500")




- Slides: 48
Memory Screening: Testing Protocols for Detection and Monitoring J. Wesson Ashford, M. D. , Ph. D. Clinical Professor (affiliated), Department of Psychiatry and Behavioral Sciences Senior Research Scientist, Stanford / VA Alzheimer’s Disease and Aging Clinical Research Center Stanford University and VA Palo Alto Health Care System Chair, Alzheimer’s Foundation of America, National Memory Screening Advisory Board February 26, 2016 Slides at: www. medafile. com (Dr. Ashford’s lectures)
Financial Disclosure • Dr. Ashford has been developing memory tests for assessment of neuropsychiatric illnesses since 1979. • Dr. Ashford has never made any money from developing these tests, though he has spent a small amount of funds maintaining websites to make some of these tests available for free: www. medafile. com. • Dr. Ashford’s son, Curtis Ashford, has a company, Mem. Trax, LLC, which owns the trademark, Mem. Trax. • Mem. Trax, LLC is working to commercialize a Continuous Recognition Test: www. memtrax. com • The USA Internal Revenue Service considers Dr. Ashford’s activities with respect to Mem. Trax to be a “hobby”
3
AFA Resources and Support • AFA’s National Toll-free Helpline – (phone, email, Skype, chat) – 866 -232 -8484 • Dementia Care Professionals of America- training and certification • Care Connection monthly teleconference • National Memory Screening Program • Educational training, resources, and conferences • AFA Care Quarterly magazine • AFA unites 2, 400+ member organizations nationwide that provide direct resources and care www. alzfdn. org 866 -232 -8484
Dementia is Under-diagnosed • Early dementia is easily missed – – especially Alzheimer’s disease (AD) the problem is subtle – MCI – mild cognitive impairment family members avoid the problem and compensate for the patient physicians tend to miss the initial signs and symptoms • about 90% of AD cases are missed early • Many AD patients are never recognized for their disease – Estimates are that 25% to 50% of cases remain undiagnosed – Diagnoses are still missed at moderate and severe levels • No definitive laboratory test for diagnosing AD exists – Efforts to develop biomarkers – none currently accepted – Early recognition by brain scan is confusing (may rule out AD)
Reasons to Diagnose Alzheimer’s Disease Early Social / Financial • Undiagnosed patients face avoidable problems: – social, financial problems • Early education of caregivers of how to handle patient • Advance planning while patient is competent – will, proxy, power of attorney, advance directives • Reduce family stress and misunderstanding (blame, denial) • Promote safety (driving, compliance, cooking, etc. ) • Patient’s and family’s right to know, including genetic risks • Opportunity to reduce caregiver burden • Promote advocacy for research and treatment development
Reasons to Diagnose Alzheimer’s Disease Early Medical • Early diagnosis and appropriate intervention may lessen disease burden and early treatment may improve overall course substantially – Neurophysiological pathways in patients with AD are still viable and are a target for treatment • Specific treatments now available (after dementia diagnosis) – anti-cholinesterases, memantine) – Improve cognition – Improve function (ADLs) – Slow dementing process, earlier treatment is better – Decrease development of behavior problems – Delay nursing home placement, possibly over 20 months – Delay nursing home placement longer if started earlier
Introducing the time-index model of the course of Alzheimer’s disease (calculated from the CERAD data set) The best model to fit the progression, both mathematically and biologically, is the Gompertz survival curve (99. 7% fit to mean changes over time): S(t) = exp(Ro/alpha *(1 - exp (alpha * t))) Time-Index Scale AAMI / MCI/ early AD -- DEMENTIA Ashford et al. , 1995
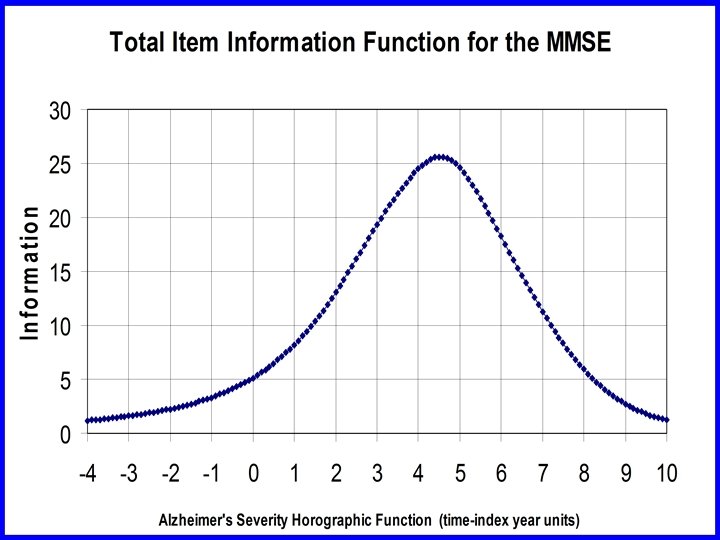
