MEDICATIONS FOR TREATMENT OF OPIOID USE DISORDER WHY




 • Chronic, relapsing disorder characterized by • compulsive drug seeking")
? • An")


 • • • Severe nausea/ vomiting Diarrhea")



 • Methadone")






 • Long-acting opioid antagonist (blocker) • Best option for those leaving")







- Slides: 35
MEDICATIONS FOR TREATMENT OF OPIOID USE DISORDER: WHY USE THEM AND HOW DO THEY WORK? ANGELINE STANISLAUS, MD CHIEF MEDICAL DIRECTOR- ADULT SERVICES MISSOURI DEPT OF MENTAL HEALTH
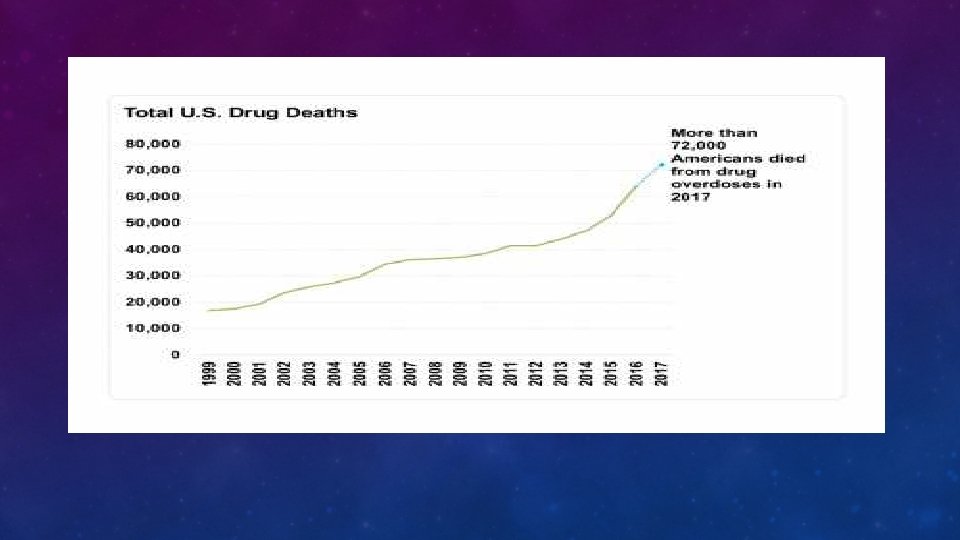
HOW MANY PEOPLE ARE DYING EACH DAY? 115
• Overdoses
MISSOURI- TOTAL NUMBER OF OPIOID RELATED DEATH 2017 951 • 92% Accidental overdose • 7% Suicide
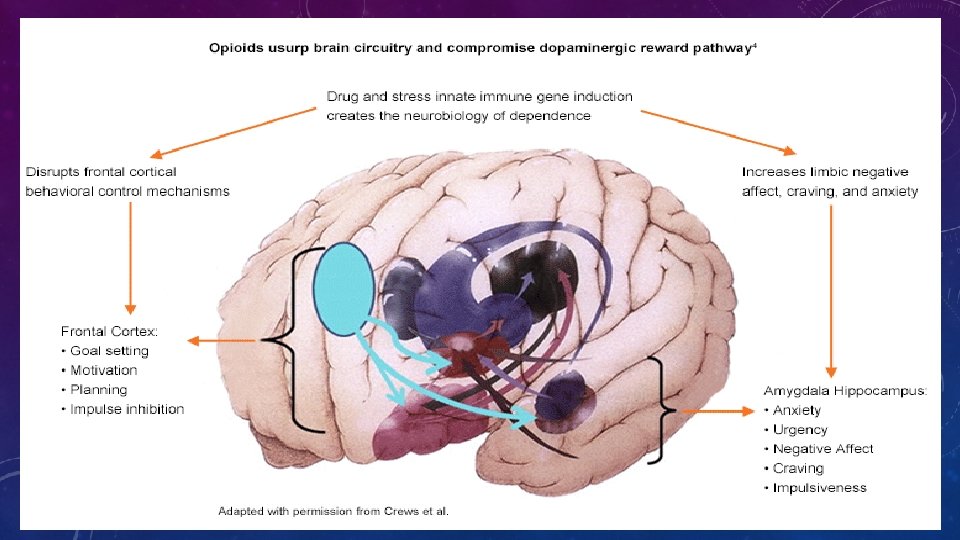
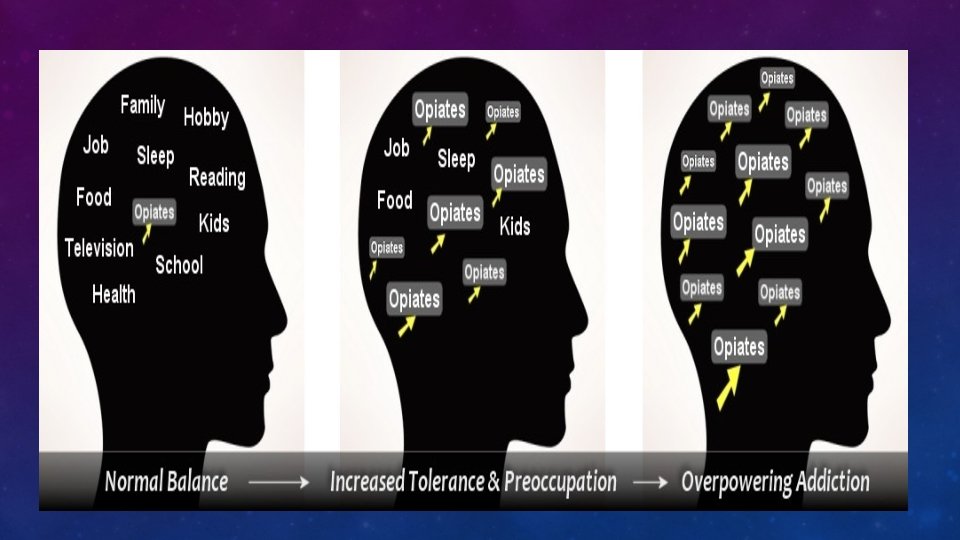
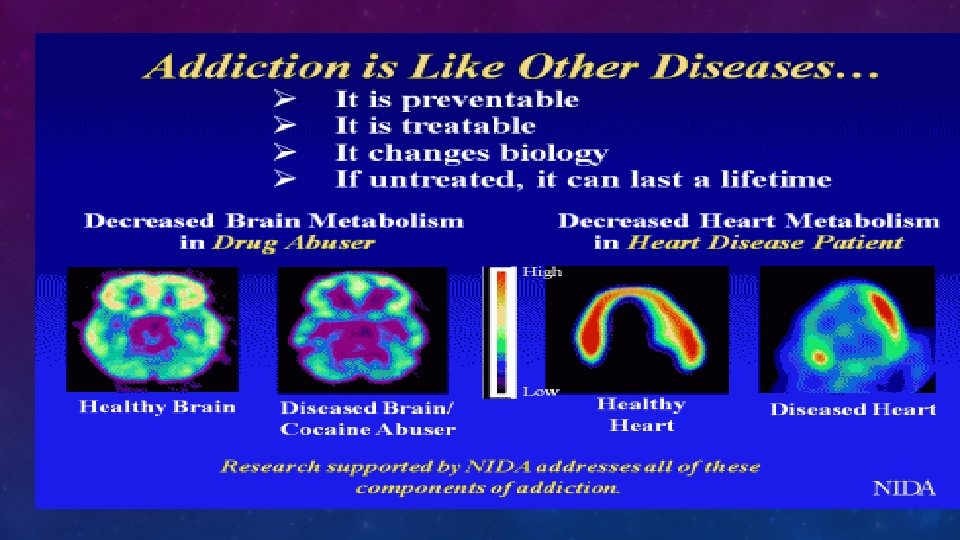
DEFINITION OF ADDICTION (NIDA) • Chronic, relapsing disorder characterized by • compulsive drug seeking and use • despite adverse consequences. • It is considered a brain disorder because • it involves functional changes to brain circuits involved in reward, stress, and self-control • those changes may last a long time after a person has stopped taking drugs.
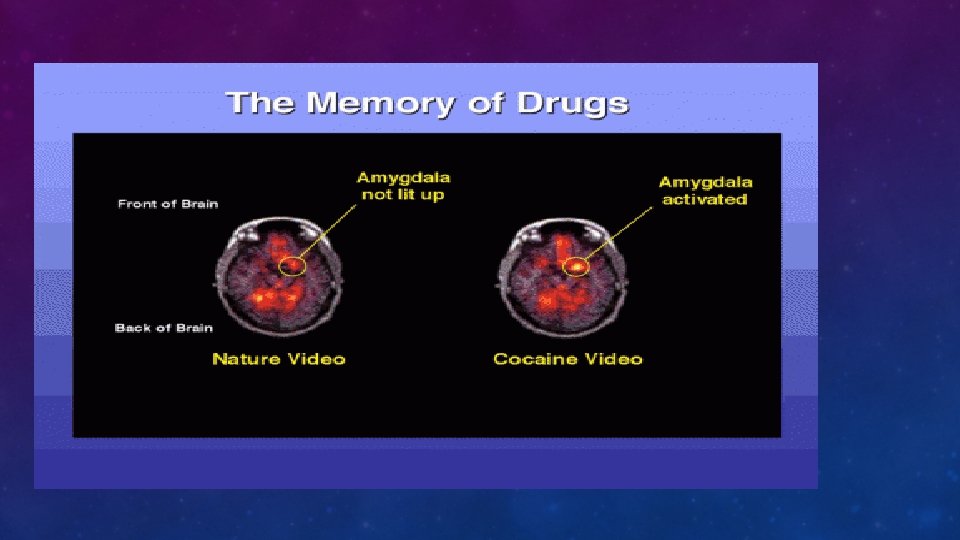
WHEN DOES USE OF A SUBSTANCE BECOME A SUBSTANCE USE DISORDER (SUD)? • An underlying change in brain circuits that may persist beyond detoxification • Behavioral effects of these brain changes include intense drug craving when the person is exposed to drug-related stimuli • Results in repeated relapses
