Medical Care In Diabetes Bijan Iraj MD Assistant

Medical Care In Diabetes �Bijan Iraj, MD Assistant Professor of Internal Medicine and Endocrinology Department of Endocrinology and Metabolism Isfahan Medical School.

Management of Type 2 Diabetes Mellitus DX HIS PE LAB + ECG REFFERAL TARGET HBA 1 C
 Mean plasma glucose")
Correlation of A 1 C with Estimated Average Glucose (e. AG) Mean plasma glucose A 1 C (%) mg/dl mmol/l 6 126 7. 0 7 154 8. 6 8 183 10. 2 9 212 11. 8 10 240 13. 4 11 269 14. 9 12 298 16. 5 These estimates are based on ADAG data of ~2, 700 glucose measurements over 3 months per A 1 C measurement in 507 adults with type 1, type 2, and no diabetes. The correlation between A 1 C and average glucose was 0. 92. A calculator for converting A 1 C results into estimated average glucose (e. AG), in either mg/dl or mmol/l, is available at http: //professional. diabetes. org/Glucose. Calculator. aspx.

Treat the patient, not the blood sugar.

�Lifestyle modification �Lipid treatment �BP control �ASA+/�Cigarette cessation �Glucose control


Lifestyle intervention

Lifestyle Therapy § medical nutrition therapy § regular physical activity § sufficient amounts of sleep § behavioral support § smoking cessation and avoidance of all tobacco products. � Lifestyle therapy begins with nutrition counseling and education. � All patients should strive to attain and maintain an optimal weight through a primarily plant-based diet high in polyunsaturated and monounsaturated fatty acids, with limited intake of saturated fatty acids and avoidance of trans fats.

Pharmacotherapy of DM 2 �Efficacy: Hb. A 1 c �Hypoglycemia �Weight �Side effects �Durability �Cardiovascular/CNS outcome �CKD �NAFLD/NASH �Cost
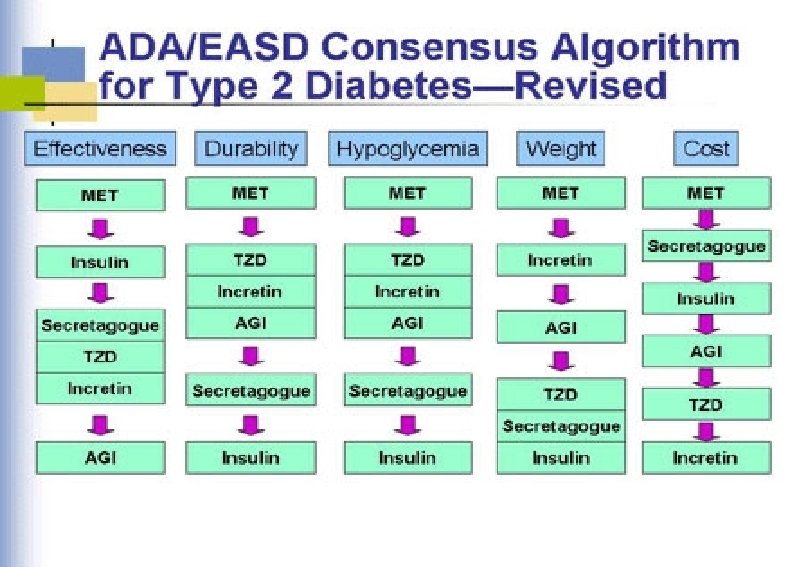