Mini-Mental State Exam items
Problems with the MMSE • Mini-Mental State Exam – Folstein et al. , 1975 (antique) • Considerable noise • Several items do not provide adequate information • Poor range for measuring change – Large standard error of measurement • Poor power for assessing medication benefit • Inadequate screening tool • Better, shorter tests are available • Now, copyright is being enforced (not free!!)
Launched by the Alzheimer’s Foundation of America (AFA) in 2003, National Memory Screening enables thousands of local sites nationwide to provide free, confidential memory screenings to individuals concerned about memory loss with the objective of early detection and intervention. • • Since the inception of the program, over 2. 5 million people have been screened. Memory screenings are taking place in all 50 states and Puerto Rico. Screenings take place year round and during National Memory Screening Month (which is November in conjunction with Alzheimer’s Awareness Month)
Memory screenings: Free and confidential Take approximately 10 minutes. Consist of a series of questions to gauge memory, language and thinking skills. Results are not a diagnosis, but a memory screening can suggest if someone should see a physician for a full evaluation. To search for a screening site in your area visit: www. nationalmemoryscreening. org To register to become a memory screening site visit: www. afascreenings. org/register AFA provides sites with all of the necessary materials to carry out the screenings- free of charge!
What is the reason you came today? (Check all that apply) (Voluntary Participant Survey – NMSD 2015) I have noticed changes in my memory over the last year I feel I have more problems with my memory than most other people my age My family or friends have encouraged me to get screened I have relatives with Alzheimer’s disease or dementia 42% 11% 10% 20% I have been a caregiver for someone with AD or dementia 8% I have been diagnosed with memory loss 2% I feel regular memory screening is important 40% Other 13%
Have you ever had a memory test before? (Voluntary Participant Survey – NMSD 2015) No I have not had a memory test before At a NMSD in the past At a health fair In my doctor’s office On a computer Other 78% 3% 2. 5% 7% 1% 6%
CLINICAL TOOLS FOR COGNITIVE SCREENING 116 listed by NIA, including: • • • MINI-MENTAL STATE EXAM MIS (Memory Impairment Screen) Mini-Cog GP-Cog Brief Alzheimer Screen (BAS) 7 -Minute Screen MOCA (Montreal Cognitive Assessment) SLUMS (St. Louis Mental Status test) GLOBAL CLINICAL SCALE Continuous Recognition Test https: //www. nia. nih. gov/research/cognitive-instrument
National Memory Screening Day NMSD - 2010 • 2334 sites participated • e. g. , Alzheimer’s agencies, pharmacies, hospitals, community centers • estimated 60, 000 individuals were screened • 48 sites agreed to provide data to the AFA • Information was provided on 4, 396 individuals • A mean of 55 +/- 34 participants were seen at each site (range 5– 159) Bayley et al. 2015
Demographic Characteristics of Participants- NMSD - 2010 Characteristic n (%) Sex Male 1, 257 (28. 8) Female 3, 109 (71. 2) Age <35: 40 (0. 9) 35– 44: 57 (1. 3) 55– 64: 604 (13. 8) 65– 74: 1, 330 (30. 5) 75– 84: 1, 524 (34. 9) >85: 617 (14. 1) Black 320 (7. 4) Other 221 (5. 1) > High School 356 (8. 3) Bachelor’s degree 865 (20. 2) Postbachelor’s 1, 192 (27. 9) 45– 54: 190 (4. 4) Race White 3, 757 (87. 4) Hispanic 188 (4. 3) Education Elementary 197 (4. 5) High school 1, 666 (39. 0)
Tests Administered (number, percent) GP-Cog - General Practitioner assessment of Cognition 1369 45% Mini-Cog 686 23% MIS - Memory Impairment Screen 249 8% Mini-Mental State Examination 452 15% 71 2% 201 7% 9 0% Kokmen Short Test of Mental Status Mo. CA - Montreal Cognitive Assessment SLUMS - Saint Louis University Mental Status Examination
