Medical treatment of obesity F Hosseinpanah M D

Medical treatment of obesity F. Hosseinpanah, M. D Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences 4 th August, 2018 Tehran

Agenda • • Introduction Sibutramine Orlistat Lorcaserin Combination therapy liraglutide Conclusion

Outcome Measures • • Weight Waist W/H ratio Lipid profile BP , HR Hb A 1 c , c peptide , Insulin Conversion of IGT to DM
 • Percentage weight")
Measures of weight loss • Mean weight loss ( Kg ) • Percentage weight loss • Percentage of individuals losing ≥ %5 or ≥ %10 of baseline weight • Maintenance of weight loss during study • Absolute weight loss (i. e. in excess of placebo )

Potential benefits of weight loss • Weight loss in overweight and obese patients even as little as five to ten percent of initial body weight – is associated with an improvement in cardiovascular risk factors (Goldstein 1992; Blackburn 1995; Colditz 1995)


Obesity Guidance: Efficacy Criteria ¨ US FDA criteria at the end of year 1: ¨ Mean placebo subtracted weight loss > 5% ¨ Proportion of subjects who lose > 5% of baseline body weight is greater in drug vs. placebo treated group ¨ EMEA* criteria at end of year 1: ¨ mean placebo subtracted weight loss > 10% ¨ Proportion of patients who lose > 10% of baseline body weight is greater in drug vs. placebo treated group *Europeans Medicines Evaluation Agency

Goals of therapy • The ideal outcome is a return to normal body weight, but this is unrealistic. • Effective therapy: • Weight loss > 2 kg during the 1 st month • Weight loss > 5% below baseline by 3 to 6 months • Remain at this level • Weight loss of 10 – 15 % : very good response • Weight loss > 15% : Excellent response

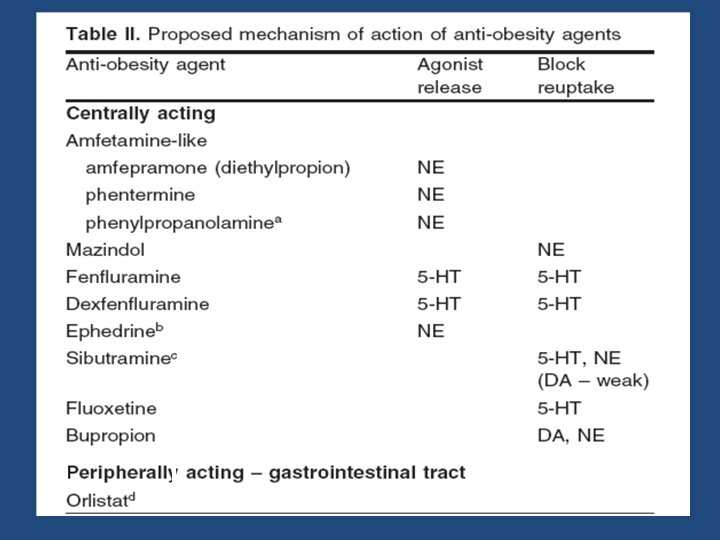
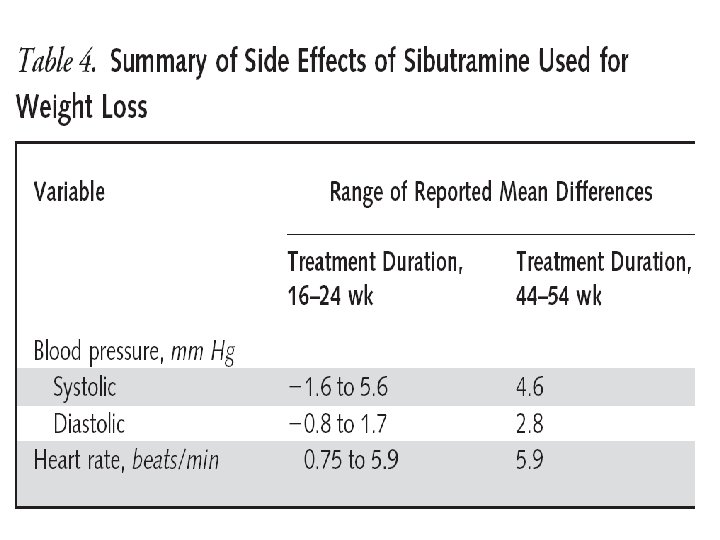
Sibutramine The brand name is Meridia Sibutramine induces weight loss primarily through its effects on food intake and to a lesser degree through its effect on metabolic rate. Sibutramine affects serotonin and norepinephrine metabolism in the brain by stimulating satiety at the appetite centers in the brain. Rapid absorption , peak plasma concentration are reached within one or two hours

