Mechanisms of Reabsorption and Secretion Dr Waleed R

Mechanisms of Reabsorption and Secretion Dr. Waleed R. Ezzat

Lecture Objectives: 1. Understand the transport and the pathways of reabsorption 2. Explain and contrast the mechanisms of electrolytes and water reabsorption in the proximal convoluted tubule, loop of Henle, and distal nephron 3. Discuss the reabsorption of glucose, urea, creatinine and protein 4. Explain how water and ion transport in any section of the nephron is altered by a change in sodium reabsorption in that section

Pathway of reabsorption: § Tubular transport is either through: § Reabsorption across the tubular epithelium (transcellular pathway) into the interstitial fluid includes: 1. 2. Transcellular pathway (through cell membranes) Paracellular pathway (through junctional spaces) 1) Active or 2) Passive transport § The peritubular capillaries behave like the venous ends of most other capillaries, i. e. moves the fluid and solutes from the interstitium into the blood.
: § Water is always reabsorbed by passive diffusion (Osmosis).")
Pathway of reabsorption (cont. ): § Water is always reabsorbed by passive diffusion (Osmosis). Reabsorption of some substances requires active transport (i. e. needs hydrolysis of ATP). Active transport could be (1) Primary or (2) Secondary (usually Co-transport such as for glucose). § Primary active transporters are: – – Na+ - K+ ATPase H+ - K+ ATPase Ca+2 ATPase § Secondary active transport mechanism is used also in the secretion of few substances such as H+. This often involves Counter-transport of the substance with Na+ ions.
")
Reabsorption of H 2 O and electrolytes: § Active transport of solutes (especially Na+) into the interstitial fluid creates a concentration difference that causes osmosis of water from the tubular lumen to the renal interstitium. § The proximal tubule is highly permeable to water and to a lesser extent to most ions, such as Na +, Cl−, K+, Ca+2, HCO 3−, and Mg+2 (Epithelial brush border increases surface area available for absorption). About 65% of filtered water and Na+ are reabsorbed by the proximal tubule. § Reabsorbed water carries with it some of the solutes (e. g. organic solutes). This is referred to as solvent drag. § Water reabsorption occurs in all regions of the renal tubule with the exception of the ascending limb of the loop of Henle and the distal convoluted tubule

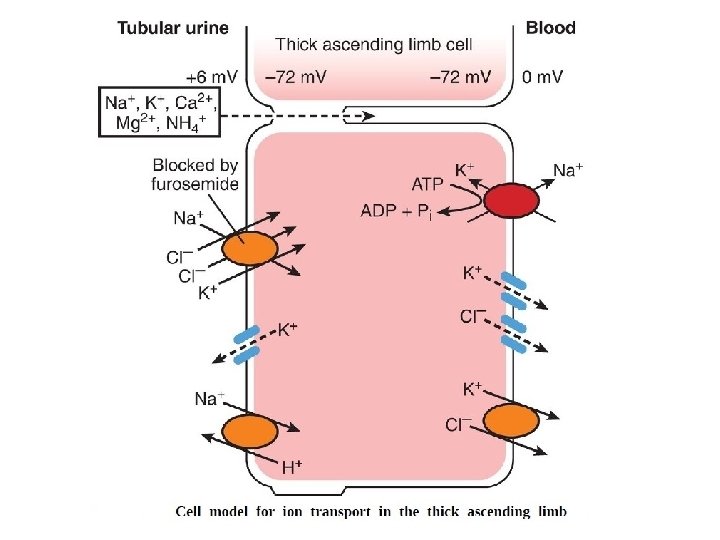
Reabsorption of H 2 O and electrolytes: § The thin and thick ascending limbs are water impermeable due to the lack of aquaporins, which are water channel proteins § Changes in Na+ reabsorption significantly influence the reabsorption of water and many other solutes. § Distal tubule, collecting tubules, and collecting ducts are less permeable to water; however, permeability can be greatly increased by ADH. § Negative ions (such as chloride) are transported along with Na+ because of electrical potential, i. e. passive diffusion through the paracellular pathway. Some chloride ions can be transported by active Co-transport mechanism. § Urea reabsorption by the proximal tubule is by passive diffusion. § As urea is freely permeable across the filtration barrier, urea concentration is the same within the Bowman capsule space as in the peritubular capillary and the adjacent interstitial fluid

