Megaloblastic vs Nonmegaloblastic Macrocytosis MCV100 fl Type Pathogenesis
 Type Pathogenesis Classification Megaloblastic Defective DNA B 12")
Megaloblastic vs Nonmegaloblastic Macrocytosis (MCV>100 fl) Type Pathogenesis Classification Megaloblastic Defective DNA B 12 deficiency synthesis; Folate deficiency Abnormal RBC maturation; Others Granulocytic/ megakaryocytic maturation are also affected Nonmegaloblastic NS Alcoholism, liver disease, hemolysis, posthemorrhagic, hypothyroidism, cold agglutinin disease, severe hyperglycemia

Megaloblastic Anemia Megalobalstic anemias Cobalamin deficiency Folate deficiency Drugs Miscellaneous Decreased ingestion Impaired Absorption Impaired utilization Decreased Ingestion Impaired Utilization Increased requirement Increased loss Metabolic inhibitor Inborn error Unexplained Disorders

Folic Acid: Absorption l 음식 l l l Asparagus, broccoli, spinach, lettuce, green bean 가열 파괴 흡수 l 공장의 근위부가 주된 흡수장소

Folic Acid: Function

Folic Acid: Function l Transfer one-carbon units l l N 5, N 10 methylene. THF l l Methylene Formyl groups THF acts as a carrier of reactive single carbon units, which are bonded to N-5 and N-10. Related to the synthesis of DNA, RNA, and proteins.

Folic Acid Pathway

Etiology of Folate Deficiency l Inadequate intake l l Increased requirement l l HA, dialysis Malabsorption l l Alcoholics, narcotic addicts, elderly Non-tropical sprue Drugs l Methotrexate, pentamidine, trimethoprim, pyrimethamine, triamterene
 l l Methotrexate (DR Inhibitor) 5 -fluorouracil (TS Inhibitor)")
Drugs (Folic acid inhibitor) l l Methotrexate (DR Inhibitor) 5 -fluorouracil (TS Inhibitor)
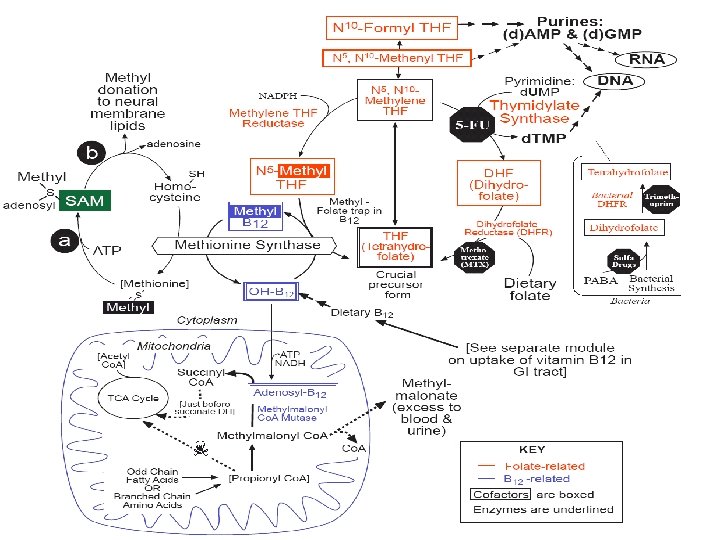

Vitamin B 12: Function l l Vitamin B 12 acts as a coenzyme for 13 enzymes Coenzyme for methylmalonyl Co. A mutase l l l Proprionate metabolism Neural tissue maintenance Coenzyme in the conversion of homocysteine to methionine l l l Vitamin B 12 is necessary for the methyl group transfer from methyl folate to homocysteine producing methionine Without vitamin B 12, methyl folate is trapped This causes a secondary deficiency in folate resulting in megaloblastic anemia
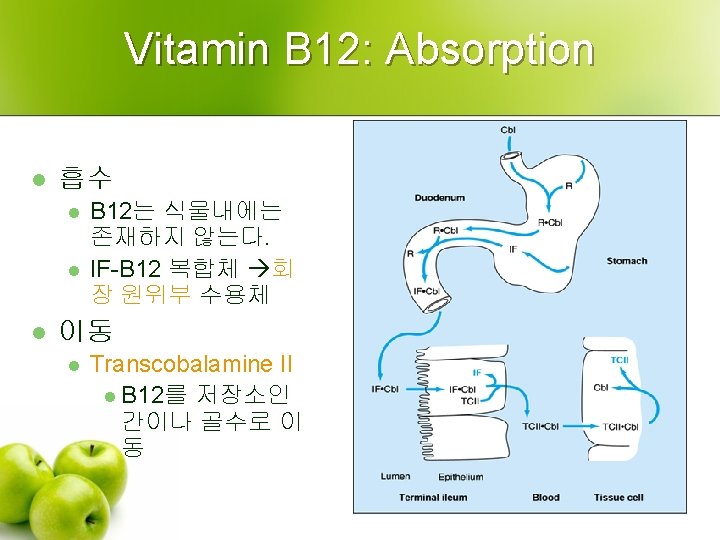

Etiology of Vitamin B 12 Deficiency

Folate Trap Hypothesis l l l In cobalamin deficiency Trapping of intracellular folate as 5 methyl. THF Intracellular deficiency of all forms of folate except 5 methyl. THF

Folate Trap Hypothesis l l l Cobalamin deficiency and folate deficiency produce indistinguishable hematologic abnormalities The hematologic abnormalities seen in cobalamin deficiency can be completely reversed by pharmacologic amounts of folic acid. The hematologic abnormalities caused by folate deficiency respond only slightly, if at all to large amounts of cobalamin.

