Meditech 6 0 Upgrade ED TRAINING SESSION 1

 Reception Routine")


")


 Questions")


























- Slides: 38
Meditech 6. 0 Upgrade ED TRAINING SESSION 1
Agenda • • My Steward Review Tracker Orientation (Main, RN, Charge RN) Reception Routine Triage and Allergies ED Visit Data RN Documentation and Screen Layout RN Additional Focus of Care RN Edit and Undo
My Steward • Locating Training Materials • Training Process – Intro – CBT – Questions
Meditech Training Tutorials
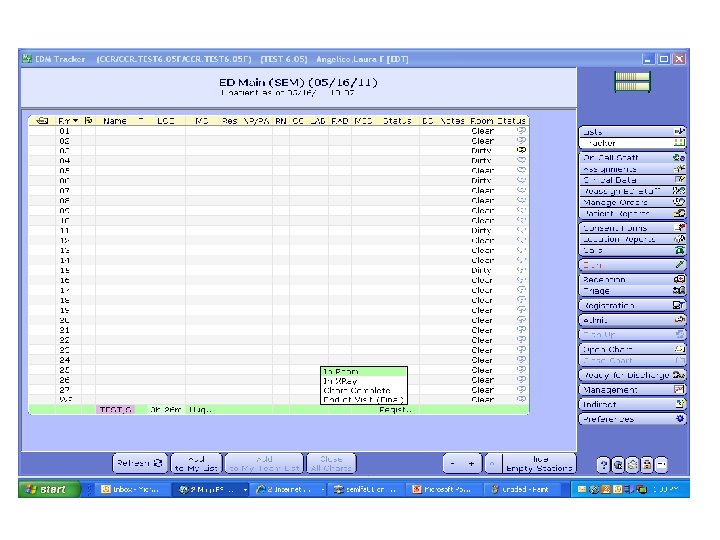
Tracker Orientation – EDM Tracker • Location Tracker (Main ED, Fast Track, etc. ) – These tracker are meant to be Standard Across the system. • My RN Tracker – This tracker allows you to keep track of only patients you are caring for. It also shows more detailed information. • Charge RN Tracker – This tracker will display all area’s of the ED and show more detail on the patient.
Tracker and Personalized View Tutorial
Charge Nurse Tracker • All RN’s will have access to the Charge Nurse Tracker • The Charge Nurse tracker contains detailed information on the patient • Displays all patient in all area’s Main, FT
Tracker and Personalized view (My RN) Questions
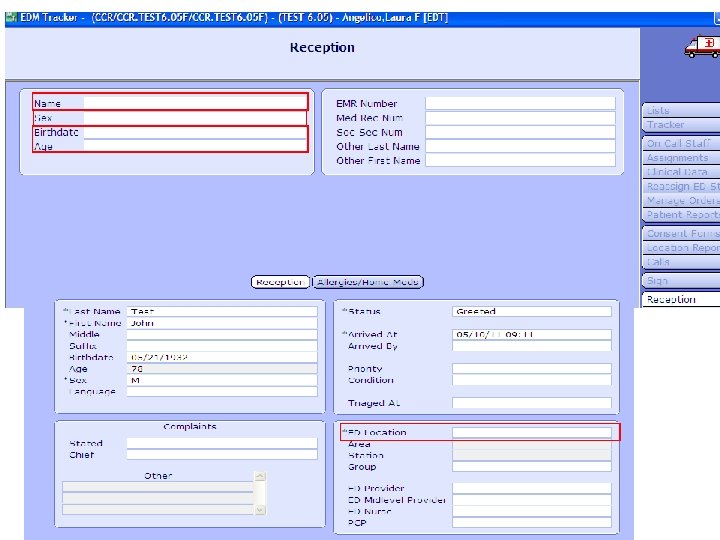
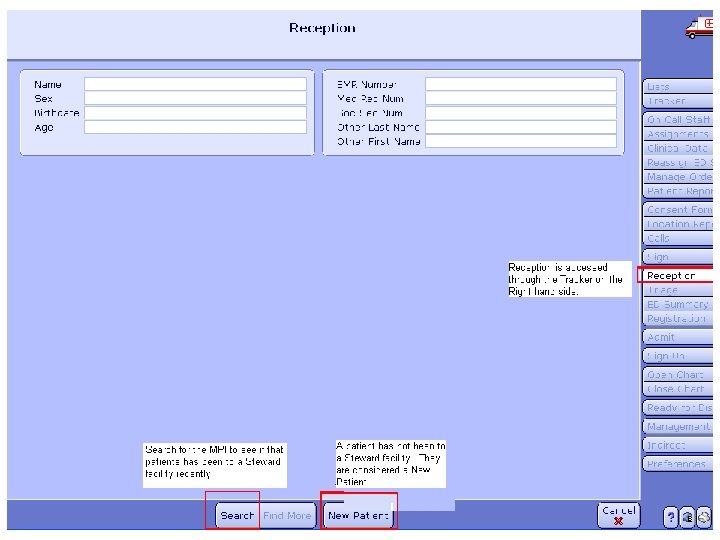
Reception Routine • This routine is the quickest way to get the patient on the tracker. – It consists of only 4 required questions. – Patient Name is a required field and should be entered in mixed case (ex. Darling, Jean) • Routine is meant to be used by Nursing only if Patient Access/Registration is not available to put the patient on the tracker. – Primarily this is a patient access/registration routine. – Through this routine you are able to print the patient wrist band face sheet. – When RN’s must perform this routine they should enter the SS number whenever possible and click SEARCH for the MPI (master patient index).
Triage and Allergies • Triage can be accessed through the tracker
Triage and Allergies • This routine allows you to document the Triage assessment as well as: – – – • Change the Location of the patient Change the Room for the patient Enter in the Patient’s Chief Complaint There are certain functions that even though you have access should not be updated on this screen – Filling in the Providers of Care will update the statistics such as door to doctor time. This is being updated another way and should not be updated on this screen. The only fields that should be filled in on the screen in the first tab of the screen are: Location, Room, Chief Complaint and Triage (Patient’s MOA must be entered) along with the ESI level.
Allergies • Allergies is accessed on the second tab of Triage • Allergy information crosses to PCS, OM etc. – Allergies must be entered to place orders in OM • Allergy information is recalled on the medical record based on what was entered in the patients last visit.
Triage and Allergies Tutorial
Triage and Allergies Questions