Reabsorption of H 2 O and electrolytes: § The reabsorption of water increases urea concentration within the tubular fluid. The proximal tubule is freely permeable to urea. Accordingly, urea diffuses down the concentration gradient from the tubular lumen to the peritubular capillaries. This is generally thought to occur by both transcellular and paracellular routes § Na+ is reabsorbed throughout the entire tubule, with the exception of the descending loop of Henle § 99. 5% of the Na+ is reabsorbed, most occurs in the proximal tubule (~65%), with 25% in the loop of Henle, and the remaining in the distal tubule and collecting ducts § With the exception of the thin ascending limb of the loop of Henle, Na+ enters the cell from the lumen across the apical cell membrane and is pumped out across the basolateral cell membrane by the Na+/K+-ATPase § Only 7% of the filtered Na+ that is reabsorbed is used for cotransport and antiport mechanisms (i. e. secondary active transport mechanisms)


Reabsorption of H 2 O and electrolytes: Note: In the proximal tubule, an increase in the filtered load of Na+ from the glomerulus stimulates an increase in sodium reabsorption by the tubule such that the percent of sodium reabsorbed remains the same. This phenomenon is called glomerulotubular balance This phenomenon is also observed in the distal nephron when sodium load entering the distal nephron from upstream segments changes as well