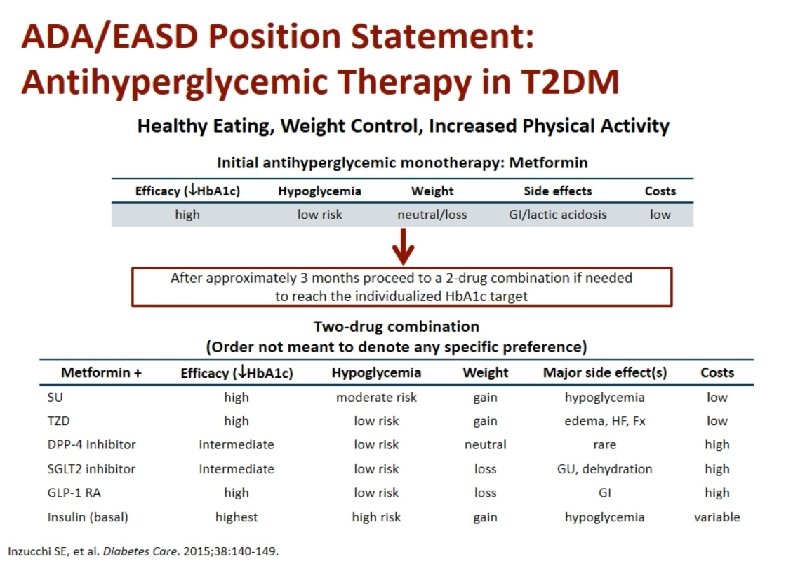
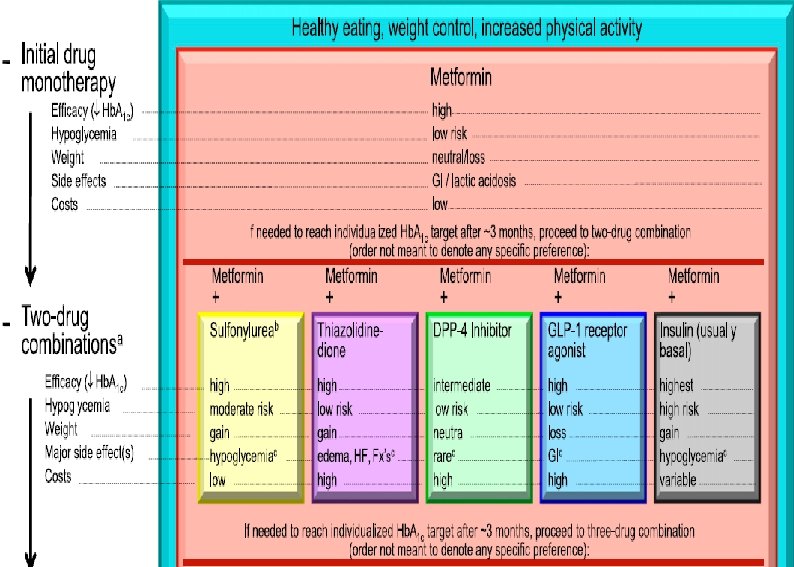
ADA Guideline, Diabetes Care 2016 Healthy eating, weight control, increased physical activity Initial monotherapy MET Not at target Hb. A 1 c after ~3 months Two-drug combinations SU TZD DPP-4 i SGLT-2 i TZD DPP-4 i GLP-1 RA Insulin SGLT-2 i SU TZD GLP-1 RA Insulin GLP-1 RA Insulin SU TZD Insulin TZD DPP-4 i GLP-1 RA SGLT-2 i Not at target Hb. A 1 c after ~3 months Three-drug combinations Not at target Hb. A 1 c after 3 -6 months combination therapy with insulin More complex strategies Basal Insulin + GLP-1 RA or Prandial Insulin ADA Guideline, Diabetes Care, January 2016

Clinical challenge: Selecting the appropriate treatment for your patient Sulfonylureas Metformi n 0. 0 Glinides Hb. A 1 c reduction (%) 0. 5 1. 0 1. 5 DPP-IV inhibitors 0. 5 -0. 7 1. 5 1. 0 -1. 5 GLP-1 RAs TZDs 1. 0 -1. 5 0. 5 - 0. 8 ≥ 2. 5 2. 0 2. 5 3. 0 Efficacy as mono therapy Insulin is the most effective glucose-lowering agent Nathan DM. N Engl J Med. 2007; 356: 437 -40 Nathan et al. Diabetes Care. 2009; 32: 193 -203 Anti diabetic agents

