Medical billing and coding Achieving success Objectives Identify

Medical billing and coding: Achieving success

Objectives • Identify BWC’s payment methodologies. • Discuss new strategies to facilitate appropriate bill payment. • Show the importance of understanding and providing medical documentation specific to BWC.
")
Provider Fee Schedule Current methodologies • Hospital inpatient services – Diagnosis Related Groups (DRG) reimbursement system • Level I HCPCS codes – Resource Based Relative Value Scale (RBRVS) methodology • Level II HCPCS codes – Historical and third-party payer data/recommendations from professional associations. • Ambulatory surgical centers – Nine payment groups identified by Medicare • Outpatient hospital services – Cost to charge ratio (CCR) + 16% < 60% allowed charges

Provider Fee Schedule Payment rate comparisons Professional services • In general, BWC’s rates are similar to workers’ compensation payments in other states. – Comparable to Pennsylvania; higher than California, Florida and West Virginia • BWC’s payments are substantially higher than Medicare. – 22 CPT® codes accounted for 50% of total payments to physicians – Payments for these services averaged 133% of Medicare and ranged from 116– 211% of Medicare

Provider Fee Schedule Payment rate comparisons Ambulatory surgery centers • BWC’s rates are similar to workers’ compensation payments in other states. – Comparable to Florida (some higher, some lower) – Lower than Pennsylvania – Higher than West Virginia • BWC pays 133% of Medicare on average.

Provider Fee Schedule Payment rate comparisons Inpatient hospital • BWC’s DRG rates are similar to workers’ compensation payments in other states. – Slightly lower than California (115% vs. 120%) – Comparable to Pennsylvania – Higher than West Virginia • BWC pays at 115% of Medicare.

Provider Fee Schedule Payment rate comparisons Outpatient hospital BWC’s rates are similar to workers’ compensation payments in other states. – Comparable to Pennsylvania (some higher, some lower) – Higher than Florida and West Virginia BWC’s payments are difficult to compare to Medicare rates since the payment methodologies differ.

Provider Fee Schedule 2008 HCPCS Level I and II – Fee schedules (professional and supplies) ASCs – Payment groups Inpatient Hospital – DRGs Outpatient Hospital – Cost to charge ratio + 16 < 60%

Provider Fee Schedule Coding requirements • Effective Oct 1, 2007, BWC will recognize the 2008 version of the International Classification of Diseases (ICD-9 -CM). • Effective for dates of service beginning Jan. 1, 2008, BWC will recognize 2008 HCPCS Level I, Level II, and Level III codes.
 • BWC will continue to accept bills containing only BWC")
National Provider ID (NPI) • BWC will continue to accept bills containing only BWC legacy (or current) numbers, as well as bills with both the legacy number and NPI. • Verify information with BWC’s provider relations department. – Phone: (614) 644 -6292, option 3 then 0 – Fax: (614) 621 -1333 – Mail: BWC Provider Enrollment P. O. Box 182031 Columbus, OH 43218 -2031

NPI BWC will process both CMS-1500 forms and UB 04 and UB-92 • Electronic version of CMS-1500 has increased number of diagnosis code accepted to eight. • You can find line-by-line instructions in chapter 4 of BWC’s Billing and Reimbursement Manual online.

Clinical editing • Bills validated to meet health-care industry coding standards • MCOs required to use nationally recognized guidelines • Consistent with expected results

$15 K Medical-Only Claim Program • $1 K Program: Claim is medical only with date of injury (DOI) < June 30, 2006 • $5 K Program: Claim is medical only with DOI > June 30, 2006, and < Sept. 10, 2007 • 15 K Program: Claim is medical only with DOI > Sept. 10, 2007 • Participating employers will notify providers

$15 K Medical-Only Claim Program • MCO does not manage claim or reimburse for services. • Bill employer directly for services related to injuries covered by the program. • Pay all bills within 30 days of receipt as billed or according to prior agreement with medical provider.

