MEGACOLON VIKAS K M 2002 MBBS MEGACOLON DEFINITION

MEGACOLON VIKAS. K. M 2002 MBBS

MEGACOLON • DEFINITION Distention of the colon to greater than 6 or 7 cm in diameter MEGACOLON CONGENITAL ACQUIRED

HIRSCHSPRUNG’S DISEASE
 n Neurogenic form of intestinal obstruction in")
CONGENITAL HIRSCHSPRUNG’S DISEASE Harald Hirschsprung (1830 -1916) n Neurogenic form of intestinal obstruction in which there is an absence of ganglion cells in the myenteric & submucosal plexus n 1 in 4500 n Sex ratio 4: 1

HIRSCHSPRUNG’S DISEASE GENETICS n Hetrogeneous n Mutations RET gene & RET ligands Endothelin receptor system n 3 -5% have down’s syndrome

HIRSCHSPRUNG’S DISEASE n Hydrocephalus VSD Meckel’s diverticulum n Definite family history

PATHOLOGY FAILURE OF MIGRATION of neuroblasts into the gut from vagal nerve trunks n ABSENCE of ganglion cells in neural plexus n HYPERTROPHY of nerve trunks n

MACROSCOPICALLY The affected segment is NOT DISTENDED n Properly innervated upstream segment DILATES n Wall may be thinned or thickened n Stercoral ulcers n

HIRSCHSPRUNG’S DISEASE

HIRSCHSPRUNG’S DISEASE Dilation of bowel proximal to the affected region

HIRSCHSPRUNG’S DISEASE
 is in the small intestine")
TOTAL COLONIC HIRSCHSPRUNG’S DISEASE The transition zone (arrow) is in the small intestine

STERCORAL ULCERS

MICROSCOPICALLY ABSENCE OF GANGLION CELLS
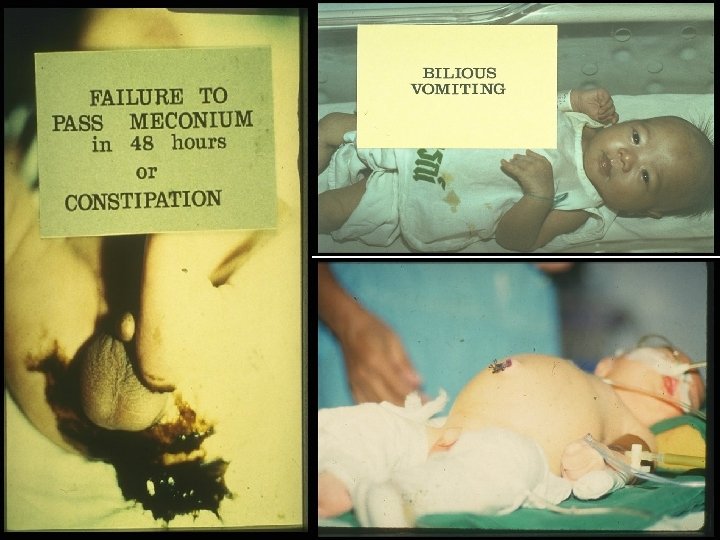
 n Abdominal distension n Bilious vomiting n Severe")
CLINICAL FEATURES Delayed passage of meconium(95%) n Abdominal distension n Bilious vomiting n Severe diarrhoea altrenating with constipation(10 -15%) Enterocolitis of hirchsprung’s disease n

DIAGNOSIS

DIAGNOSIS ABDOMINAL RADIOGRAPH Dilated bowel loops with fluid levels n Intramural gas – enterocolitis n Free peritonial gas - perforation n

ABDOMINAL RADIOGRAPH Dilated bowel loops Fluid levels

DIAGNOSIS BARIUM ENEMA n Indicate length & site n No definitive cutoff point indicating transition zone n Evacuation of contrast may take 24 – 48 hours n Transition zone clear on delayed x-ray

BARIUM ENEMA Coning down of transition zone n Irregularity in the mucosa n Abnormal contractions n TZ
, dilatation of normal bowel segment (red arrow)")
BARIUM ENEMA Contracted diseased segment (black arrow), dilatation of normal bowel segment (red arrow) and the transitional zone (TZ)

BARIUM ENEMA TZ

DIAGNOSIS RECTAL BIOPSY n Submucosal suction biopsy is adequate in 90% n Full thickness operative biopsy in more emergent circumstances n Absence of ganglion cells in at least 10 sections – diagnosis confirmed n Increased Ach staining of neurofibrils

RECTAL BIOPSY

Ach STAINING NORMAL INSCREASED Ach STAINING

DIAGNOSIS ANORECTAL MANOMETRY n Measures anorectal intraluminal pressure n Absent rectoanal inhibitory reflex indicating a lack of relaxation of the internal sphincter characteristic of aganglionosis

ANORECTAL MANOMETRY

DIFFRENTIAL DIAGNOSIS HYPOTHYROIDISM n MECONIUM PLUG SYNDROME n COLONIC NEURONAL DYSPLASIA n ADYNAMIC ILEUS WITH SEPSIS n INTESTINAL PSEUDO-OBSTRUCTION n

TREATMENT

TREATMENT n Depends on Age Length of involved segment Severity of symptoms Presence of enterocolitis

TREATMENT NEONATAL PERIOD n TEMPORARY DECOMPRESSING COLOSTOMY n At least 10 cm proximal to transition zone

COLOSTOMY
 n")
TREATMENT 6 MONTH – ONE YEAR A definitive pull-through procedure using n SOAVE(endorectal) n DUHAMEL(retrorectal) n SWENSON(rectosigmoidectomy)

