Medical Cost Containment What are the cost drivers

































 as effective as preauthorization reforms.")
 • U. S. District Court")



- Slides: 44
Medical Cost Containment – What are the cost drivers? Scott Brener, J. D. Vice President and General Counsel with SFM Mutual Insurance Company Dr. Nicholas Tsourmas Medical Director with Texas Mutual Shannon Pounds, J. D. Staff Attorney with Texas Mutual
The Context - MN n Injury rates have fallen dramatically in Minnesota… Paid claims per 100 full-time -equivalent workers, injury years 1997 -2008 Minnesota Workers’ Compensation System Report, 2008 Yet, costs since 1997 have taken a different trajectory: n System cost per $100 of payroll, 1997 -2008
The Context Medical benefits now cost more than wage benefits medical wage (inclusive of vocational rehab benefits) Minnesota Workers’ Compensation System Report 1999 and 2008
The Context Similar injuries cost more in workers’ compensation than in general health Robertson J, Corro D, Schaff D “What Can Workers Compensation Learn From Group Medical Insurance? ” NCCI Research Brief July 2005
The Current Controls Fee Schedule - Managed Care - Treatment Parameters … did work at first An 18. 5% reduction in average medical cost per claim from 1992 to 1995. Research & Statistics, Minnesota Department of Labor and Industry, 2005
The Current Controls Fee Schedule - Managed Care - Treatment Parameters … and then not so good A 68% increase in average medical cost per claim from 1997 to 2006. Research & Statistics, Minnesota Department of Labor and Industry, 2007
The Battlegrounds Provider Reimbursement / Fee Schedule Pharmaceuticals Hospital Costs Managed Care Treatment Parameters
Provider Reimbursement/Fee Schedule • Inflationary spiral • Service coverage has eroded
Pharmaceutical Dilemma Nationwide & TX Dr. Nicholas Tsourmas Medical Director with Texas Mutual
PRESCRIPTION DRUGS Misuse and Abuse 10
AT THE NATIONAL LEVEL. . . 11
FACTS Drug users at a minimum consume almost twice the medical benefits as non-users, are absent 1. 5 times as often, and make more than twice as many workers’ compensation claims. Source: U. S. Center for Substance Abuse Prevention, NCADI Most people take prescription medications responsibly; however, an estimated 48 million people (ages 12 and older) have used prescription drugs for non-medical reasons in their lifetimes. This represents 20 percent of the U. S. population. Source: Online NIDA Research Report from the Director, April 2006. 12
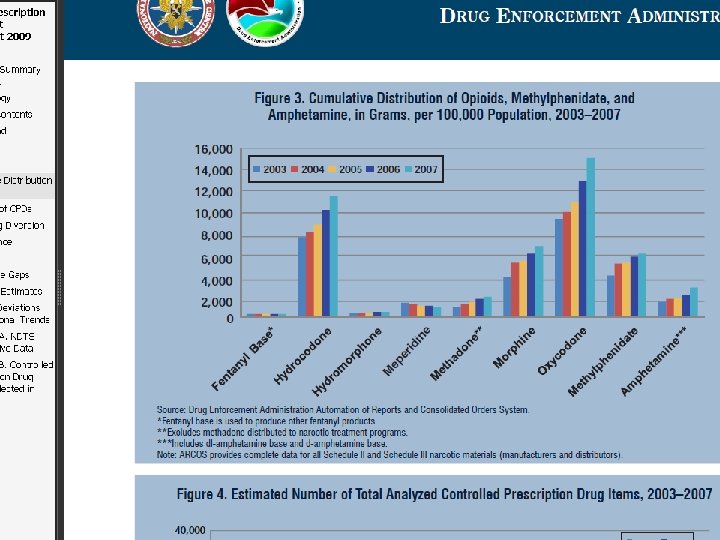
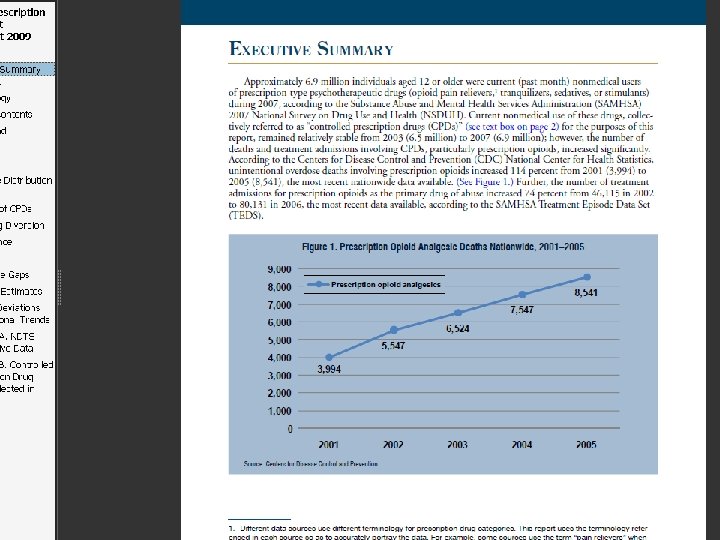
PRESCRIPTION DRUG SPENDING Increased Spending is primarily due to increased use. (Reinhardt et al. , 2004) 13
PRESCRIPTION DRUG SPENDING Prescription Drugs are consuming more health costs. (Reinhardt et al. , 2004) 14