Grievance hearing Procedure allows a provider, employer or employee to grieve a disputed bill payment, including: – Grievances involving a provider’s objection to the denial of payment or reduced payment; – Appeals regarding the recovery of overpayments. It does not address BWC fee schedule grievances or alternative dispute resolution (ADR) issues.
 776 • Payment made for a non-allowed, related condition •")
Explanation of benefits (EOB) 776 • Payment made for a non-allowed, related condition • Supporting medical documentation needed to substantiate determination to override and pay the bill

Appropriate use of EOB 776 Treatment authorized by MCO based on Miller Criteria for condition not specifically allowed in the claim, but related to the allowed condition. • Injured worker develops a post-operative infection which may resolve within a few weeks. • Injured worker develops post-operative complications, such as deep vein thrombosis or pulmonary embolism, which could require re-hospitalization • IW develops complications related to treatment for the allowed conditions i. e. adverse reaction to the medications

Appropriate use of EOB 776 • Treatment not requiring prior approval is provided and billed with a non-allowed ICD -9. • Symptoms indicating that further diagnostic studies are necessary to determine if a more extensive work-related injury (than previously believed) has occurred.

Inappropriate use of EOB 776 • The condition is expressly denied in the injured worker’s claim. • The MCO note does not document that Miller Criteria has been met.

Inpatient hospitalizations • BWC reimburses with a version of the Medicare DRG system. BWC implemented this process beginning Jan. 1, 2007. • Approximately 6, 000 inpatient bills per year • Hospital reimbursement and review staff – Includes a certified coder

Inpatient hospitalizations • Documents necessary for the review process include: – History and physical; – ED report (if applicable); – Operative note (if applicable); – Discharge summary or progress notes if stay is more than 48 hours; – Discharge note if stay is less than 48 hours.

Inpatient hospitalizations • BWC recognizes correct coding guidelines for DRG reimbursement. • Regardless of allowed condition, coding should reflect medical record documentation of the treating physician.

Medical documentation policy E-learning • BWC Learning Center – External User Quick Tips • What is the BWC Learning Center? • It is a Web-based application that can be accessed here: www. bwclearningcenter. com.

Medical documentation policy E-learning To search for or enroll in a learning event using the BWC Learning Center, follow these instructions. • Visit www. bwclearningcenter. com. • Click First Visit. • Enter your (or your employer’s) BWC policy number, your first name and last name. • Enter a login ID and a password of your choice. • Click Submit. • Complete a User Profile.

Medical documentation policy E-learning • If your name is entered in the system, you will be directed to contact BWC. – E-mail: BWCLearning. Center@bwc. state. oh. us. com – Phone: 1 -800 -OHIOBWC, option 2, 2, 2 • To update your user profile, follow these instructions. – – – From the home page, click User Information Center. Click Student Records. Click Update Profile. Edit as needed. Click Submit to save changes.

Medical documentation policy E-learning To enroll in a learning event, follow these instructions. • From the home page click on the Learning Center building/icon. • Click on Course Information & Enrollment. • Search by keyword, entering a word(s) that is closely related to the desired training event. • Click Search.

Medical documentation policy E-learning To enroll in a classroom learning event, follow these instructions. • From the returned list, locate the desired course and click on the information icon. • In the lower right section of the screen, locate the date/location of your choice. • Click Enroll. • If you have given an e-mail address, you will receive an e-mail confirming your enrollment.

Medical documentation policy E-learning • If you have no e-mail address, you will receive a fax or letter. • Once you are enrolled, you can view your list of selected classes (and cancel, if needed) in the Personal Learning Center, which is located on the left side of the home page. To take an online learning event, follow these instructions. • From the returned list, locate the desired online course and click on the title. • Click Take Course.

Medical documentation policy E-learning To access the Personal Learning Center, follow these instructions. – On the left side of the home page, click on Personal Learning Center. – The list will display current learning events (classroom session enrollment and online tutorial stated). – Click the Transcript tab. – Locate the learning event (classroom or online) you have completed. – Click on Certificate. – A survey will open if required for completion of the learning event. – When certificate displays click the Print icon to print it.
 services • E&M services are primarily the same as")
Documentation Evaluation & Management (E&M) services • E&M services are primarily the same as CMS rules with changes instituted for BWC purposes. • Only one E&M service per injured worker per day will be reimbursed. • Credit given for additional effort required to treat a new injury or revise return-to-work restrictions.