• ARCH INTERN MED/VOL 164, MAY 10, 2004
 randomized controlled trial (2) sibutramine, 10 to 20 mg/d,")
Inclusion Criteria • • (1) randomized controlled trial (2) sibutramine, 10 to 20 mg/d, was administered (3) placebo controlled trial (4) overweight or obese subjects (BMI≥ 25) (5) subjects were aged 18 years or older (6) weight loss was assessed (7) 8 week duration or longer (8) 29 studies were pooled

")
-5. 06(-6. 16 to-3. 96)
")
-4. 45 Kg(-5. 29 to -3. 62)

Methods • Subjects: 9804 overweight or obese subjects, 55 years of age or older, with preexisting cardiovascular disease, type 2 diabetes mellitus. , underwent random assignment to sibutramine (4906 subjects) or placebo (4898 subjects) • F/U: 3. 4 years • Primary end point: nonfatal myocardial infarction, non fatal stroke, resuscitation after cardiac arrest, or cardiovascular death

Sibutramine Placebo HR P value Primary endpoint 11. 4% 10% 1. 16 (1. 03 1. 31) 0. 02 Non fatal MI 4. 1% 3. 2% 1. 28 (1. 04 1. 57) 0. 02 Non fatal Stroke 2. 6% 1. 9% 1. 36 (1. 04 1. 77) 0. 03
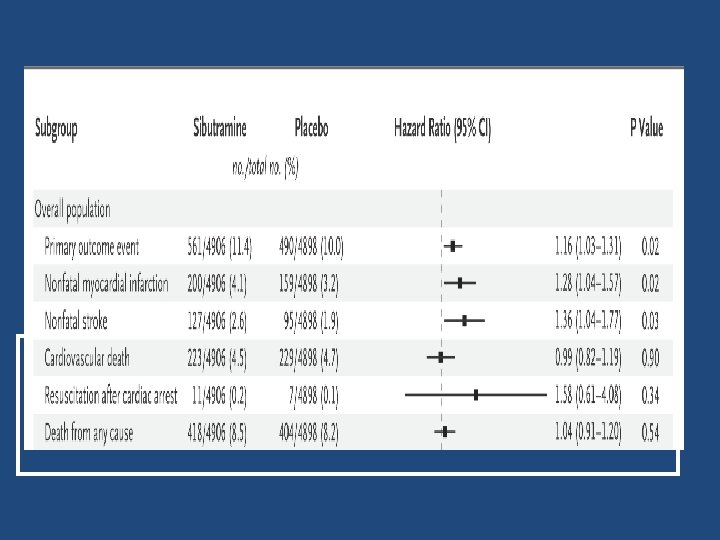
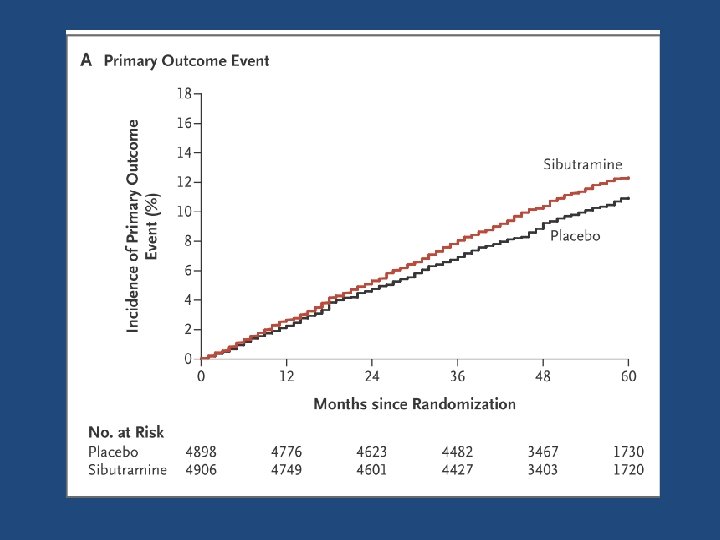
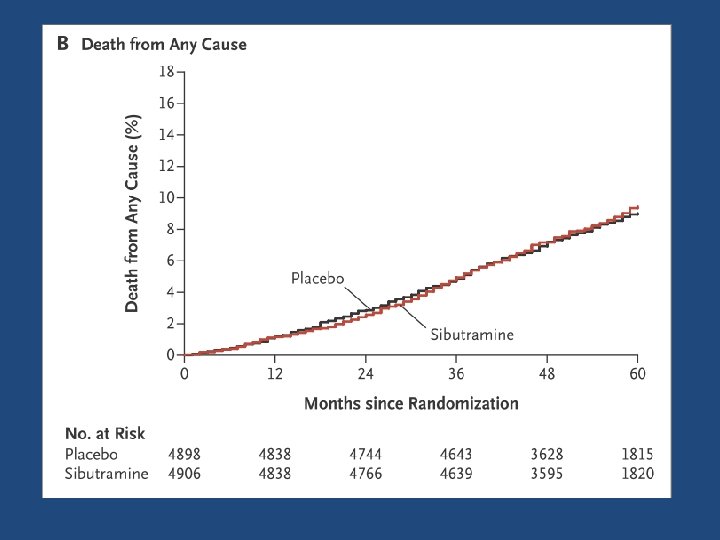

