Medication Errors Opioid Unintentional Overdose Epidemic Pharmacy Safety













: • Process for identifying the basic or causal factors that")


 Workbook")


















































- Slides: 79
- Medication Errors - Opioid Unintentional Overdose Epidemic - Pharmacy Safety - PMP - Forgeries
MEDICATION ERROR REPORTING • • •
16. 19. 25 ADVERSE DRUG EVENT • Incident - a drug that is dispensed in error, that is administered and results in harm, injury or death • Harm - temporary or permanent impairment requiring intervention The Pharmacist in Charge shall: A. Develop and implement written error prevention procedures as part of the Policy and Procedures Manual. B. Report incidents, including relevant status updates, to the Board on Board approved forms within fifteen (15) days of discovery. • “Significant Adverse Drug Event Reporting Form” The Board shall: A. Maintain confidentiality of information relating to the reporter and the patient identifiers. B. Compile and publish, in the newsletter and on the Board web site, report information and prevention recommendations. C. Assure reports are used in a constructive and non-punitive manner.
MEDICATION ERRORS • BOP receives sworn Complaints Alleging Misfilled Prescriptions. • Not generated from Adverse Drug Event Reports. • Most of these would not have occurred if the pharmacist complied with BOP requirements for: • Prospective Drug Review • Counseling
Medication Error Reduction
Prospective drug review Prior to dispensing any prescription, a pharmacist shall review the patient profile for the purpose of identifying: (1) (a) (b) (c) (d) (e) (f) (g) (h) clinical abuse/misuse; therapeutic duplication; drug-disease contraindications; drug-drug interactions; incorrect drug dosage; incorrect duration of drug treatment; drug-allergy interactions; appropriate medication indication.
QUESTIONED Rx’S ARE ALWAYS WRONG UNTIL PROVEN CORRECT Presume the prescription is wrong until the pharmacist has satisfied him or herself it is correct.
ONLY THE RPh CAN COUNSEL All clerks and technicians are taught that if there is a question regarding a prescription, the RPh (or intern) must take the question.
MEDICATION ERROR REDUCTION: PATIENT COUNSELING Patients need to know: Ø The name of the medication Ø How to take it Ø What it’s for Ø If the medication looks different, talk to the pharmacist http: //www. fda. gov/For. Consumers/Consumer. Updates/ucm 096403. htm accessed 6/3/16
PATIENT COUNSELING ØEstimate: half of medication-related deaths could have been prevented by appropriate and timely counseling. * ØShow the patient the drug while asking: 1) Tell me what you take this drug for? 2) Tell me how do you take the medication? -how often, and -directions for taking the medication http: //www. uspharmacist. com/continuing_education/ceviewtest/le ssonid/105916
REMEMBER THE PATIENT • Patients provide a major safety check ØCounseling – not a “veiled offer” Ø Wrong patient errors: Not opening the bag at the point of sale Ø Risk of dispensing correctly filled Rx to wrong patient at POS – about 6 per month per (community) pharmacy https: //www. ismp. org/newsletters/acutecare/showarticle. aspx? id=9 1
“To Err is Human” Building a Safer Health System • the majority of medical errors are caused by faulty systems, processes, and conditions that: • lead people to make mistakes • fail to prevent mistakes q. When an error occurs, blaming an individual does little to make the system safer and prevent someone else from committing the same error.