Documentation Established patient • Injury or worsening of the condition that causes a repeat office visit requiring a more thorough evaluation • May include an injured worker with a new injury, though the injured worker, based on accepted terminology, is considered an established patient

Documentation Social history • This criterion could be met by a thorough occupational history. • It’s often necessary for documentation of causality and return-to-work restrictions.

Documentation Examination Either ‘ 95 or ‘ 97 E&M guidelines exam criteria • ‘ 95 body areas and organ systems elements • ‘ 97 bullet system • Most favorable to provider

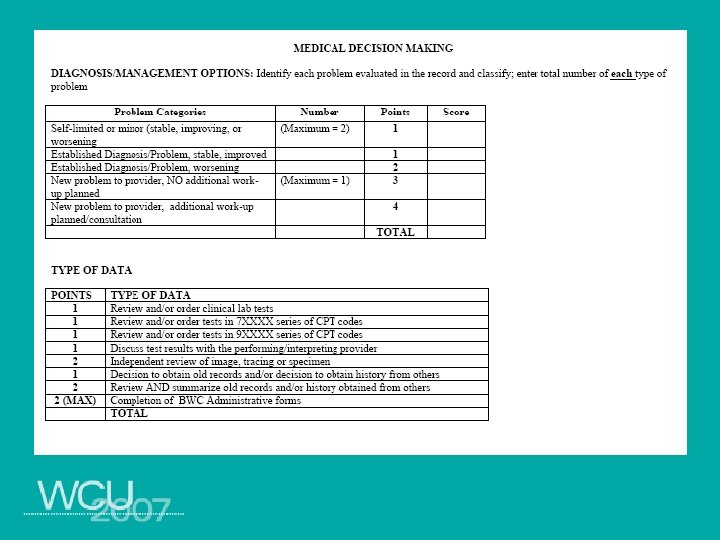
Documentation Medical decision making Number of diagnoses or management options Return-to-work restrictions: • Are essential in the management of injured workers; • Are valued as a part of management option; • May increase the complexity of management decisions.

Documentation Medical decision making Amount and/or complexity of data to be reviewed BWC administrative forms completed during a visit are: • Counted as a data element; • Worth two points, regardless of the number of forms.

Documentation Time Additional time may be considered in the selection of the E&M code if documentation indicates: • Requirement to complete forms or; • Counseling injured worker regarding return-to-work restrictions.
 • May be reimbursed • Must be")
Documentation Telephone calls (99371 -99373 CPT ®) • May be reimbursed • Must be medically necessary • Must contribute to overall care of the injured worker • Supporting documentation with a brief description of the conversation noted
 Codes are not to be used: •")
Documentation Telephone calls (99371 -99373 CPT ®) Codes are not to be used: • In addition to consultation services (9924199255) or team conferences (99361 and 99362); • For conversations with an MCO or BWC; • As a replacement for face-to-face interaction with the injured worker.

Documentation Telephone calls 99371 ® • Simple or brief – most calls will fit into this category • May be used when a provider calls the injured worker for: – Consultative reasons; – Medical management; – Coordinating medical management with other health-care professionals.

Documentation Telephone calls 99371 ® Discussion with the employer regarding an injured worker’s status • Test and/or laboratory results • Clarify or alter previous instructions • Integrate new information from other health professionals into the medical treatment plan • Adjust therapy, report on progress of treatment • Return-to-work status and job restrictions

Documentation Telephone calls 99372 ® Intermediate telephone call • To discuss and evaluate new information • To provide details or to initiate a new plan of care • Covers at least 20 minutes of provider time

Documentation Telephone calls 99373 ® Complex or lengthy telephone calls • Lengthy, emergent counseling session with an anxious or distraught patient • Detailed or prolonged discussion with family members regarding a seriously ill patient • Rare occurrence and required at least 30 minutes of provider time.