Key message • Subjects with preexisting cardiovascular conditions who were receiving long term sibutramine treatment had an increased risk of nonfatal myocardial infarction and nonfatal stroke but not of cardiovascular death or death from any cause.

Orlistat It inactivates pancreatic lipase that is involved with fat digestion , and about 30 percent less fat is absorbed.

Orlistat meta analysis • 22 studies were pooled • Average , 48 years • Average BMI , 36. 7 Kg/m� • Seventy three percent were women Meta-Analysis: Pharmacologic Treatment of Obesity, Ann Intern Med. 2005; 142: 532 -546
")
-2. 75 Kg (-3. 31 to -2. 20)

N = 3305 , BMI ≥ 30 F/U = 4 y Diet + placebo VS DIET + orlistat ( 120 mg TDS ) DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004

Attrition rate = %54 in the orlistat and %34 in the placebo

What About Side Effects? • Gastrointestinal symptoms – – – Increased flatus Abdominal discomfort Oily spotting Fecal Incontinence More severe if intake of fat is more than 100 grams. • Nutritional concerns – Fat soluble vitamins may be malabsorbed. – Daily multi vitamin is recommended

• • • Double blind randomized clinical trial Sample size : 3182 (obese or overweight) Intervention : lorcaserin (10 mg) twice daily Length of F/U : 2 years Primary outcomes : weight loss at 1 year and maintenance of weight loss at 2 years N Engl J Med 2010; 363: 245 -56.

High attrition rate • The rates of completion of year 1 of the study were 55. 4% in the lorcaserin group and 45. 1% in the placebo group • The overall rate of completion of year 2 of the study was 72. 6% of patients who completed year 1
 20. 3% 7. 7%")
47. 5% 22. 6%) 20. 3% 7. 7%

5. 8± 0. 2 kg with lorcaserin and 2. 2± 0. 1 kg with placebo

The loss was maintained in more patients who continued to receive lorcaserin during year 2 (67. 9%) than in patients who received placebo during year 2 (50. 3%, P<0. 001)

Adverse events • Rate of cardiac valvulopathy was not increased with the use of lorcaserin • Among the most frequent adverse events re ported with lorcaserin were headache, dizziness, and nausea • The rates of serious adverse events in the two groups were similar

Key message • In conjunction with behavioral modification, lorcaserin was associated with significant weight loss and improved maintenance of weight loss, as compared with placebo

Another failure • On September 16, 2010, the drug was rejected by a vote of nine to five due to the concern that weight loss efficacy in nondiabetic overweight and obese subjects was marginal • In addition, animal studies suggested that lorcaserin may cause tumors in rats

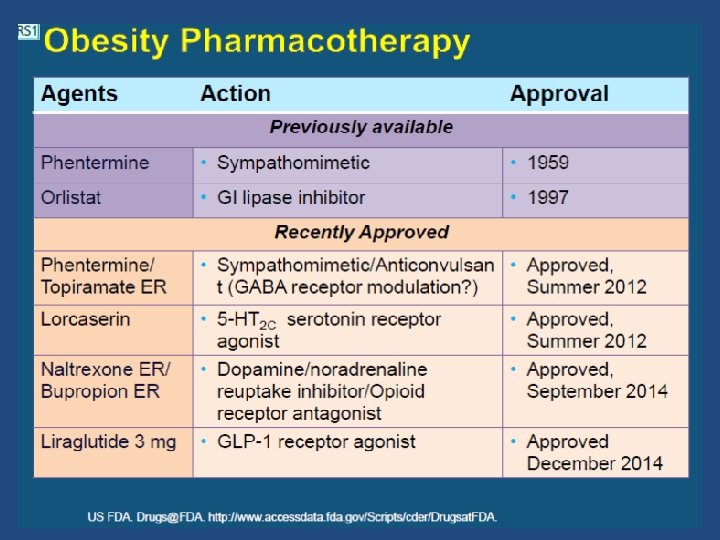
Recent approval! • On 27 June 2012, the FDA officially approved lorcaserin for use in the treatment of obesity for adults with a BMI equal to or greater than 30 or adults with a BMI of 27 or greater who "have at least one weight related health condition, such as high blood pressure, type 2 diabetes, or high cholesterol



Combinations of drugs that produce weight loss • • Phentermine and Fenfluramine Phentremine with Topiramate Phentremine with Zonisamide Naltrexone with Bupropion Initial data have been published on all these combinations, but longer term studies are needed to evaluate the potential drug-drug interaction and side effects.