TEXAS FACTS The total impact of alcohol and drug abuse in Texas cost the state’s economy an estimated $25. 9 billion for 2000. The cost is representative of significant direct and indirect costs in the form of reduced and lost productivity (43. 1%), crime (27. 7%), premature death (18. 6%), health care, law enforcement, property damage, motor vehicle accidents, and social welfare administration. On a per capita basis, this represents $1, 244 for every man, woman and child in Texas. Source: TCADA Media Archive, December 12, 2002 15
Types of Drugs Hydrocodone, alprazolam, and benzodiazepine products continue to comprise the majority of prescription controlled drugs abused in North Texas. Oxy. Contin has surpassed hydrocodone as the drug of choice for abusers seeking pharmaceuticals in the Tyler area. The most commonly abused pharmaceutical drugs in Houston continue to be Hydrocodone, Promethazine with Codeine and other Codeine cough syrups, and Benzodiazepines (mostly Alprazolam). Oxy. Contin abuse is on the increase, with most illegal prescriptions being written by pain management doctors. In addition to the aforementioned, commonly abused pharmaceutical drugs in San Antonio include Morphine, Dilaudid, Diazepam, Xanax, Tussionex, Lortab, Vicodin, and Ketamine. http: //www. dea. gov/pubs/states/texas. html 16
Threat Assessment The recent increase in the extent of prescription drug abuse in this country is quite likely the result of a confluence of factors, such as significant increases in the number of prescriptions; significant increases in drug availability; aggressive marketing by the pharmaceutical industry; the proliferation of illegal Internet pharmacies that dispense these medications without proper prescriptions and surveillance; and a greater social acceptability for medicating a growing number of conditions. Source: Statement by National Institute on Drug Abuse Director Nora D. Volkow, M. D. , before the Subcommittee on Criminal Justice, Drug Policy, and Human Resources, U. S. House of Representatives, July 26, 2006.
$$$$ Illicit Finance Insurance fraud is used to finance the purchase of CPDs. According to law enforcement reporting, some individuals and criminal groups divert CPDs through doctor-shopping and use insurance fraud to fund their schemes. In fact, Aetna, Inc. reports that nearly half of its 1, 065 member fraud cases in 2006 (the latest year for which data are available) involved prescription benefits, and most were related to doctor-shopping, according to the Coalition Against Insurance Fraud (CAIF). CAIF further reports that diversion of CPDs collectively costs insurance companies up to $72. 5 billion
$$$$$ Individual insurance plans lose an estimated $9 million to $850 million annually, depending on each plan’s size; much of that cost is passed on to consumers through higher annual premiums. CAIF also reports that a typical doctor-shopper can cost insurers between $10, 000 and $15, 000 per year in total costs related to diversion as well as emergency room treatment, hospital stays, physician’s office visits, tests, and rehabilitation.