ED Visit Data Screen • The ED Visit Data Screen is an additional screen where you can update the patients room and location. • To access the screen go to Open Chart -> ED Visit Data
Documenting in Meditech • Ensure that you are logged onto the computer under your own name and have a pin • All entries are part of the patients legal Medical Record and time stamped • Only answered questions appear as part of the Medical Record • Be sure to lock down or sign out of your PC when leaving • All documentation must be completed prior to Discharge or Admit and before end of shift. • Always remember to SAVE your documentation!
Things that MUST be Documented in Meditech on every patient • • • Complete Triage Assessment Allergies Patient History CC Assessment RN Disposition Documentation (part of Discharge Routine)
Things that need to be documented in Meditech as applicable • Additional Focus of Care items • Additional Vital Signs and Progress Notes • IV site Intake and Output/ Add an IV or Add a Void • Critical Value • Treatments • Other
Chief Complaints • By choosing a Chief Complaint at Triage you are driving documentation onto your work list.
Notes • You have the ability to add a Progress Note in the Vital Signs and Progress Note Assessment (typically this is what is being utilized for notes) • You also have the ability to document anything in the comment section in each one of the CC driven assessments.
RN Documentation and Screen Layout
RN Documentation and Screen Layout Questions
Additional Focus of Care • Allows you to add assessments as needed
RN Additional Focus of Care
RN Additional Focus of Care Questions
Oops! • With edit and undo options you have the ability to edit incorrect documentation done on a patient. • You also have the ability to remove the entire assessment • If you need to back date the time that can be done as well either when initially documenting or at a later time through edit
RN Edit and Undo
RN Edit and Undo Questions
Printing A Patient Report • Click the ED Summary button from the Tracker • Print the ED Summary this contains the complete SBAR format information of the patients visit.
Things that are still on paper • • • Codes Procedural Sedation State Mandated Forms Cobra Section 12 Consents
EMR Review – Highlight the Patient and Open the Chart EMR – Click on Clinical Panel – Choose the ED Here you can review all ED documentation (this is utilized by ED Physicians, medical records and inpatient Nurses)
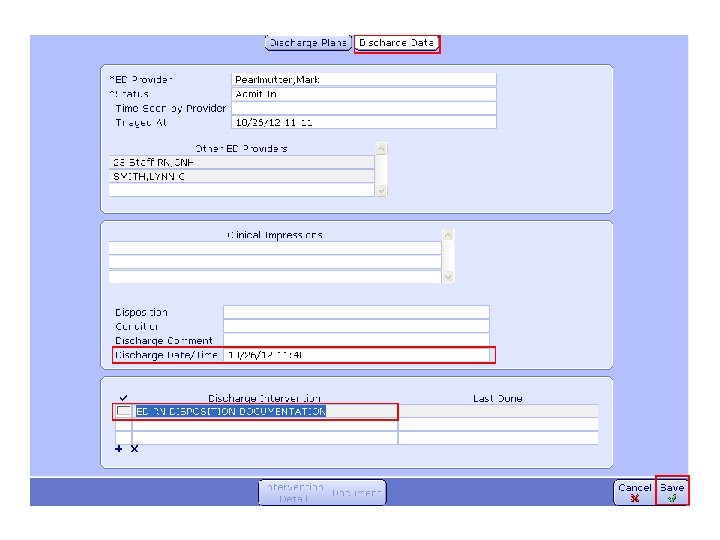
Discharge • Accessed through Open Chart • The discharge date/time should be entered for when the patient is leaving the department this function is done by the CAN staff • The discharge intervention should also be filled in a the time of discharge • Once both are complete and accurate the Discharge can be saved.
Remove the Patient off the Tracker: Status Event change • To remove a patient from the tracker you must update the status event to End of Visit • This must be done after the patient has left the ED.
Questions? Time to practice! Remember the more practice you have now the better off you will be!