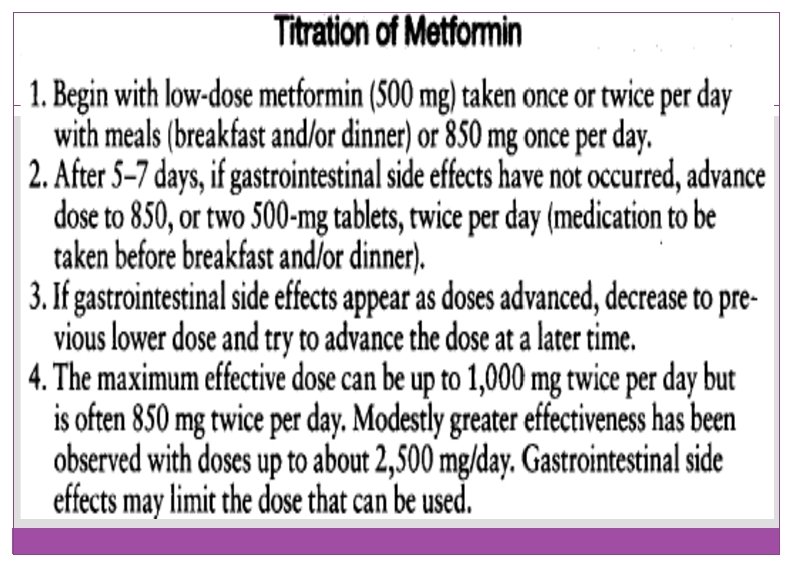
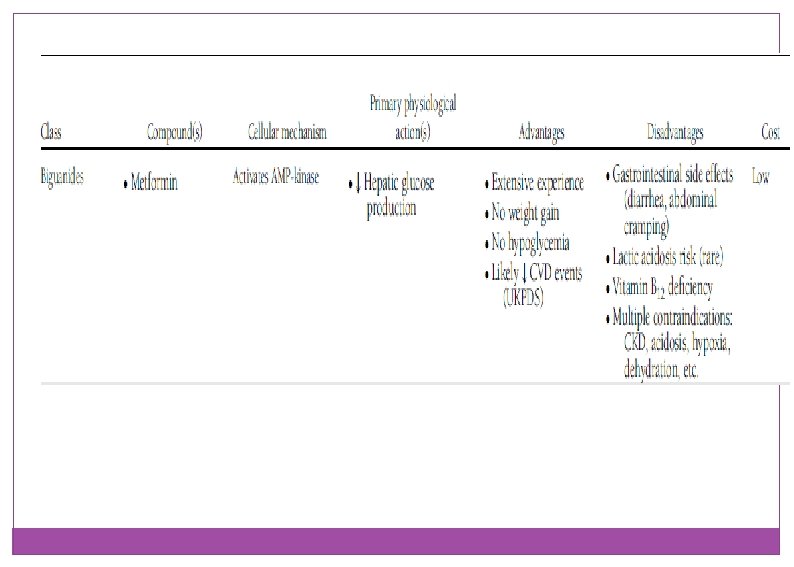
Insulin sensitizer with predominant action in the liver: Metformin: v. Dose v. Adverse events v. Titration

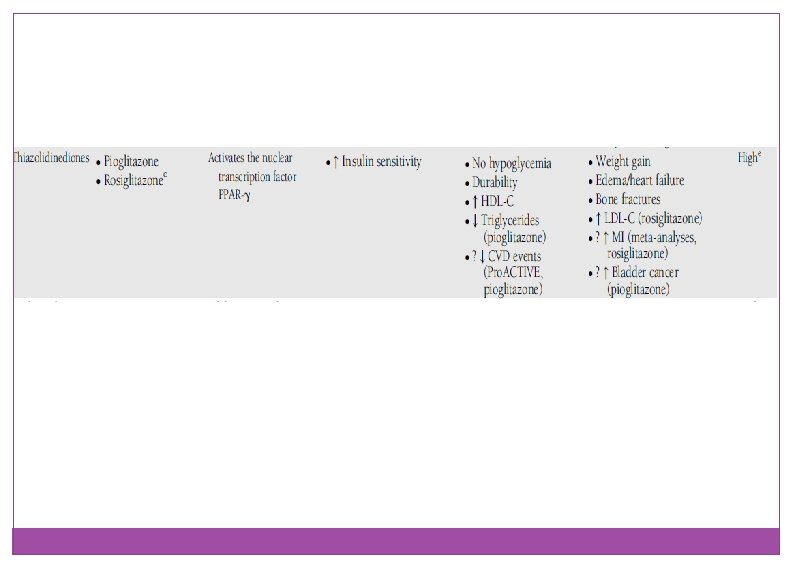
Insulin sensitizer with predominant action in Peripheral: TZD Pioglitazon: v. Dose v. Advers events