When an error occurs • Be compassionate ØISMP persistent safety gaffe #4 respond with empathy and concern • Evaluate and address medication use system issues ØRoot cause analysis https: //www. ismp. org/newsletters/acutecare/showartic le. aspx? id=91
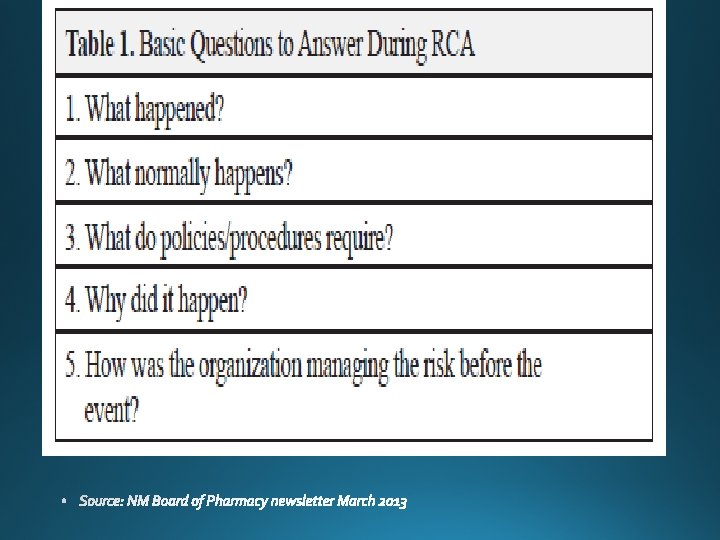
Root cause analysis (RCA): • Process for identifying the basic or causal factors that underlie variation in performance, including the occurrence or risk of occurrence of a sentinel event. • Focus is on systems and processes, not individual performance • Identifying root causes illuminates significant, underlying, fundamental conditions that increase the risk of adverse consequences. • RCA facilitates system evaluation, analysis of need for corrective action, tracking and trending
Resources: http: //www. ismp. org/community. Rx/aroc/
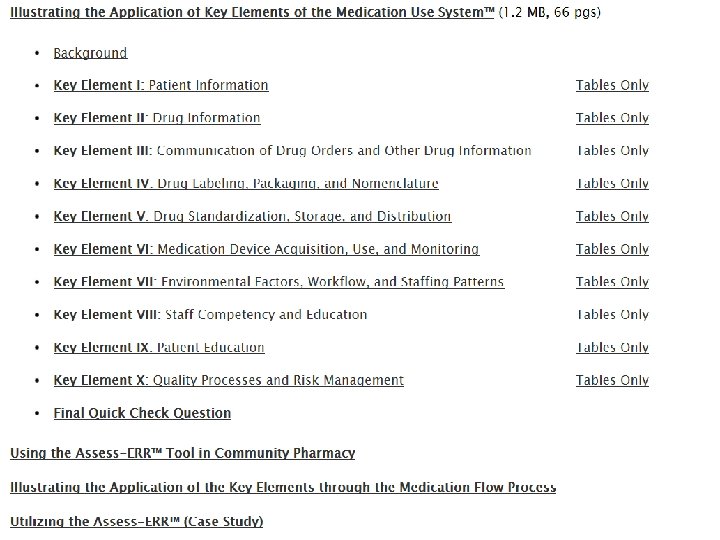
Improving Medication Safety in Community Pharmacy: Assessing Risk and Opportunities for Change
ISMP Community Pharmacy Medication Safety Tools and Resources • Root Cause Analysis (RCA) Workbook for Community/Ambulatory Pharmacy • ISMP Medication Safety Self Assessment for Community/Ambulatory Pharmacy