Combinations of drugs that produce weight loss Effects of low-dose, controlled-release, Phentermine plus Topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Gadde KM. et al. Lancet. 2011 Apr 16; 377(9774): 1341 -52 Obesity Clinical Trials Programme, Duke University Medical Center, Durham, USA

CONQUER Trial Effects of Phentermine plus Topiramate on body weight

CONQUER Trial Patients with at least 5% and 10% weight loss.

New approval • In July 2012, FDA has approved extended release phentermin (7. 5 mg)plus topiramate (46 mg)

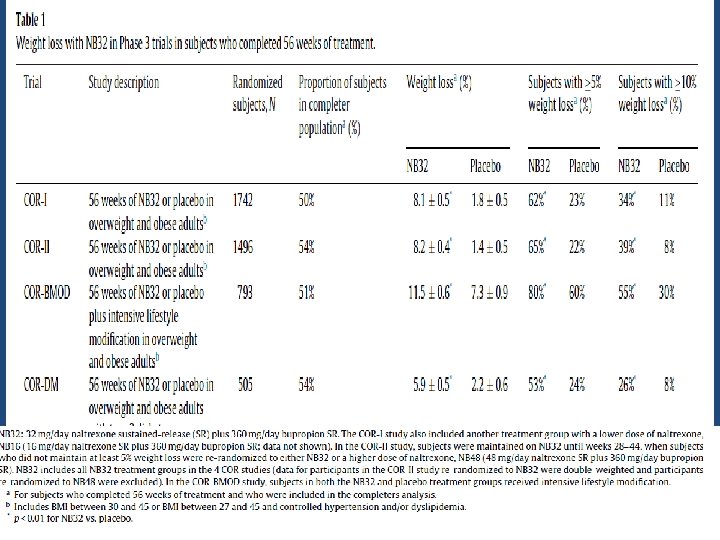
Naltrexone Hydrochloride and Bupropion Hydrochloride extended release September 10, 2014 • The effectiveness of Contrave was evaluated in multiple clinical trials that included approximately 4, 500 obese and overweight patients with and without significant weight related conditions treated for one year • Frothy two percent of patients treated with Contrave lost at least 5 percent of their body weight compared with 17 percent of patients treated with placebo
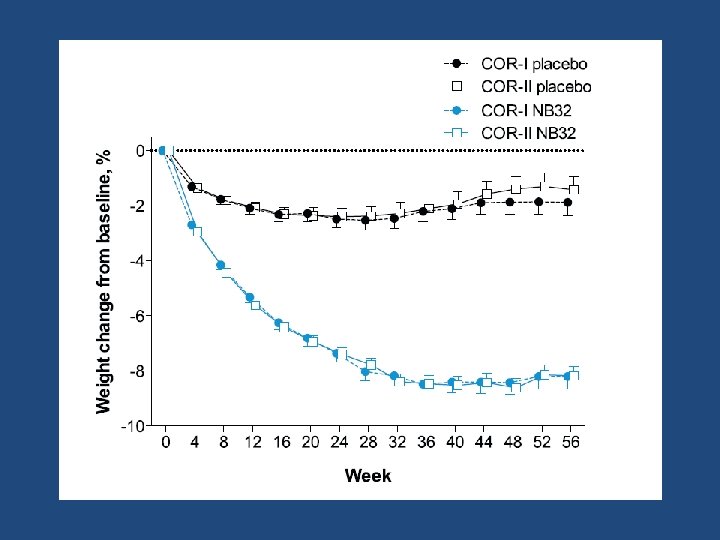
 receptor agonist's proposed brand name for obesity")
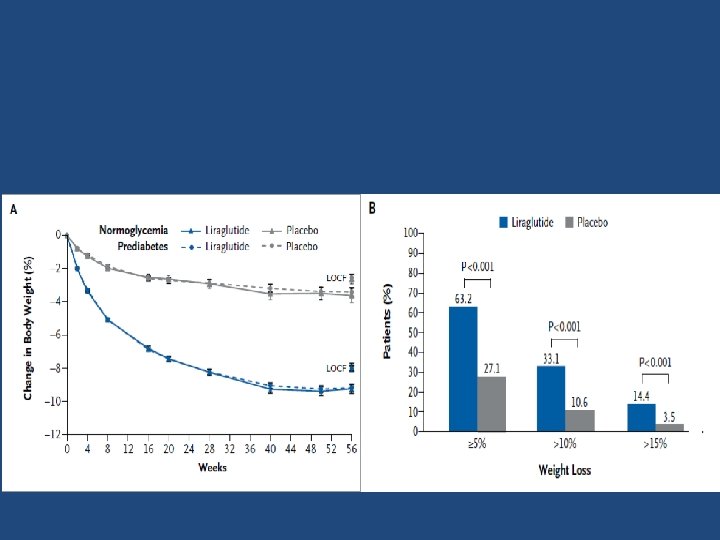
Liraglutide September 10, 2014 • (GLP 1) receptor agonist's proposed brand name for obesity is Saxenda • The dose for obesity will be 3. 0 mg, in contrast to 1. 2 or 1. 8 mg for diabetes • In largest trial involving 3731 patients, the liraglutide group lost an average 8% of body weight vs 2. 6% with placebo at 56 weeks • Significantly more patients taking liraglutide lost 5% or more of their body weight vs placebo (63. 5% vs 26. 6%)