Clinical Manifestations of Vitamin B 12 Deficiency

Hematologic Manifestation: PB l l l Reticulocyte count is not elevated MCV is often increased Neutropenia and thrombocytopenia Neutrophil hypersegmentation Nucleated red cells Hemolytic anemia

Hematologic Manifestation: BM l l Hypercellular in all cellular elements. Megaloblastic changes l l In all cells within the bone marrow More prominent in the erythroid series

Hematologic Manifestation: BM

Ineffective Erythropoiesis
")
Neurologic Manifestation (B 12 deficiency)
 l Loss of myelin with axonal degeneration Most frequently")
Neurologic Manifestation (B 12 deficiency) l Loss of myelin with axonal degeneration Most frequently in the dorsal and lateral columns l Peripheral and cranial nerves l l Spinal cord Initially: dorsal (proprioceptive afferent) l Later: lateral (corticospinal efferent) l
 l l This leads to a spongy or")
Subacute Combined Degeneration (B 12 deficiency) l l This leads to a spongy or "vacuolar" degeneration of the spinal cord white matter that begins in the posterior and lateral columns. Subacute combined degeneration is due to vitamin B-12 deficiency.

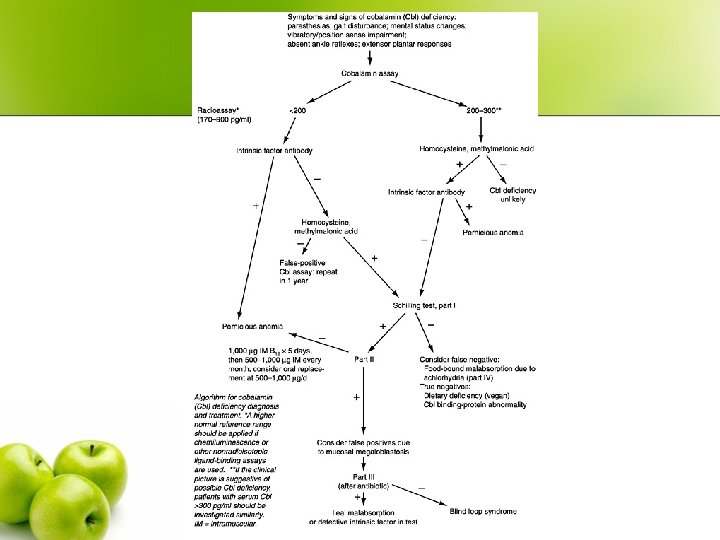
Diagnosis of Megaloblastic Anemia l Blood concentration l S-Folate/Vitamin B 12 l Initial screening tests l S-Methylmalonic acid/Homocysteine l Follow-up tests Schilling test l Therapeutic trial l

Typical Serum Findings in Megaloblastic Anemias Component Normal Levels Deficiency Cobalamin Folate Cobalamin 200 -900 pg/m. L D N Folate 2. 5 -20 ng/m. L N D MMA 70 -270 nmol I N Homocysteine 5 -14 umol I I

Pernicious Anemia l l l 주로 중년이후 북유럽에 빈발 검사 l l Chronic atrophic gastritis Anti-intrinsic factor antibody: 특이도 Anti-parietal cell antibody 임상양상 l B 12 결핍 증상 l 연관 l l l Hashimoto's thyroiditis Hypogammaglobulinemia Rheumatoid arthritis Vitiligo 예후 l 2/3: increased risk of gastric ca.

Treatment of MA l B 12 deficiency Parenteral cobalamin. l Oral cobalamin l l Folate deficiency l l Oral folate Red cell transfusions

Vitamin B 12 Deficiency: Tx l l The traditional approach to treating cobalamin is intramuscular injection of cyanocobalamin. Alternatives include oral tablets and nasal gel. l l l Patients with pernicious anemia will absorb 1 to 2 percent of an oral dose even without IF. One thousand to two thousand micrograms daily of oral B 12 is an alternative to injections. The nasal gel is currently labeled for maintenance use.

Folate Deficiency: Tx l l l Folic acid 1 mg daily will replenish body stores in about three weeks. Patients with malabsorption may require doses up to 5 mg/day for replenishment. Because folic acid, even through food supplementation, partially corrects the hematologic abnormalities of B 12 deficiency but not the associated neurologic deterioration, concomitant B 12 deficiency should be ruled out before starting folic acid therapy.
- Slides: 30