Resources: http: //www. nccmerp. org/
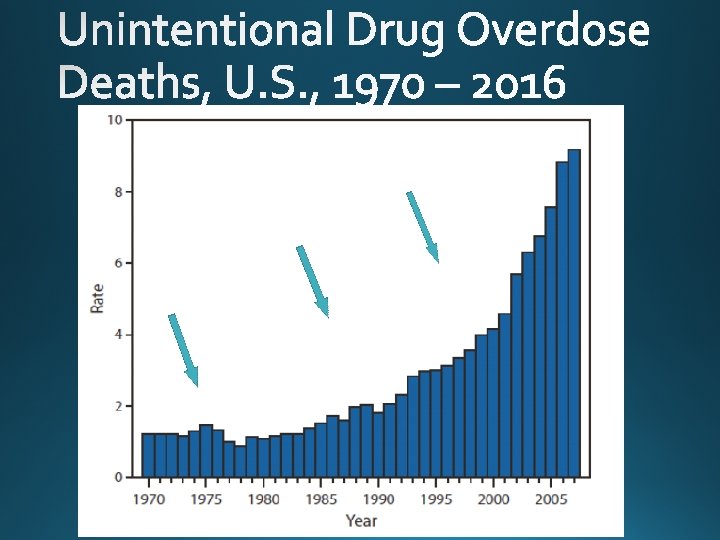
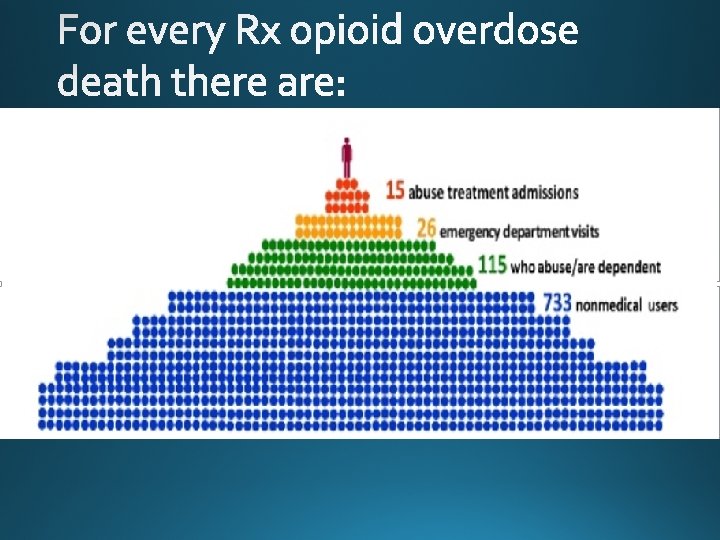
OPIOID Unintentional Overdose Epidemic, United States
http: //www. nytimes. com/interactive/2016/01/07/us/drug-overdose-deaths-in-theus. html? _r=1 By HAEYOUN PARK and MATTHEW BLOCH JAN. 19, 2016
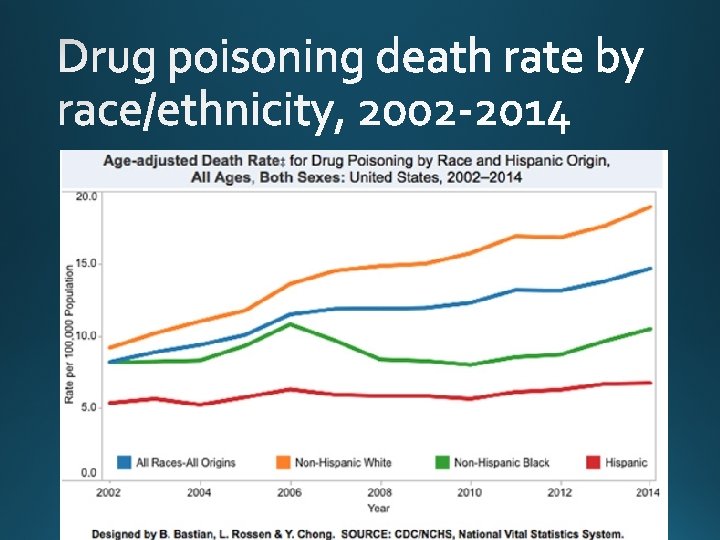
Age-adjusted rate of drug overdose deaths and drug overdose deaths involving opioids 2000 -2014 http: //www. cdc. gov/mmwr/preview/mmwrhtml/mm 6450 a 3. htm? s_cid=m m 6450 a 3_w#fig 1 accessed 1/11/2016
Source: https: //www. cdc. gov/drugoverdose/data/index. html accessed 1/3/2017
http: //www. drugabuse. gov/related-topics/trendsstatistics/overdose-death-rates
http: //www. cdc. gov/drugoverdose/epidemic/providers. html
http: //www. drugabuse. gov/publications/researchreports/relationship-between-prescription-drug-abuse-heroinuse/subset-users-may-naturally-progress-rx-opioids-to-heroin
1999 - 2014 http: //www. cdc. gov/drugoverdose/data/overdose. html
From 1999 through 2013, adults aged 55 -64 experienced the greatest increase in the opioid-analgesic poisoning death rate.