INTERACTIONS OF GENETIC FACTORS AND ENVIRONMENT
HALLMARK OF OPIOID USE DISORDER • Tolerance • Withdrawal • Craving
WITHDRAWAL SYMPTOMS • Opioid withdrawal (Dope sick) • • • Severe nausea/ vomiting Diarrhea Muscle aches Fever Lacrimation (tearing) Pilo-erection (goosebumps) Pupils dilated Yawning Insomnia
MANAGEMENT OF CRAVING
OPIOID USE DISORDER • Buprenorphine / Suboxone • Naltrexone XR-NRT (Vivitrol) • Methadone
PHASES OF TREATMENT FOR OUD • Induction • Stabilization • Maintenance
SUBOXONE
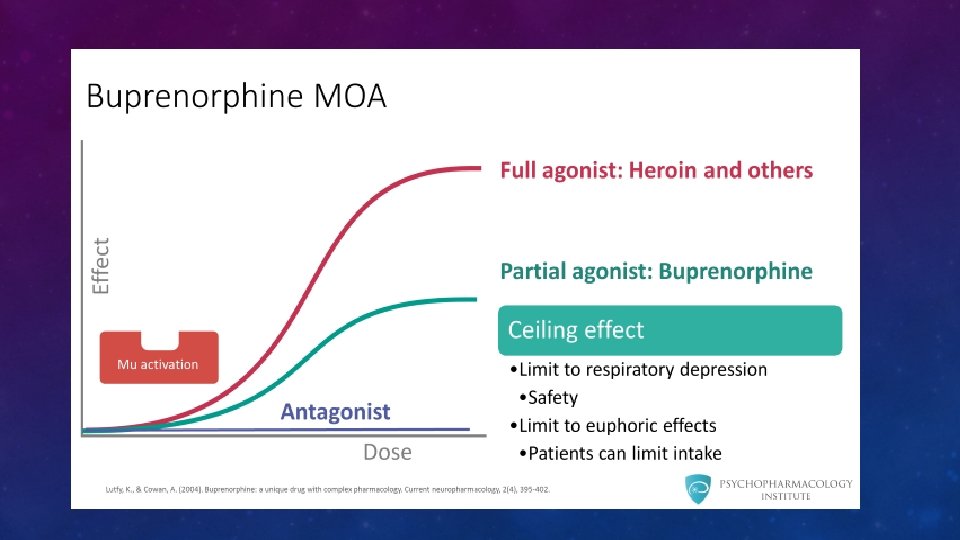
BUPRENORPHINE
SUBOXONE • Not absorbed when taken orally • 50% absorption when taken sublingually • Plasma concentration peaks in 1 hour • Long half-life – up to 32 hours • Metabolized by P 450 3 A 4
SUBOXONE • Can be given as single dose • More effective as divided doses to manage craving • Very slow to dissociate from opioid receptors -24 to 60 hours
METHADONE • Full agonist • Very long half-life- 2 days • Available only in specialized OTP • Daily administration for several months.
NALTREXONE XR-NRT (VIVITROL) • Long-acting opioid antagonist (blocker) • Best option for those leaving jails and prisons after period of abstinence
HOW LONG SHOULD THEY TAKE MEDICATIONS AND REMAIN IN TREATMENT?
