Medical Emergencies Anuradha Perera B Sc Nspecial Respiratory
special")
Medical Emergencies. Anuradha Perera (B. Sc. N)special

Respiratory failure

Definitions • acute respiratory failure occurs when: – pulmonary system is no longer able to meet the metabolic demands of the body • hypoxaemic respiratory failure: – Pa. O 2 50 mm Hg when breathing room air • hypercapnic respiratory failure: – Pa. CO 2 50 mm Hg.

Oxygen in • Depends on – PAO 2 – Diffusing capacity – Perfusion – Ventilation-perfusion matching

Oxygen Carbon dioxide Water vapour Nitrogen

Pathophysiology
 • Intra-cardiac – Any cause of right to left shunt")
Perfusion without ventilation (Shunting) • Intra-cardiac – Any cause of right to left shunt • eg Fallot’s, Eisenmenger • Intra-pulmonary – – – Pneumonia Pulmonary oedema Atelectasis Collapse Pulmonary haemorrhage or contusion
 Intra-pulmonary • Small airways occluded ( e. g asthma, chronic")
Perfusion without ventilation (shunting) Intra-pulmonary • Small airways occluded ( e. g asthma, chronic bronchitis) • Alveoli are filled with fluid ( e. g pulm edema, pneumonia) • Alveolar collapse ( e. g atelectasis)

Brainstem Airway Lung Spinal cord Nerve root Nerve Pleura Chest wall Neuromuscular junction Respiratory muscle Sites at which disease may cause ventilatory disturbance

Respiratory Failure Symptoms CNS: Headache Visual Disturbances Anxiety Confusion Memory Loss Weakness Decreased Functional Performance

Respiratory Failure Symptoms Pulmonary: Cough Chest pains Sputum production Stridor Dyspnea

Respiratory Failure Symptoms Cardiac: Orthopnea Peripheral edema Chest pain Other: Fever, Abdominal pain, Anemia, Bleeding

Clinical • Respiratory compensation • Sympathetic stimulation • Tissue hypoxia • Haemoglobin desaturation

Clinical • Respiratory compensation – Tachypnoea RR > 35 Breath /min – Accessory muscles – Recesssion – Nasal flaring • Sympathetic stimulation • Tissue hypoxia • Haemoglobin desaturation

Clinical • Respiratory compensation • Sympathetic stimulation – HR – BP – sweating • Tissue hypoxia • Haemoglobin desaturation

Clinical • Respiratory compensation • Sympathetic stimulation • Tissue hypoxia – Altered mental state – HR and BP (late) • Haemoglobin desaturation

Clinical Altered mental state ⇓Pa. O 2 +⇑Pa. CO 2 ⇨ acidosis ⇨ dilatation of cerebral resistance vesseles ⇨ ⇑ICP Disorientation Headache coma personality changes

Clinical • Respiratory compensation • Sympathetic stimulation • Tissue hypoxia • Haemoglobin desaturation – cyanosis