http: //www. drugabuse. gov/related-topics/trends-statistics/overdose-death-rates
http: //www. cdc. gov/vitalsigns/Prescription. Painkiller. Overdoses/index. html
http: //www. cdc. gov/vitalsigns/prescriptionpainkiller overdoses/infographic. html
http: //www. cdc. gov/drugoverdose/epidemic/risk factors. html
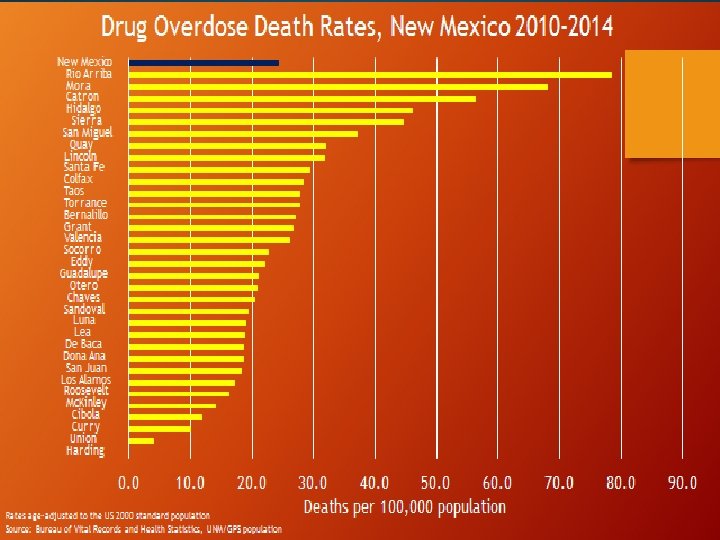
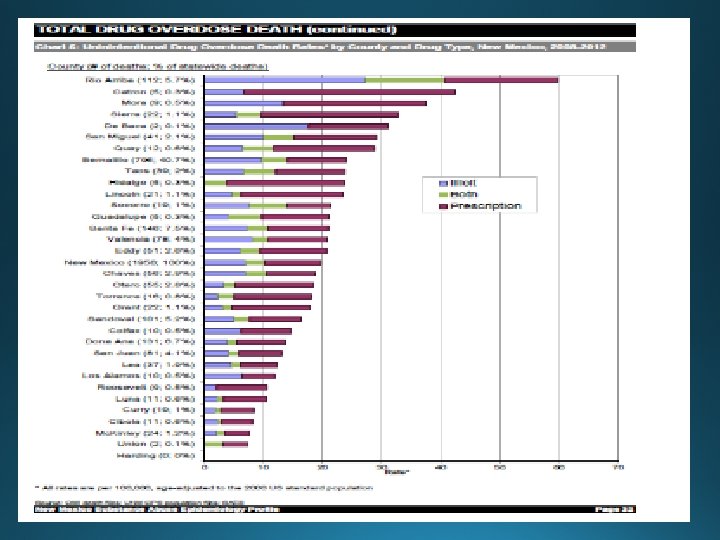
OPIOID UNINTENTIONAL OVERDOSE EPIDEMIC, NEW MEXICO
New Mexico Overdose Deaths, 2003 -2014 Source: New York Times: How the Epidemic of Drug Overdose Deaths Ripples Across America. January 19, 2016 Slide credit: James Davis, MA, Drug Epidemiologist, NM DOH
Age-adjusted rate of drug overdose deaths, 2010 and 2015 Source: CDC MMWR Increases in Drug and Opioid-Involved Overdose Deaths — United States, 2010– 2015 Weekly / December 30, 2016 / 65(50 -51); 1445– 1452
https: //www. cdc. gov/drugoverdose/data/overdose. html
Drug Overdose Death Rates, New Mexico and United States, 1990 -2015 Deaths per 100, 000 population 30 25 NM: 24. 8 20 US: 16. 3 15 Series 1 10 Series 2 5 0 Series 3 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 1920212223242526 Rates are age adjusted to the US 2000 standard population Source: United States (CDC Wonder); New Mexico (NMDOH BVRHS/SAES, 1990 -1998, 2014 ; NM-IBIS, 1999 -2013) Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH
Unintentional Injury Deaths by Year and Cause of Injury Death, NM, 1999 -2014 https: //ibis. health. state. nm. us/indicator/complete_profile/Injury. Unin ten. Death. html
Top Rx Drugs in Overdose Death, NM 2015 oxycodone alprazolam morphine diazepam hydrocodone methadone fentanyl zolpidem tramadol 0 20 40 60 Overdose death involvements Deaths may involve more than one drug Source: NM Office of the Medical Investigator Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH 80 100
Relative Risk of Prescription OD Death by Opioid Dose level, NM 2007 -2011 18. 00 Risk relative to <=20 16. 00 14. 00 12. 00 10. 00 8. 00 6. 00 4. 00 2. 00 0. 00 <=20 >20 -40 >40 -60 >60 -80 >80 -120 >120 -200 >200 Average Daily Dose (total MME/total days in 6 months) Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH
100. 00 90. 00 80. 00 70. 00 60. 00 50. 00 40. 00 30. 00 20. 00 10. 00 160+ days 90 -159 days 30 -89 days >2 00 0 20 >1 20 -1 >8 0 >6 080 060 >4 >2 0 -4 0 <30 days <= 20 Relative Risk to <=20 MME, <30 days Relative Risk of Rx OD Death by Opioid Dose and Days Prescribed in 6 months Average dose level (morphine equivalents, MME) Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH
Relative Risk of Rx opioid OD Death by days of overlap 40 Risk relative to None 35 30 25 20 Opioid 15 10 5 0 none 1 -9 10 -29 30 -89 Days of Overlap in 6 mo (different prescribers) 90+ Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH
Risk relative to None Relative risk of OD death with Opioid/sedativehypnotic overlap, NM 2007 -2011 45. 00 40. 00 35. 00 30. 00 25. 00 20. 00 15. 00 10. 00 5. 00 0. 00 Prescription Drug OD Illicit Drug OD None <10 d 10 -29 d 30 -89 d 90+d Opioid-Sedative/Hypnotic overlap days in 6 months Slide Credit: James Davis, MA, Drug Epidemiologist, NM DOH
Age-adjusted Deaths per 100, 000 Drug Overdose Death by Age, Gender, and Drug Type, NM, 2010 -2014 20 Women Men 18 16 14 12 10 8 6 4 2 0 0 -4 5 - 15 - 25 - 35 - 45 - 55 - 65 - 75 - 8 14 24 34 44 54 64 74 84 5+ Prescription Opioid 0 -4 5 - 15 - 25 - 35 - 45 - 55 - 65 - 75 - 8 14 24 34 44 54 64 74 84 5+ Heroin Both Source: UNM OMI/UNM GPS Slide credit: James Davis, DOH
1, 000 Estimated Costs of Prescription Opioid Abuse, Dependence, and Misuse, New Mexico, 2007 900 890 Dollar Amount in Millions 800 700 600 500 410 400 300 200 80 100 0 1 2 3 4 Note: New Mexico costs were estimated by multiplying estimated 2007 U. S. costs by the portion of 2007 U. S. prescription opioid overdose deaths that occurred in New Mexico (i. e. , 231/14, 408 = 0. 016). Costs for the United States were derived in Birnbaum et al (2011) “Societal Costs of Opioid Abuse, Dependence, and Misuse in the United States, ” Pain Medicine , April 12(4): 657 -67.