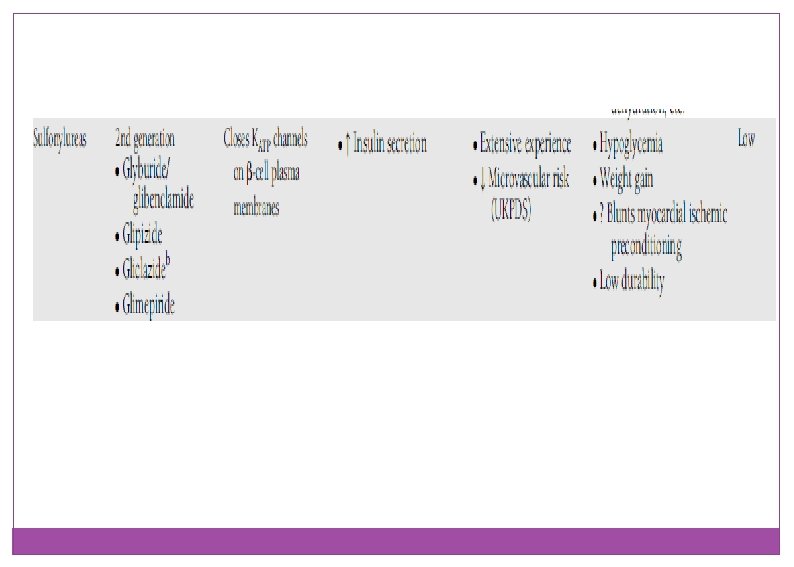
Insulin secretagogues: sulfonylureas Meal plane and Regularity: v. Dose v. Potency v. Age v. Drug interaction v. Indications

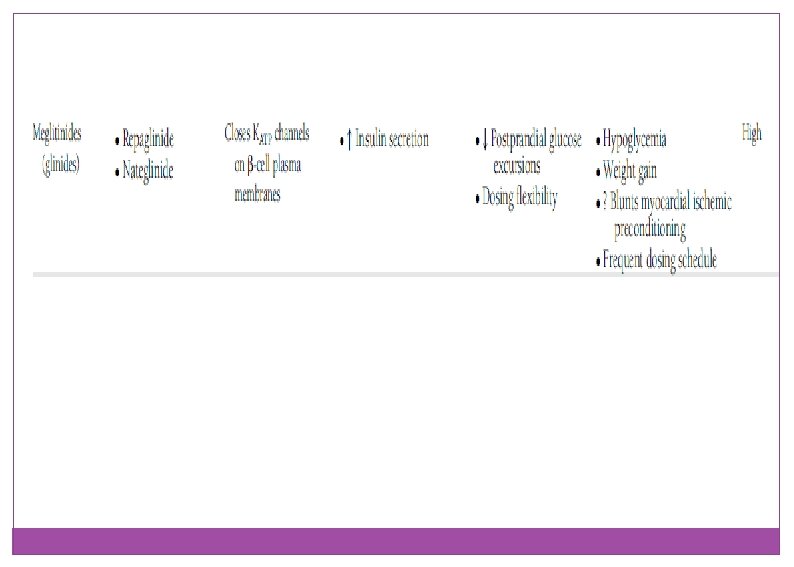
Hypoglycemia due to SUR Glibenclamid �Glimiprid �Glicloasid Repaglinid/nateglinid SR Glipizid � MR Gliclazid