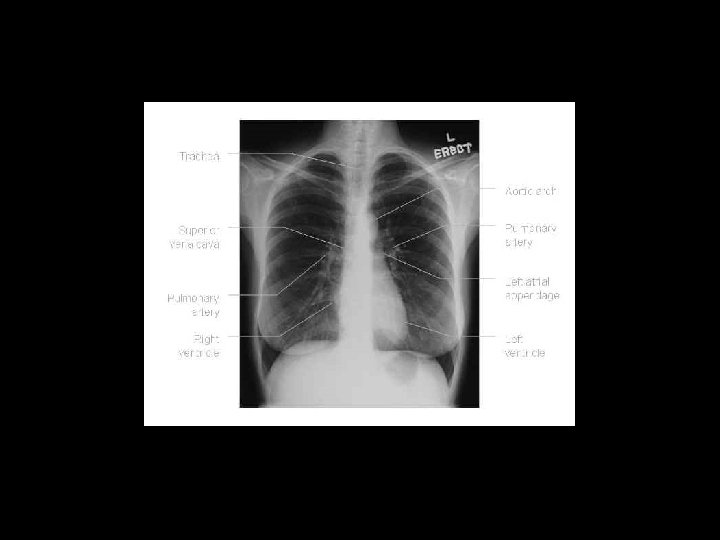
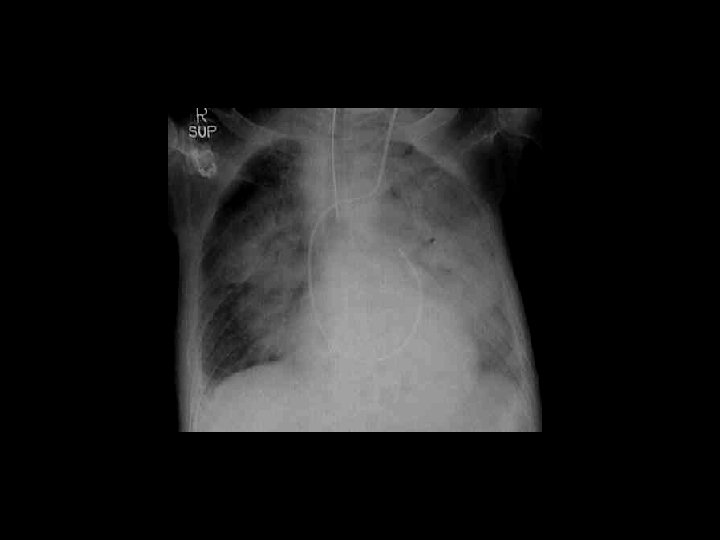
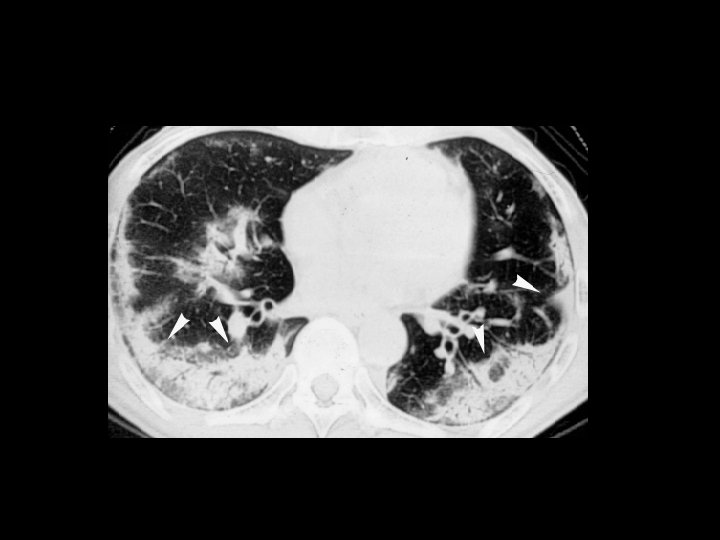
Respiratory Failure Laboratory Testing Arterial blood gas Pa. O 2 Pa. CO 2 PH Chest imaging Chest x-ray CT sacn Ultrasound Ventilation–perfusion scan
 Respiratory muscle")
Respiratory Failure Laboratory Testing Respiratory mechanics Spirometry (FVC, FEV 1, Peak flow) Respiratory muscle pressures MIP ( maximum inspiratory pressure) MEP ( maximum expiratory pressure)

Respiratory Failure Laboratory Testing Other tests Hemoglobin Electrolytes, blood urea nitrogen, creatinine Creatinine phosphokinase, aldolase EKG, echocardiogram Electromyography (EMG) Nerve conduction study

True or False • Diffusion abnormality is considered the most common cause of hypoxia.

True or False • Dead space ventilation decreases when blood flow is reduced

True or False • Shunt occurs when areas of lung are perfused but not ventilated

True or False • In myasthenia gravis mechanism of hypoxia may be due to alveoli being perfused but not ventilated

True or False • Arterial hypoxemia may be caused by alveolar hypoventilation alone

True or False • The distinction between ventilation/perfusion mismatch and intrapulmonary shunting can be made by measuring the response to the administration of 100% oxygen

True or False • There is a good relationship between dyspnea and arterial hypoxemia but a poor relationship between dyspnea and arterial carbon dioxide retention

Which of the following statements regarding the physical examination for patients with acute respiratory failure are true or false? • Central nervous examination is important • Breath sounds are commonly diminished • Supraclavicular and intercostal space muscle retractions do not correlate with increased work of breathing
 90 8 Pa. O 2 (k. Pa)")
Pulse oximetry Hb saturation (%) 90 8 Pa. O 2 (k. Pa)