Rate per 1, 000 live births Rate of Neonatal Abstinence Syndrome per 1, 000 live births, NM (2000 -2013) & U. S. (20002012) 9. 00 8. 00 7. 00 6. 00 5. 00 4. 00 3. 00 2. 00 1. 00 0. 00 1 Series 1 1. 7 Series 2 1. 3 2 3 4 2. 1 1. 5 1. 7 1. 1 1. 3 5 6 7 8 9 10 11 12 13 14 1. 9 1. 6 1. 92. 95131980368749 2. 3 3. 49807778893776 3. 92156862745098 5. 54108106124546 7. 44665085951393 8. 11675939333892 1. 6 2 2. 3 2. 8 3. 6 5 5. 2 6. 1 Sources: US: Weighted national estimates from HCUP Nationwide Inpatient Sample (NIS), 2000, Agency for Healthcare Research and Quality (AHRQ), based on data collected by individual States and provided to AHRQ by the States. Total number of weighted discharges in the U. S. based on HCUP NIS = 36, 417, 565. New Mexico: 2000 -2013 Hospital Inpatient Discharge Data (HIDD). Slide credit: James Davis, MA, Drug Epidemiologist, NM DOH
Past 30 -day Painkiller Use to Get High Grades 9 -12, New Mexico, 2007 -2013
http: //www. cdc. gov/vitalsigns/heroin/infographic. html#use
OPIOID OVERDOSE AND ABUSE EPIDEMIC RESPONSE
Prescription Drug Abuse Prevention Plan • expands upon the Administration’s National Drug Control Strategy and includes action in four major areas to reduce prescription drug abuse: • Education • Tracking and monitoring • Proper medication disposal • Enforcement and-research/rx_abuse_plan. pdf http: //www. whitehouse. gov/sites/default/files/ondcp/policy-
Prescription Drug Abuse: Strategies to Stop the Epidemic October 2013 Key recommendations • Educate the public to understand the risks of Rx drug use to avoid misuse in the first place; • Ensure responsible prescribing practices, including increasing education of healthcare providers and prescribers to better understand how medications can be misused and to identify patients in need of treatment; • Increase understanding about safe storage of medication and proper disposal of unused medications, such as through "take back" programs; • Make sure patients do receive the pain and other medications they need, and that patients have access to safe and effective drugs http: //healthyamericans. org/reports/drugabuse 2013/
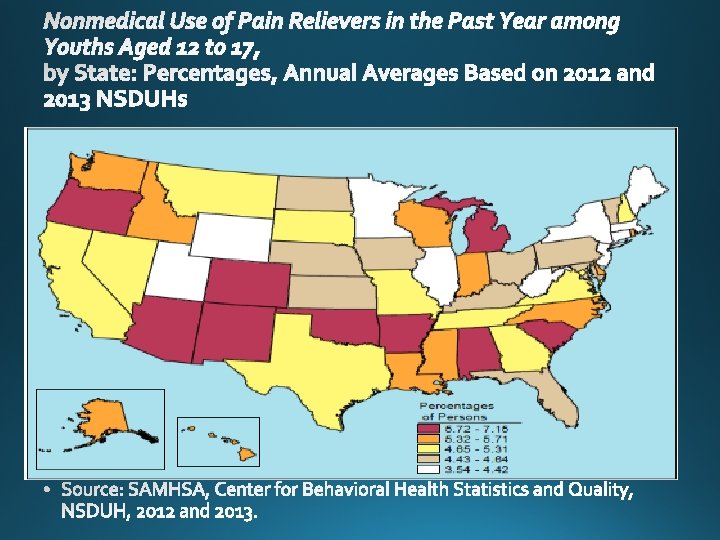
Source: 2015 National Survey on Drug Use and Health
Rx drug misuse, abuse and overdose related laws in NM • Requiring a Physical Examination before Prescribing • Setting Prescription Drug Limits • Prohibiting “Doctor Shopping”/Fraud** • Requiring Patient Identification before Dispensing • PMP utilization • Medical provider education **general language
Harm Reduction • Rescue Drug Law: ØIn 2001, NM became the 1 st state to amend its laws to make it easier to provide naloxone, and to administer (good faith, reasonable care) without fear of legal repercussions. (NMSA 24 -23 -1, 24 -23 -2; NMAC 7. 32. 7) ØMarch 2016, SB 262 / HB 277 signed into law : significantly expanded naloxone access (possess, store, distribute, prescribe, administer). NMSA 24 -23 -1 ØNaloxone standing orders (issued NM DOH March 2016) Ø Any person acting under a standing order issued by a licensed prescriber may store or distribute an opioid antagonist Ø A licensed prescriber may directly or by SO prescribe, dispense, or distribute an opioid antagonist to (several categories)
Harm Reduction • Good Samaritan Law: In 2007, NM became the 1 st state to amend its laws to encourage summoning aid in the event of an overdose. (NMSA 30 -3127. 1 )
Source: The Network for Public Health Law, last updated April 2015
http: //www. cdc. gov/vitalsigns/heroin/infographic. ht ml#use
Household Pharmaceutical Disposal Program http: //www. cabq. gov/police/programs/pharmaceuticals/ / • Six area command substations, Monday through Friday from 8 a. m. to 5 p. m. Complete list is on the web page. • Household medications • Only pills, no chemo or medical waste web page has instructions and details.
