Medication use in residential aged care facilities The


























- Slides: 29
Medication use in residential aged care facilities
The patients
Who are our patients? AIHW 2012
uk
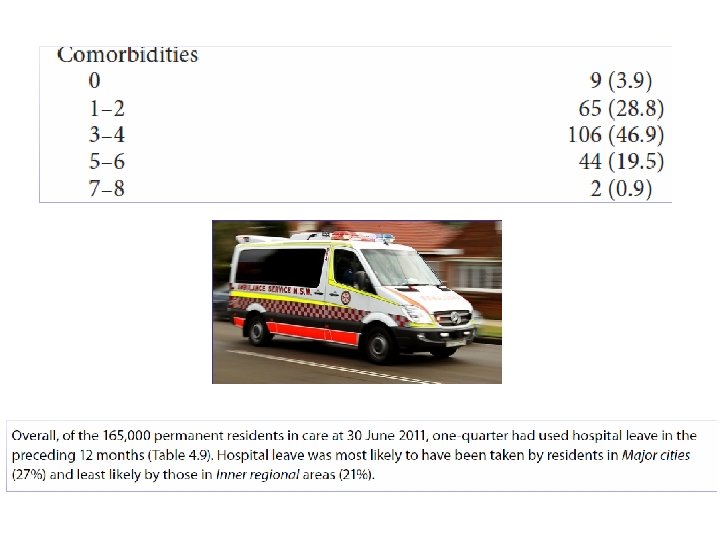
What does this mean for medications? • 60% dementia • Sedatives, anticholinergics • <2 -3 yr life expectancy • End of life vs preventative • 4 -6 comorbidities • Polypharmacy • 25% hospitalized pa • Reconciliation, errors
Their pills
What medications do they take? No medications <1% Snowdon et al Ageing 2006
Sydney nursing home medications Snowdon et al Ageing 2006
Psychotropic use Snowdon et al Int Psychoger 2011
Medications take lots of nursing time Munyisia J Adv Nurs 2011
What is appropriate? If dramatic increase in use of oxycodone in very elderly is for pain then appropriate, if for sedation is inappropriate Bennet et al BJCP 2013
The problems
Some problems related to medications • Adverse effects of polypharmacy – Cognition, behaviour, falls, mortality, QOL – Cost $1→$1. 33 • Human rights issues and autonomy • Appropriate vs inappropriate use • Antibiotics and resistant microorganisms
Polypharmacy and CHAMP: risk per additional medication * and remained highly significant with multivariate analysis Gnjidic et al JCE 2012
Five is a reasonable definition of polypharmacy… and is the norm
Falls and fractures 10% of hip fractures in Australia are attributable to benzodiazepines Cummings Le Couteur CNS Drugs 2003
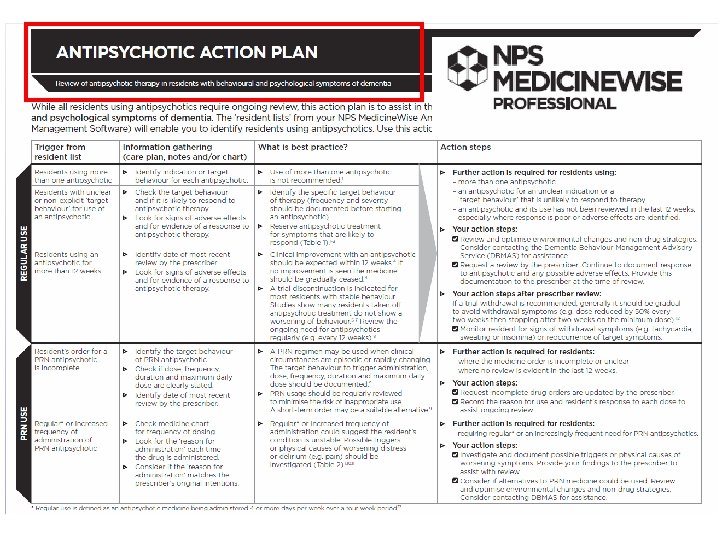
Antipsychotics in BPSD/dementia: death, strokes, falls, pneumonia Lon Schneider JAMA 2005 Meta-analysis Risk of death 1. 65 (1. 19 -2. 29) (pneumonia, stroke)
The solutions
Changing approaches to medications in RACFs • Staff turnover rapid • Access to GPs often difficult (and specialists, impossible!) • Increasing roles – Pharmacists – Nurse practitioners – Government and professional bodies
Residential Medication Management Review RMMR Nishtala et al JECP 2011
The Silverbook Do we still have the right to die as people rather than patients?
COCHRANE REVIEW 2013
• Polypharmacy DEPRESCRIBING IS A POSITIVE – Physical function, cognition, falls, institutionalization, hospitalization and death INTERVENTION TO IMPROVE QUALITY – Independent of underlying comorbidities OF LIFE, FUNCTION, COGNITION, • Deprescribing can be considered when – BEHAVIOUR Polypharmacy – Adverse effects – No efficacy AND IN MANY CASES, MORTALITY – Change in treatment goals (palliative care, frailty, dementia) Aust Presc 2011 Reeves JAGS 2013
a single cost-saving intervention that will prevent multiple diseases in older people
Thank you and acknowledgements • • • Prof Andrew Mc. Lachlan A/Prof Vasi Naganathan A/Prof Sarah Hilmer Dr Danijela Gnjidic Advocates – Margot O’Neill – Rodney Lewis – Dr Helen Creasey