PULL-THROUGH PROCEDURE n Each is done a little differently, but all involve removing the part of the intestine that isn't working and connecting the healthy part that's left to the anus. After pull-through surgery, the child has a working intestine

SOAVE PROCEDURE

DUHAMEL PROCEDURE

SWENSON PROCEDURE

OPERATIVE FINDING OF TRANSITION ZONE

PROGNOSIS Overall survival in > 90% cases n Rare deaths due to – Delayed diagnosis Complications n > 96% continent n Long term follow up is important n

ACQUIRED MEGACOLON

ACQUIRED MEGACOLON CAUSES n Chagas disease n Organic obstruction of bowel n Toxic megacolon n Fuctional psychosomatic disorder

ACQUIRED MEGACOLON n Can occour at any age n Except for chagas disease, where inflammatory involvment of ganglia is evident, the remaining forms are not associated with deficiency of mural ganglia

CHAGAS DISEASE Protozoosis n Flagellate protozoa Trypanosoma cruzi n Destruction of the autonomic nervous system innervation of the colon leads to a loss of the normal smooth muscle tone of the wall and subsequent gradual dilation n REDUVID BUG

MEGACOLON IN CHAGAS DISEASE

TOXIC MEGACOLON DEFINITION Toxic megacolon is the clinical term for an acute toxic colitis with dilatation of the colon n Total or segmental n Hallmarks - nonobstructive colonic dilatation larger than 6 cm and signs of systemic toxicity n

TOXIC MEGACOLON

TOXIC MEGACOLON Colon is dilated and shows hemorrhagic necrosis

TOXIC MEGACOLON CLASSIC ETIOLOGIES Ulcerative colitis n Crohn colitis n Pseudomembranous colitis n Crohns disease Pseudomembranous colitis

TOXIC MEGACOLON INFECTIOUS CAUSES n Salmonella species n Shigella species n Campylobacter species n Yersinia species n Clostridium difficile n Entamoeba histolytica n Cytomegalovirus OTHER CAUSES n Radiation colitis n Ischemic colitis n Nonspecific colitis secondary to chemotherapy

PATHOPHYSIOLOGY The microscopic hallmark inflammation extending beyond the mucosa into the smooth-muscle layers and serosa n NO involved in the pathogenesis n NO inhibits smooth-muscle tone n NO generated by inflammatory cells n

CLINICAL FEATURES Abdominal pain n Severe diarrhoea n Abdominal distention n Generalised tenderness n Fever, leucocytosis, tachycardia pallor & lethargy n

DIAGNOSTIC CRITERIA - Jalan et al Radiographic evidence colonic dilatation n Three of the following - Fever (>101. 5°F), tachycardia (>120), leukocytosis (>10. 5), or anemia n One of the following - Dehydration, altered mental status, electrolyte abnormality, or hypotension n

INVESTIGATIONS

LAB STUDIES Blood examination leukocytosis with a left shift bloody diarrhea results in anemia n Electrolyte disturbances n ESR & CRP usually are elevated n
 transverse colon n Loss of colonic haustrations")
IMAGING STUDIES ABDOMINAL RADIOGRAPH Dilated (>6 cm) transverse colon n Loss of colonic haustrations n pseudopolyps n Free intraperitoneal air n

ABDOMINAL RADIOGRAPH

IMAGING STUDIES CT – SCAN n Perforation n Abscess BARIUM ENEMA n Avoid barium studies n perforation

ENDOSCOPY Diagnosis is in doubt & patient is not toxic n Flexible sigmoidoscopy or colonoscopy n Perforation is an obvious potential complication with this approach n

ENDOSCOPY n n The mucosa is grossly denuded, with active bleeding noted Patient had her colon resected very shortly after this view was obtained

MEDICAL MANAGEMENT TREATMENT

MEDICAL TREATMENT 3 main goals n Reduce colonic distension to prevent perforation n Correct fluid and electrolyte disturbances n Treat toxemia and precipitating factors

MEDICAL TREATMENT IV fluids n Electrolyte resuscitation n Nasogastric suction n Broad spectrum antibiotics n Total parenteral nutrition n Intravenous steroids No response in 24 -48 hrs - surgery n

SURGICAL MANAGEMENT

SURGICAL MANAGEMENT n Early surgical consultation is essential INDICATIONS- For urgent intervention n Free perforation n Massive hemorrhage n Increasing toxicity n Progression of colonic dilatation

SURGICAL MANAGEMENT Acute toxic megacolon – high operative morbidity & mortality n Conservative approach is appropriate n Anal sphincter sparing procedurespossibility of subsequent surgical correction for continence n

SURGICAL MANAGEMENT WHEN URGENT COLECTOMY REQUIRED TOTAL ABDOMINAL COLECTOMY n BROOKE ILEOSTOMY n HARTMANN’S POUCH n

TOTAL ABDOMINAL COLECTOMY

BROOKE ILEOSTOMY

HARTMANN’S POUCH This surgery leaves you with only one stoma and the non-functional end of the bowel simply stitched or stapled shut and left inside you until reconnection can take place.

SUMMARY HIRSCHSPRUNG’S DISEASE • Hirschsprung’s disease is a defined clinical entity with an unclear etiology • Early diagnosis, surgical expertise & multidiciplinary support • Current trends are towards any of the pull-through procedures

SUMMARY TOXIC MEGACOLON • Nonobstructive colonic dilatation larger than 6 cm and signs of systemic toxicity • Combined aggressive medical & surgical treatment • Total abdominal colectomy, Brooke ileostomy & Hartmann’s pouch

n a Th . . . u o y k
- Slides: 73