Time to Administer Available Short Screening Tests • MMSE 10 -- 15 min • Too long, poor screener • 7 -Minute Screen 7 – 10 min • Too complex • Brief Alzheimer Screen (BAS) 2 – 4 min • High sensitivity, specificity, only one form • Mini-cog 3 – 5 min • Unclear sensitivity, specificity • Memory Impairment Screen 4 min • Need shorter, easier to perform test • (a suitably accurate test that takes less than 2 minutes is not available)
JW Ashford, MD Ph. D, 2003
Brief Alzheimer Screen (BAS) ROC for Univ. Kentucky ADRC Clinic Cases Schmitt et al. , 2006
Factors for Deciding whether a Screening Test is Cost-Effective 1) Benefit of a true positive screen 2) Benefit of a true negative screen 3) Cost of a false positive screen (? Harm) 4) Cost of a false negative screen (? Harm) 5) Incidence of the disease (in population – increasing) 6) Test sensitivity (in population) 7) Test specificity (in population) 8) Test cost (include cost of test administrator)
$W = Cost–Worthiness Calculation $W > ($B x I x Se) – ($C x (1 -I) x (1 -Sp)) - $T • BENEFIT – $B = benefit of a true positive diagnosis • Earlier diagnosis may mean proportionally greater savings • Estimate: (100 years – age ) x $1000 • Save up to $50, 000 (e. g. , nursing home cost for 1 year) – (after treatment cost deduction at age 50, none at age 100) – (cost-savings may vary according to your locale) • • • – True negative = real peace of mind (no money) COST – $C = cost of a false positive diagnosis • $500 for further evaluation – (time, stress of suspecting dementia) – False negative = false peace of mind (no price) I = incidence (new occurrences each year, by age) Se = sensitivity of test = True positive / I Sp = specificity of test = True negative / (1 -I) = (1 -False positive/(1 -I) $T = cost of test, time to take (Subject, Tester) Kraemer, Evaluating Medical Tests, Sage, 1992
Se, Sp
Need to Develop Better Screening and Early Assessment Tools • • Genetic vulnerability testing (trait risk) Vulnerability factors (education, occupation, head injury) Early recognition (10 warning signs), ADLs Positive diagnostic tests – CSF – tau levels elevated, amyloid levels low – Brain scan – PET – amyloid, tau ligands • Screening tools (6 th vital sign in elderly) • Mild Cognitive Impairment assessments • Detecting early change over time – predicting progression, measuring rate
Cognitive Impairment Assessment • Detect Alzheimer’s disease (universal screening test) • Also detect: fronto-temporal dementia, mild traumatic brain injury, intoxication, safety to operate machinery & drive, mild cognitive impairment, other types of dementia, chemobrain, etc. ) • Be on multiple platforms: – Computer for rapid, objective assessment – World-Wide Web – for testing anywhere – Doctor’s offices – Smart-phone, tablets (HTML-5) – KIOSK administration – drug stores, shopping malls • Be very brief (1 to 2 minutes), but have high sensitivity, specificity • Have multiple test forms so it can be repeated often • Detect change over time (monthly, weekly, daily, hourly testing) (infinite number of comparable forms with high test-retest consistency)
Audience Screening using a Continuous Recognition Test (CRT) • CRT is widely used academically for memory study • Presentation of complex pictures (that are easily remembered normally) are useful for detecting memory difficulties • Testing memory using a pictures approach can be standardized for population use • Picture memory is less affected by education • Picture memory can be tested by computer • Audiences can be shown slide presentations
d' The relationship between discriminability (d′) and age on the audience-based continuous recognition test of memory for 868 individuals with all information Age (years)
The relationship between discriminability performance (d′) and age in 868 individuals on the continuous recognition test of memory
The relationship between discriminability performance (d′) and age in 868 individuals on the continuous recognition test of memory.