Cardiac failure
 • Pain signals death of cells. •")
Heart Attack • Acute myocardial infarction (AMI) • Pain signals death of cells. • Opening the coronary artery within the first hour can prevent damage. • Immediate

Signs and Symptoms • Sudden onset of weakness, nausea, sweating without obvious cause • Chest pain/discomfort – Often crushing or squeezing – Does not change with each breath • Pain in lower jaw, arms, back, abdomen, or neck • Sudden arrhythmia with syncope • Shortness of breath or dyspnea • Pulmonary edema

Pain of Heart Attack • May or may not be caused by exertion • Does not resolve in a few minutes • Can last from 30 minutes to several hours • May not be relieved by rest or nitroglycerin

Sudden Death • 40% of AMI patients do not reach the hospital. • Heart may be twitching.

Arrhythmias Bradycardia Ventricular Tachycardia

Cardiogenic Shock • Heart lacks power to force blood through the circulatory system. • Onset may be immediate or not apparent for 24 hours after AMI.

Congestive Heart Failure • CHF occurs when ventricles are damaged. • Heart tries to compensate. • Increased heart rate • Enlarged left ventricle • Fluid backs up into lungs or body as heart fails to pump.

• You obtain a brief history while taking the patient’s blood pressure. • Your partner retrieves the nitroglycerin and obtains permission from medical control. • Your partner administers the nitroglycerin. • What else can you do at this time? You are the Provider (continued)

Focused History and Physical Exam • Medications are important! • Medications often prescribed for CHF: – Furosemide – Digoxin – Amiodarone

Focused Physical Exam • Cardiac and respiratory systems • Look for skin changes. • Lung sounds • Baseline vital signs – BOTH systolic and diastolic BP readings

Communication Relay history, vital signs, changes, medications, and treatments.

Aspirin • Administer according to local protocol. • Prevents clots from becoming bigger • Normal dosage is from 162 to 324 mg.

Nitroglycerin • Forms – Pill, spray, skin patch • Effects – Relaxes blood vessel walls – Dilates coronary arteries – Reduces workload of heart

Nitroglycerin Contraindications • Systolic blood pressure of less than 100 mm Hg • Head injury • Maximum dose taken in past hour

Nitroglycerin Potency • Nitroglycerin loses potency over time. – Especially if exposed to light • When nitroglycerin tablets lose potency: – May not feel the fizzing sensation – May not experience the burning sensation and headache • Fizzing only occurs with a potent

Assisting With Nitroglycerin • Obtain order from medical direction. • Take patient’s blood pressure. (1 of 4)
 • Check that you have right medication, patient,")
Assisting With Nitroglycerin (2 of 4) • Check that you have right medication, patient, and delivery route. • Check expiration date. • Find out last dose taken and effects. • Be prepared to lay the patient down.
 (3 of • Administer tablet or spray under tongue. •")
Assisting With Nitroglycerin 4) (3 of • Administer tablet or spray under tongue. • Have patient keep mouth closed until tablet dissolves or is absorbed.
 • Recheck blood pressure. • Record each activity")
Assisting With Nitroglycerin (4 of 4) • Recheck blood pressure. • Record each activity and time of application. • Reevaluate and note response. • May repeat dose in 3 to 5 minutes.

Ongoing Assessment • Repeat initial assessment. • Reassess vital signs every 5 minutes. • Monitor closely. • If cardiac arrest occurs, begin defibrillation or CPR immediately. • Record interventions, instructions from medical control, patient’s response. • Obtain medical control physician’s
 • Angioplasty • Cardiac")
Heart Surgeries and Pacemakers • Coronary artery bypass graft (CABG) • Angioplasty • Cardiac pacemaker
 • Maintains a regular heart rhythm and")
Automatic Implantable Cardiac Defibrillators (1 of 2) • Maintains a regular heart rhythm and rate • Do not place AED patches over pacemaker.
 • Monitor heart rhythm and deliver shocks")
Automatic Implantable Cardiac Defibrillators (2 of 2) • Monitor heart rhythm and deliver shocks as needed. • Low electricity will not affect rescuers.