: 1377– 1383.")
Obes Rev. 2017; 18(12): 1377– 1383.



FDA approved drugs for short term use • Benzphetamine • Diethylpropion • Phendimetrazine • Phentermine

phentermine • Six placebo controlled RCTs contributed data to the pooled analysis. • The duration of treatment with phenteramine varied from 2 to 24 weeks. • Mean Weight Change in Treated Patients Compared with Placebo (95% CI) was 3. 6 kg ( 0. 6 to 6. 0 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. Int J Obes Relat Metab Disord. 2002; 26: 262 -73

Diethylpropion • Nine Placebo controlled RCTs contributed data to the pooled analysis. • The duration of treatment with diethylpropion varied from 6 to 52 weeks. • More than 80% of enrolled individuals were female • Mean Weight Change in Treated Patients Compared with Placebo (95% CI ) was 3. 0 kg ( 1. 6 to 11. 5 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. Int J Obes Relat Metab Disord. 2002; 26: 262 -73

Critical appraisal • • • Methodological quality was moderate or good blinding High attrition rate Run in period Last observation carry forward analysis (LOCF) Younger and older people Sex , ethnicity , social class High risk vs low risk groups Recruitment method

Critical appraisal • A careful assessment of the safety of antiobesity medications may be more important than for drugs used to treat other conditions , in which the drugs are less liable to misused. • Obesity is a chronic condition. In light of this, longer term data on the effectiveness and safety would be helpful.

Pharmacotherapy Drugs approved for long-term use by the FDA may be used as part of a comprehensive weight loss program including diet and physical activity. Evidence Category B. • For patients with a BMI of 30 or above with no concomitant risk factors or diseases • For patients with a BMI of 27 or above for those with concomitant risk factors or diseases (hypertension, dyslipidemia, CHD, type 2 diabetes, sleep apnea)

Conclusions • The most well-studied medication is orlistat • Mean weight loss was 1. 3– 4. 2 kg more for orlistat 120 mg three times daily than placebo • Weight loss attributable to these medications are modest but still may be clinically significant • The maximal duration of published treatment results is four years for orlistat • When drug therapy is discontinued , weight is regained • Near maximal weight loss is achieved by six months in most trials • For obese patients with HTN or dyslipidemia , orlistat can be considered as first line • Lorcaserine has similar efficacy with orlistat and is an alternative option for those who cannot tolerate orlistat. • The efficacy for weight loss of phentermine extended release topiramate appears to be greater than either orlistat or lorcaserin, but with more side effects • The research in this field is full of removal after approval !? • Orlistat, Lorcaserin, Phentermin plus extended-release topiramate, Naltrexone hydrochloride and bupropion hydrochloride extended-release and liraglutide are FDA approved drugs for long term use

Conclusions • Pharmacologic therapy can be offered to obese patients who have failed to achieve their weight loss goals through diet and exercise alone. • However, there needs to be a doctor–patient discussion of the drugs’ side effects, the lack of long term safety data, and the temporary nature of the weight loss achieved with medications before initiating therapy.

Final solution • With better understanding of complexity of energy balance regulation • Ultimately , goal must be to use this understanding to develop more effective strategies not only for treatment , but also for the primary prevention of obesity

Thanks for your kind attention
- Slides: 66