http: //findtreatment. samhsa. gov/
Pharmacy Safety
Rx. PATROL. COM
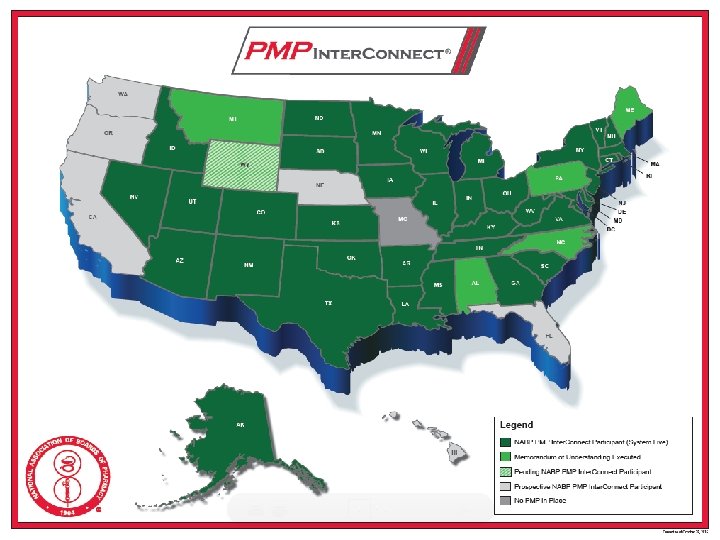
PMP
https: //newmexico. pmpaware. net/login
Duties of a pharmacist • A RPh SHALL REQUEST AND REVIEW A PMP REPORT IF: • PERSON EXHIBITS POTENTIAL ABUSE/MISUSE OF OPIATES • OVER-UTILIZATION • EARLY REFILLS • MULTIPLE PRESCRIBERS • SEDATED/INTOXICATED • UNFAMILIAR PATIENT • PAYING CASH INSTEAD OF INSURANCE
Duties of a pharmacist • A RPh SHALL REQUEST AND REVIEW A PMP REPORT IF: • OPIATE Rx FROM UNFAMILIAR PRACTITIONER • OUT OF STATE OR USUAL GEOGRAPHIC AREA
Duties of a pharmacist • A RPh SHALL REQUEST AND REVIEW A PMP REPORT IF: • providing opiates for a patient that is receiving chronic pain management prescriptions.
High Risk Prescribing Patterns • Long term use of opioids • High doses of opioids • Overlapping prescriptions of opioids from different prescribers • Multiple Provider Episodes ( MPE: Doctor and pharmacy shopping) • The combination of opioids and sedativehypnotics • The combination of opioids, benzodiazepines and carisoprodol
FORGERIES • ARE THE FOLLOWING PRESCRIPTIONS • STOLEN Rx FORMS? • PHOTOCOPIED PRESCRIPTIONS? • COMPUTER SCANNED PRESCRIPTIONS?