Medical documentation • Sept. 15, 2005 – Established patient • CC - Right knee pain • 40 -year-old male presents with right knee pain after tripping over an extension cord at work (K-Mart stockroom) yesterday. He is now experiencing moderate to severe pain. States he has no numbness or tingling in the lower leg, but says he has a large bruise on the back and side of his knee. He is in good health. He has an occasional cigarette. • Patient is alert and oriented. Vital signs are normal. Gait is abnormal as he cannot bear weight on the right leg. There is a large bruise on the posterior and lateral aspects of the knee. There appears to be some effusion. He is very tender to palpation. Straight leg raise is difficult to assess due to pain. Sensation is intact. • Knee pain with possible ACL tear. Will request MRI. Rx-Darvocet. N 100 mg q 6 hrs prn pain. Will call patient to schedule MRI when we receive approval.

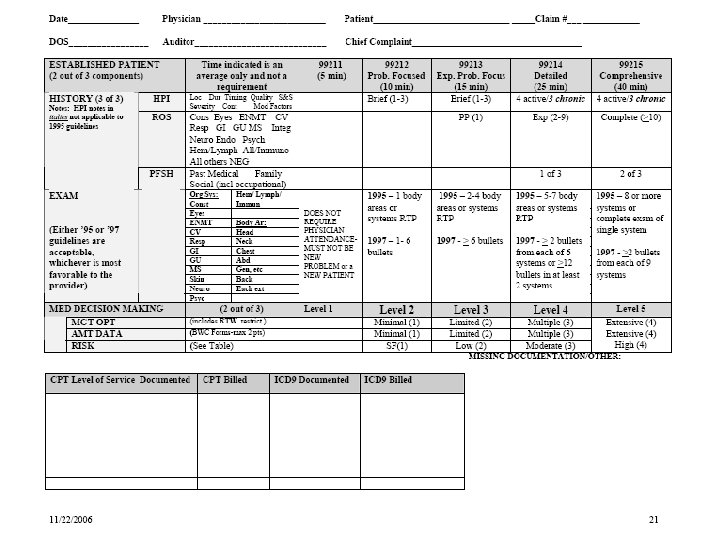
Medical documentation History • Chief complaint • History of present illness – Brief one to three elements – Extended four or more • Review of systems Exam • ‘ 95 or ‘ 97 guidelines

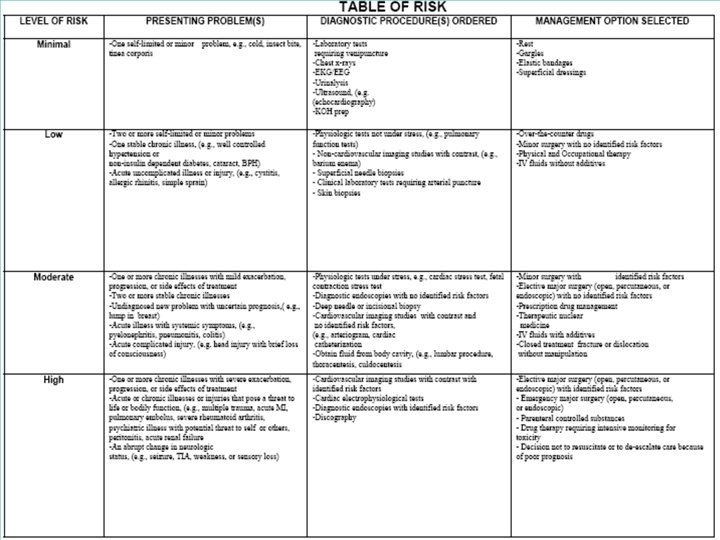
Medical documentation Medical decision making • Diagnoses or management options • Data • Risk

Documentation • Type of history • Type of exam • Complexity of medical decision making • Established patient two/three key components • CPT® code selected
 coding guidelines • Pre- and post-manipulation assessment • Pre-service")
Documentation Osteopathic manipulation therapy (OMT) coding guidelines • Pre- and post-manipulation assessment • Pre-service work includes: – Reviewing previously gathered clinical data; – Initial or interim history; – Reviewing the problem list.