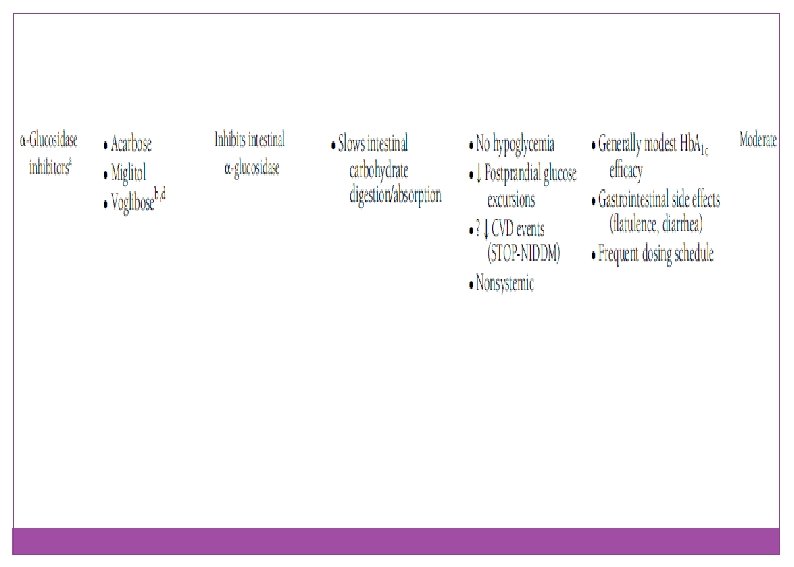
Carbohydrate absorption inhibitors α-glucosidose inhibitors Acarbose: v. Dose v. Adverse events

GLP-1 Secretion and Inactivation Mixed meal Intestinal GLP-1 release T 1/2 = 1 to 2 min GLP-1 (7 -36) active DPP-4 GLP-1 (9 -36) inactive (>80% of pool) Adapted from Deacon CF, et al. Diabetes. 1995; 44: 1126 -1131.
")
Inhibition of DPP-4 Increases Active GLP-1 Mixed meal Intestinal GLP-1 release GLP-1 (7 -36) GLP-1 active DPP-4 inhibitor Adapted from Rothenberg P, et al. Diabetes. 2000; 49(suppl 1): A 39. GLP-1 (9 -36) inactive

Incretin – Based therapies DPP-4 Inhibitors: v Sitagliptin v Linagliptin v Saxagliptin v Alogliptin

Incretin – Based Therapies GLP 1 agonists: v Exenetide v Liraglutide v Exenetide QW

Sodium Glucose Co-Transports 2 inhibitors SGLT 2 IS

Targeting the Kidney Chao EC, et al. Nat Rev Drug Discovery. 2010; 9: 551 -559.

The Kidneys Play an Important Role in Glucose Control Normal Renal Glucose Physiology • 180 g of glucose is filtered each day • Virtually all glucose reabsorbed in the proximal tubules & reenters the circulation • SGLT 2 reabsorbs about 90% of the glucose • SGLT 1 reabsorbs about 10% of the glucose • Virtually no glucose excreted in urine Mather, A & Pollock, C. Kidney International. 2011; 79: S 1 -S 6.

SGLT 2 Inhibitors in Phase 3 Development • Empagliflozin • Canagliflozin • Dapagliflozin • Ipragliflozin

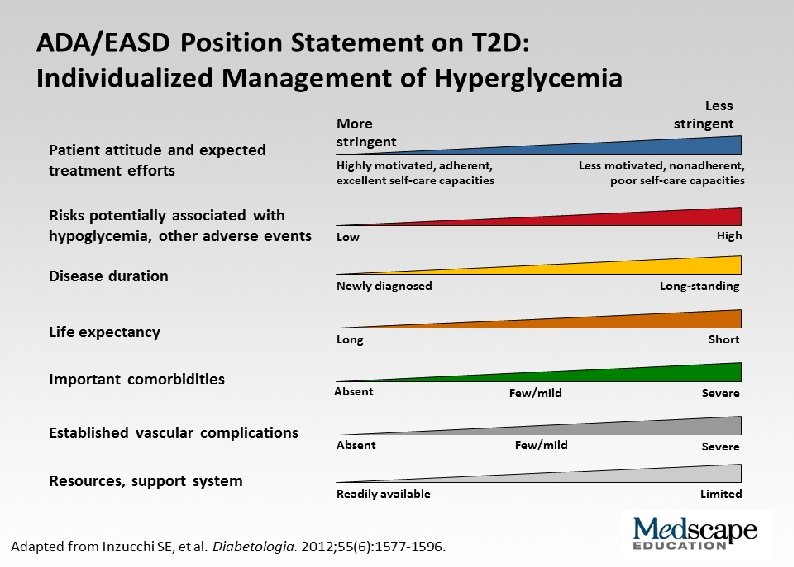
ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • • Age Weight Sex / racial / ethnic / genetic differences Comorbidities - Coronary artery disease Heart Failure Chronic kidney disease Liver dysfunction Hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Age: Older adults - Reduced life expectancy Higher CVD burden Reduced GFR At risk for adverse events from polypharmacy More likely to be compromised from hypoglycemia üLess ambitious targets üHb. A 1 c <7. 5– 8. 0% if tighter targets not easily achieved üFocus on drug safety Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Weight - Majority of T 2 DM patients overweight / obese Intensive lifestyle program Metformin GLP-1 receptor agonists ? Bariatric surgery Consider LADA in lean patients Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Metformin: CVD benefit (UKPDS) Ø Avoid hypoglycemia Ø ? SUs & ischemic preconditioning Ø ? Pioglitazone & CVD events Ø ? Effects of incretin-based therapies Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction Ø Metformin: May use unless condition is unstable or severe Ø Avoid TZDs Ø ? Effects of incretin-based therapies - Hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