Mem. Trax - Memory Test (on-line version) • • • Test to screen for memory function and change Available on any platform Determines percent correct and recognition time Measures episodic memory, inhibition Test takes 1 to 2 minutes Test can be repeated often (even hourly) High test-retest consistency Minimal learning over repeated tests Change over time sensitively detected
Mem. Trax Test Development • Based on the continuous recognition task paradigm Categories Mountain Fountain Art House Birdhouse 1 3 s 3 s Pic 1_CArt 1_Repeat 0 Pic 2_CMountain 1_Repeat Pic 3_C 0 Fountain 1_Repeat Pic 4_C 0 Art 1_Repeat 1 Pic 5_CHouse 1_Repeat 0 Pic 6_C 3 s 3 Ts ota 3 s ~3 l t mi ime ns 2 3 4 5 Birdhouse 1_Repea t 0 . . 3 s Pic 26_CArt 1_Repeat 2 Pic 27_CMountain 1_Repeat 2 Pic 49_CMountain 5_Repeat 1 Pic 50_CArt 5_Repeat 1 . . 3 s
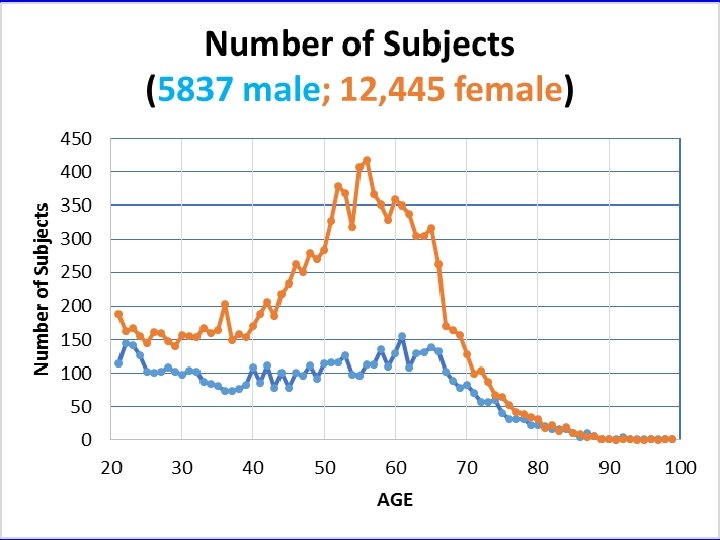
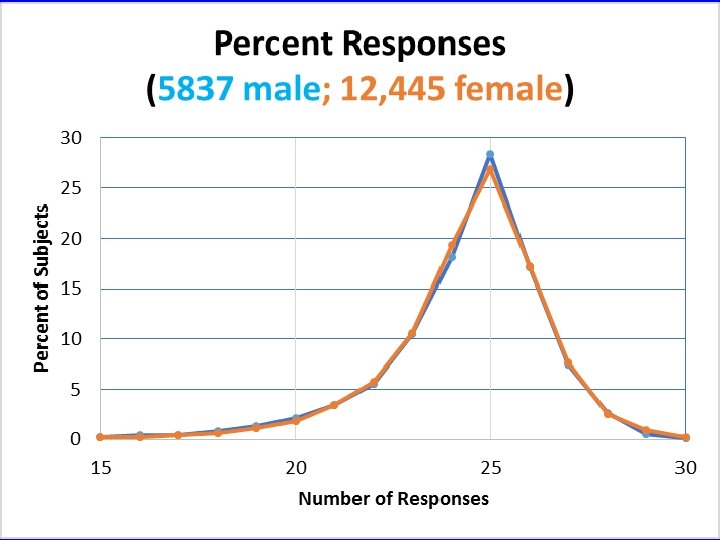
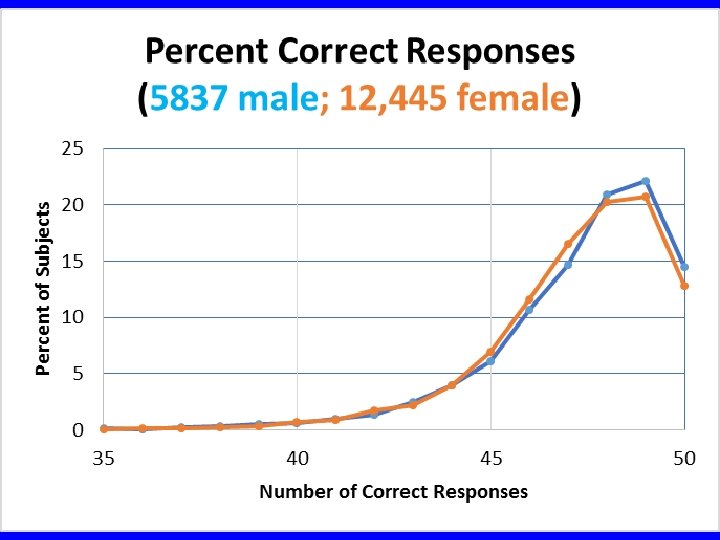
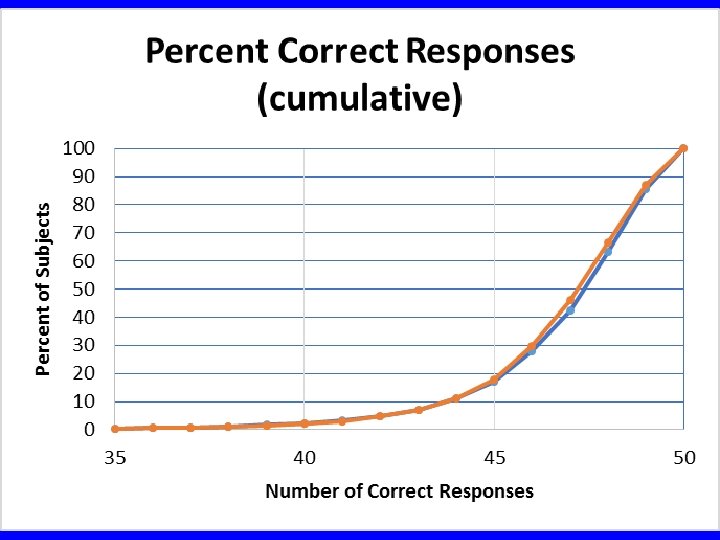
Mem. Trax Test Data • Data collection period: September 2011 - August 2013 • Collected in collaboration with HAPPYneuron, Inc. (Lyon, France) • 4, 800 repeat administratons (over 24 months, up to 24 times) • Analysis approved by Stanford IRB • Total number of tests taken: 30, 435 • Tests excluded: 12, 153 – Repeat administrations: 4, 800 (over 24 months, up to 24 times) – Age below 21: 4, 999 (no IRB approval for under 21 analyses) – Age above 100: 1, 573 (unrealistic number) – Performance outliers: 780 (invalid scores - less than 70% correct • Total valid, initial tests: 18, 282 – Females: 12, 445 – Males: 5, 837 • Mean age: 50. 28 years, SD: 15. 23, Range 21 -99 years