Documentation OMT coding guidelines Pre-service work includes: • Pertinent correspondence or reports; • Prior care; • Review of imaging and other test results, test interpretation; • Care planning; • Other important findings.

Documentation An E&M service may be billed on the same day as OMT. • It must be significant and separately identifiable from OMT. • CPT® modifier 25 is used. Examples include: – First visit at which a patient is examined; – Significant change in the injured worker’s condition warrants an additional evaluation; – Change of medications; – Review of additional or new data; – Ordering of laboratory imaging studies, X-rays or additional studies.
 • Pre-manipulation assessment including: – Reviewing previously gathered clinical")
Documentation Chiropractic manipulative treatment (CMT) • Pre-manipulation assessment including: – Reviewing previously gathered clinical data; – An initial or interim history; – Reviewing the problem list; – Pertinent correspondence or reports.

Documentation CMT • Pre-manipulation assessment including: – – Prior care; Review of imaging and other test results, test interpretation; Care planning; Other important findings. • Outcome or response to treatment must be included. • The plan for ongoing care is noted.

Documentation CMT • You may bill E&M on the same day as CMT. • The service must be significant and separately identifiable service. • Modifier 25 is appended to the CPT® code.

Documentation CMT • Examples of E&M service billed on same day as CMT include: – First visit at which time injured worker is examined; – Significant change in injured worker’s condition. • Work not included in the CMT includes: – Review of additional or new data; – Ordering of laboratory imaging studies, X-rays or additional studies.

Documentation Physical, occupational and massage therapy documentation • Must support CPT® code submitted • Amount of time submitted for time-based physical and massage therapy codes • Inclusion of plan of care • Flow sheet of modalities and exercises with treatment • Short narrative of function and status with summary of response

Documentation Time-based guidelines Record time in the medical record, including: • Beginning and ending time of the treatment; • Time spent delivering each service. Time calculations for multiple procedures • More than one CPT® code billed during calendar day, total number of units billed is constrained by total treatment time. – 24 minutes of 97112 and 23 minutes of 97110 were furnished, total treatment time = 47 minutes. – Three total units can be billed for treatment; two units of 97112 and one unit of CPT® code 97110.

Documentation Units reported • • One unit > 8 minutes to <23 minutes Two units > 23 minutes to <38 minutes Three units > 38 minutes to < 53 minutes Four units > 53 minutes to < 68 minutes Five units > 68 minutes to < 83 minutes Six units > 83 minutes to < 98 minutes Seven units > 98 minutes to < 113 minutes Eight units > 113 minutes to < 128 minutes

Documentation Do not bill for services performed less than eight minutes. • Multiple time-based procedures – duration of any procedure is less than eight minutes and total treatment time exceeds eight minutes, figure time into total treatment time on that date. Time starts when therapist is working directly with injured worker. • Do not count pre- and post-delivery services. • Intra-service care begins when therapist or physician is directly working with the injured worker. • Injured worker should already be in the treatment area and prepared to begin treatment.

Documentation Time counted is the time the patient is treated. Example · Gait training requires both therapist and an assistant, or even two therapists, to manage in the parallel bars. · Each 15 minutes the patient is being treated can count as only one unit of CPT® code 97116. · You should not bill the time an injured worker spends not being treated.

Documentation Psychotherapy • Insight oriented, behavior modifying and/or supportive psychotherapy refers to: – – – Development of insight or affective understanding; Use of behavior modification techniques; Use of supportive interactions; Use of cognitive discussion of reality; Any combination of the above to provide therapeutic change. Note face-to-face time spent during psychotherapy in the medical record.

Documentation Submit procedure code that most closely matches face-to-face time spent with injured worker. • For example: CPT® codes – 90804: 20 to 30 minutes up to and including 44 minutes – 90806: 45 to 50 minutes up to and including 74 minutes – 90808: 75 to 80 minutes up to and including 94 minutes

Questions?
- Slides: 64