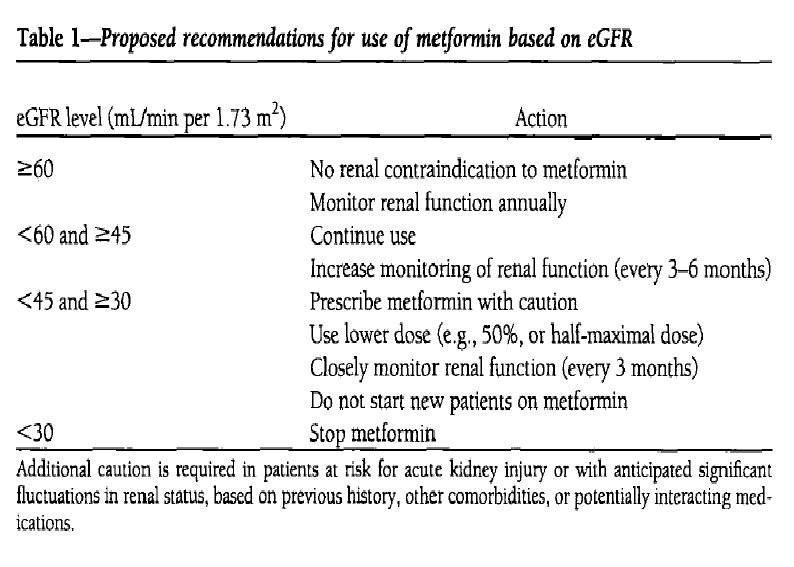
ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Increased risk of hypoglycemia Ø Metformin & lactic acidosis § US: stop @SCr ≥ 1. 5 (1. 4 women) § UK: dose @GFR <45 & stop @GFR <30 Ø Caution with SUs (esp. glyburide) Ø DPP-4 -i’s – dose adjust for most Ø Avoid exenatide if GFR <30 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Most drugs not tested in advanced liver disease Ø Pioglitazone may help steatosis Ø Insulin best option if disease severe Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print

ADA-EASD Position Statement: Management of Hyperglycemia in T 2 DM 4. OTHER CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Emerging concerns regarding association with increased mortality Ø Proper drug selection in the hypoglycemia prone Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print
 Lifestyle measures Usual approach Then, at each step, if")
IDF treatment algorithm (2013 update) Lifestyle measures Usual approach Then, at each step, if not to target (generally Hb. A 1 C<7. 0%) Alternative approach Consider first line Sulfonylurea or α-glucosidase Metformin Consider second line Sulfonylurea Metformin (if not first line) or α-gluc or DPP-4 or TZD or GLP-1 agonist Consider third line Basal insulin or premix insulin or Consider fourth line Basal + mealtime insulin Basal or pre-mix (later basal+mealtime) IDF 2013 Global Guidelines for Type 2 diabetes

Recommended standards of care for patients with type 2 Diabetes Mellitus v Weight at each visit v Bp at each visit v Blood glucose monitoring individualized v Hb. A 1 C at 3 -mo intervals v at diagnosis and then yearly v Dilated v v eye exam Lipid profile Urine micro albumin

- Slides: 57