MEDICATION FIRST MODEL OF TREATMENT FOR OUD • Managing fear of withdrawal • Stabilizes the brain circuits • Better engagement in treatment • Decreased deaths from opioid overdose • Then able to engage better in needed psychosocial treatments
MEDICATION FIRST MODEL DOES NOT MEAN “MEDICATION ONLY” MODEL LOWERS THRESHOLD FOR MEDICATION TREATMENT MEET THE CLIENT WHERE THEY ARE!
RECOVERY • The road to recovery is long and windy with several pot holes • Relapses occur despite the best treatment like all chronic illnesses • As long as they are alive, they can work on it again • Kicking them out of the program for minor violations is not helpful • We expect patients to meet us where we are. • If they could, they would have done it! • We need to meet them where they are and help them work their way up.
NALOXONE
HIGH RISK FOR OPIOID OVERDOSE • Individuals who have overdosed once are at higher risk of overdosing again • After a period of abstinence and re-use (less than 5 days of stopping use tolerance decreases) • Release from jails, prisons, residential facilities • IV users are at higher risk • Household members of those prescribed opioid pills
HIGH RISK FOR OPIOID OVERDOSE • Opioids taken in combination with other sedating substances such alcohol, benzodiazepines • Those who also have medical conditions such as liver and lung disease • Co-morbid psychiatric conditions such as depression, PTSD – increase risk of suicide