Cardiac Arrest • The complete cessation of cardiac activity, either electrical, mechanical, or both.
 • AEDs come in various models. • Some operator interaction")
Automated External Defibrillator (AED) • AEDs come in various models. • Some operator interaction required. • A specialized computer recognizes heart rhythms that require defibrillation.

Potential AED Problems • Battery is dead. • Patient is moving. • Patient is responsive and has a rapid pulse.

AED Advantages • ALS providers do not need to be on scene. • Remote, adhesive defibrillator pads are used. • Efficient transmission of electricity

Non-Shockable Rhythms • Asystole • Pulseless electrical activity

Rationale for Early Defibrillation • Early defibrillation is the third link in the chain of survival. • A patient in ventricular fibrillation needs to be defibrillated within 2 minutes.

AED Maintenance • Read operator’s manual. • Check AED and battery at beginning of each shift. • Get a checklist from the manufacturer. • Report any failures to the manufacturer and the FDA.

Medical Direction • Should approve protocols • Should review AED usage • Should review speed of defibrillation • Should provide review of skills every 3 to 6 months

Preparation • Make sure the electricity injures no one. • Do not defibrillate a patient lying in pooled water. • Dry a soaking wet patient’s chest first. • Do not defibrillate a patient who is touching metal. • Remove nitroglycerin patches.
 • Assess responsiveness. • Stop CPR if in")
Using an AED (1 of 8) • Assess responsiveness. • Stop CPR if in progress. • Check breathing and pulse. • If patient is unresponsive and not breathing adequately, give
 • If there is a delay in obtaining")
Using an AED (2 of 8) • If there is a delay in obtaining an AED, have your partner start or resume CPR. • If an AED is close at hand, prepare the AED pads. • Turn on the machine.
 • Remove clothing from the patient’s chest area.")
Using an AED (3 of 8) • Remove clothing from the patient’s chest area. Apply pads to the chest. • Stop CPR. • State aloud, “Clear the patient. ”
 • Push the analyze button, if there is")
Using an AED (4 of 8) • Push the analyze button, if there is one. • Wait for the computer. • If shock is not needed, start CPR. • If shock is advised, make sure that no one
 • After the shock is delivered, begin 5")
Using an AED (5 of 8) • After the shock is delivered, begin 5 cycles of CPR, beginning with chest compressions. • After 5 cycles, reanalyze patient’s rhythm. • If the machine advises a shock, clear the patient and push shock button. • If no shock advised, check for pulse.
 • If the patient has a pulse, check")
Using an AED (6 of 8) • If the patient has a pulse, check breathing. • If the patient is breathing adequately, provide oxygen via nonrebreathing mask and
 • If the patient is not breathing adequately,")
Using an AED (7 of 8) • If the patient is not breathing adequately, use necessary airway adjuncts and proper positioning to open airway. • Provide artificial ventilations with
 • If the patient has no pulse, perform")
Using an AED (8 of 8) • If the patient has no pulse, perform 2 minutes of CPR. • Gather additional information on the arrest event. • After 2 minutes of CPR, make sure no one is touching the patient. • Push the analyze button again (as applicable). • If necessary, repeat alternating CPR/Analyze/Shock until ALS arrives. • Transport and check with medical

After AED Shocks • Check pulse. • No pulse, no shock advised • No pulse, shock advised • If a patient is breathing independently: – Administer oxygen. – Check pulse. • If a patient has a pulse but breathing is inadequate, assist ventilations.

Transport Considerations • Transport: – When patient regains pulse – After delivering six to nine shocks – After receiving three consecutive “no shock advised” messages • Keep AED attached. • Check pulse frequently. • Stop ambulance to use an AED.
 • Check unconscious patient’s pulse every 30")
Cardiac Arrest During Transport (1 of 2) • Check unconscious patient’s pulse every 30 seconds. • If pulse is not present: – Stop the vehicle. – Perform CPR until AED is available. – Analyze rhythm. – Deliver shock(s). – Continue resuscitation according to local protocol.
 • If patient becomes unconscious during transport:")
Cardiac Arrest During Transport (2 of 2) • If patient becomes unconscious during transport: – Check pulse. – Stop the vehicle. – Perform CPR until AED is available. – Analyze rhythm. – Deliver up to three shocks. – Continue resuscitation according to local protocol.
- Slides: 80