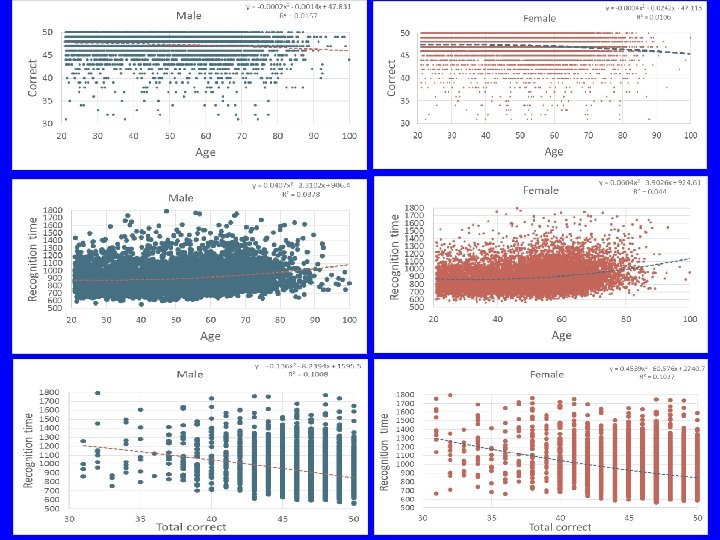
Data Analysis (25 initial presentations, 25 repeats) (males, females separated) - Number of subjects by age Total number responses (similar to beta) Number of correct responses (similar to d’) Cumulative number of correct responses Percent correct versus age Recognition time versus percent correct Number wrong and +2 STDs versus age Recognition time and +2 STDs versus age
Number Wrong, m vs f, mean + 2 SD 16 15 14 R 2 = 0. 4372 R 2 = 0. 6824 13 Number wrong out of 50 12 11 R 2 = 0. 4285 R 2 = 0. 6321 10 9 8 7 6 5 4 3 2 1 0 20 30 40 50 60 AGE (years) 70 80 90
Recognition Time, m vs f, mean + 2 SD 1600 Recognition Time (msecs) 1500 R 2 = 0. 925 1400 1300 R 2 = 0. 8199 1200 1100 1000 900 800 20 30 40 50 60 AGE (years) 70 80 90
Positives versus Negatives www. memtrax. com • • • Very Fast (less than 2 minutes) Easy (explanation can be understood) Innovative (based on extensive memory studies) Tests complex encoding (unlike any other available test) Fun (subjects very willing to retake tests frequently) Reliable (test works on many platforms) Inexpensive (after development, cost is negligible) Infinite number of repeatable tests (test-retest reliability) Validity - face, construct (measures memory encoding) Normative data (collected in large quantities) • • • Does not test remote memory (but does have cultural sensitivity) Human monitoring optional (can be taken without supervision) Requires access to internet enabled device (at present) Computers cannot yet make diagnosis (may assist) Discriminant/concurrent validity lacking (need to establish) Distraction could influence test results
Needs for Better Memory Testing Clinicians/Professionals/Researchers • Testing & Monitoring – Individuals – Family members – Friends – Care givers • Researchers – Pre-post intervention trials – Cognitive studies – Adaptable for f. MRI studies
Future Directions for Testing • Precise assessment of cognition from normal to moderate dementia • Item Response Theory and Computerized Adaptive Testing (on-line update of analyses) • Expansion to measure numerous functions • Analysis of tests for risk/benefit (cost-worthiness) • Expansion of applications – driving, various types of cognitive impairment, hospital monitoring • Use for recruitment of subjects for AD research – Mem. Trax being used by www. brainhealthregistry. org
New Applications for Memory Testing • Medicare Annual Wellness Visit cognitive assessment • 6 th vital sign for health-provider visits • Pharmacist assures client is able to understand directions for prescribed medication • Evaluate potential for learning in subject beginning rehabilitation therapy (stroke, etc. ) • Assessment of anesthesia recovery • Contact sport side-line assessment of concussion • Determine if individual is safe to operate heavy machinery, drive