Addressing the Issue RX Program Letter to treating doctor-medication profile Response-positive changes or no changes Peer Review Second letter with Peer Response-positive changes or no changes Telephonic contact with doctor by designated physician • Consideration to MQRP • • •
New Solutions in Minnesota: Pharmaceutical Treatment Parameter Initiatives Scott Brener, J. D. Vice President and General Counsel SFM Mutual Insurance Company
New Solutions- In Process • New treatment parameters for commonly used medications o. Rules requiring use of older, less expensive drugs in most situations o. Time and quantity parameters for the use of selected drugs for specific conditions
Hospital Issues in Minnesota Scott Brener, J. D. Vice President and General Counsel SFM Mutual Insurance Company
Hospital Costs More services are being provided by hospitals Hospital charges have risen faster than those of other providers (except pharmacies) Only a small proportion of hospital services are subject to meaningful cost controls WC pays 85 -100% of the bill compared to 46 -65% paid by other types of insurance
Hospital Costs Medical Fee Schedule Does not apply at all to small hospitals* - They are paid 100% of whatever they bill for both in-patient and outpatient services ( * small hospitals have less than 100 beds – set by statute) And, there is no fee schedule for in-patient services at large hospitals - They are paid 85% of whatever they bill for in-patient services
Hospital Costs Implants Prior proposals included: Limited mark-up: o 50% for devices ≤ $500 o 30% for devices from $500. 01 to $1000. 00 o 25% for devices > $1000. 00
Managed Care in Minnesota Scott Brener, J. D. Vice President and General Counsel SFM Mutual Insurance Company
Managed Care Number of plans has dropped from 10 in 1995 to 3 currently Plans are not allowed to negotiate payments with network providers Plans are required to provide a large set of services even if duplicative of insurer activities Employees are not required to use the network
Managed Care Research in a number of states shows that managed care reduces both medical & indemnity costs with the same functional outcomes In other states, up to 15% of the reduction in costs is due to negotiation of fees with network providers In other states, costs are up to 10% lower when employees are required to use the network
Treatment Guidelines Shannon Pounds, J. D. Staff Attorney with Texas Mutual
Cost containment strategy: treatment guidelines Texas adopted Official Disability Guidelines – Treatment in Workers’ Compensation, effective May 2007, for all non-emergency, non-network health care. Follow up to reforms to preauthorization requirements: spinal surgery (2002), work hardening/conditioning and rehab services (2004), and PT/OT (2005)
Timeline of the Reforms
Cost containment strategy: treatment guidelines Effects of reforms: • Excessive service utilization has reduced significantly since 2003: Total costs decreased by 24% Average claim cost lower by 17% 12% from effects of preauthorization reforms (2006) 5% from effects of adoption of ODG (2007) and residual preauthorization effect • Reductions mainly in physical medicine services, especially chiropractic services
Cost containment strategy: treatment guidelines Treatment guidelines not (yet) as effective as preauthorization reforms. • Preauthorization reforms had immediate effects due to regulatory requirements • No universal approach to how we use treatment guidelines Cannot just start denying care Prescription medications
Cost driver: legal challenges Gianzero v. Wal-Mart (filed 3/24/09) • U. S. District Court of Colorado • Class action (certified on 3/29/10) All persons who have received or have attempted to obtain, or will in the future receive or attempt to obtain workers’ comp benefits for compensable injuries sustained while an employee of Wal-Mart • Violations of RICO and Colorado Consumer Protection Act
Gianzero v. Wal-Mart • Allegation: Defendants conspired to control and manipulate the system of medical care providers that provides medical treatment to employees of Wal-Mart who are injured on the job. • Lead plaintiff injured thumb in 2005. ALJ found that Concentra delayed referral to specialist Treatment protocols did not cover chiro visits Preauth required for PT and specialist referrals
Cost driver: aging workforce Degenerative conditions • Current science → evidence-based medicine • Disputes/acceptance of conditions, not body parts • Strengthened causation standards Transcontinental Ins. Co. v. Crump, 2010 WL 3365339 (8/27/10) “Producing cause” means "a substantial factor in bringing about the injury or death and without which the injury or death would not have occurred. "
QUESTIONS?