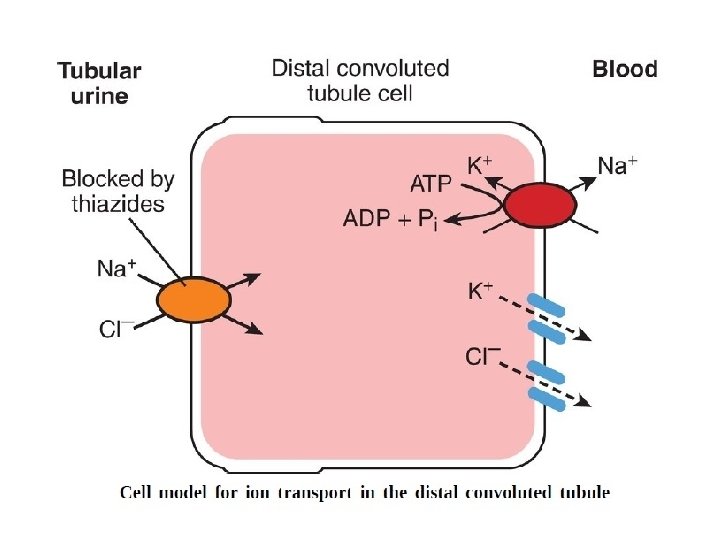
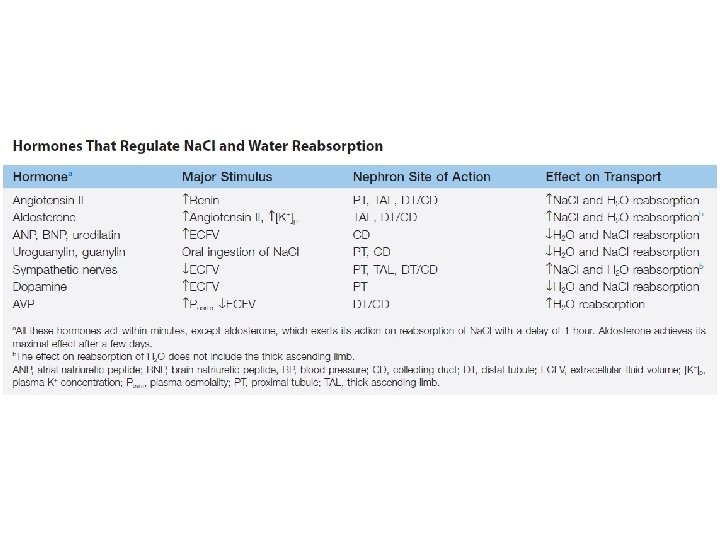
The distal nephron: § The distal nephron includes the distal convoluted tubule; and the cortical and medullary collecting ducts § The distal nephron reabsorbs much smaller amounts of salt and water. Typically, the distal nephron reabsorbs 9% of the filtered Na+ and 19% of the filtered water, compared with 65% for both substances in the proximal convoluted tubule § Unlike in the proximal tubule, Na+ and water reabsorption can be uncoupled because water permeability may be low and variable § The distal convoluted tubule is essentially impermeable to water and urea but can actively reabsorb Na. Cl by a Na–Cl cotransport. This transporter can be inhibited clinically by thiazide diuretics § Sodium reabsorption coupled with the low water and urea permeability of the distal tubular epithelium further reduces the osmolality of the tubular fluid without changing its volume or urea concentration § The collecting duct system participates in electrolyte and fluid balance through reabsorption and excretion, processes regulated by the hormones aldosterone and vasopressin (ADH)
: § Each component of the collecting duct system contains")
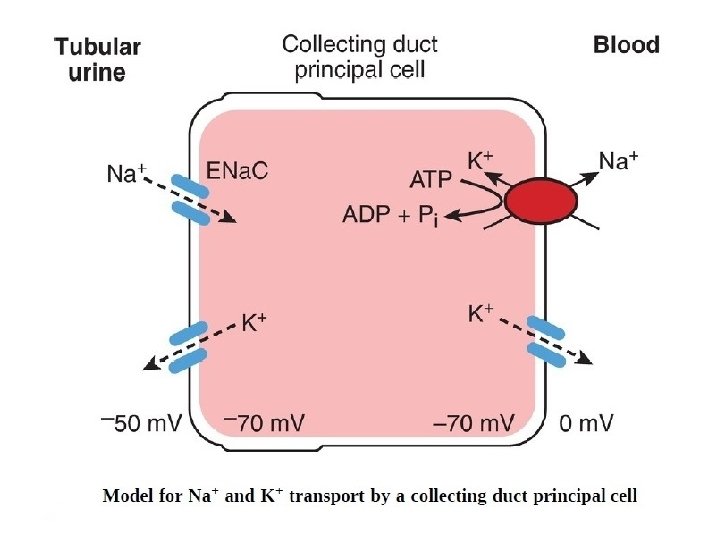
The distal nephron (cont. ): § Each component of the collecting duct system contains two cell types, principal cells and the intercalated cells § The principal cell mediates the collecting duct's influence on sodium and potassium balance via sodium channels and potassium channels located on the cell's apical membrane § Aldosterone determines expression of sodium channels (especially the ENa. C, epithelial sodium (Na) channel) in principal cells. Increases in aldosterone increase expression of luminal sodium channels. Aldosterone also increases the number of Na ⁺/K⁺ATPase pumps that allow increased Na+ reabsorption and K+ and H+ excretion. Excretion primarily occurring in the connecting ducts and cortical region of the collecting ducts § The channel can be inhibited by amiloride and similar diuretics, which are known as potassium-sparing diuretics because they do not cause the potassium loss seen with other diuretic classes § Vasopressin determines the expression of aquaporin channels that provide a physical pathway for water to pass through the principal cells § Intercalated cells come in α and β varieties and participate in acidbase homeostasis. A H+/K+-ATPase is present in the luminal cell membrane of α-intercalated cells and contributes to renal K + conservation when dietary intake of K+ is deficient

Reabsorption of glucose, urea, creatinine, and protein: § Glucose and amino acids are completely reabsorbed by secondary active transport mechanism (Co-transport). § Urea is poorly reabsorbed (passively). This results in increased tubular urea concentration because of water osmosis. Only one-half of filtered urea is passively reabsorbed. § Creatinine is a larger molecule than urea and tubular membrane is impermeable to it. Therefore, none of creatinine is reabsorbed. § Pinocytosis is the prime mechanism for reabsorption of protein especially in the proximal tubule. Inside the endothelial cell, protein is digested into its amino acids, which are reabsorbed back into the interstitial fluid by diffusion. Pinocytosis requires energy. Therefore, it is considered as a special form of active transport.

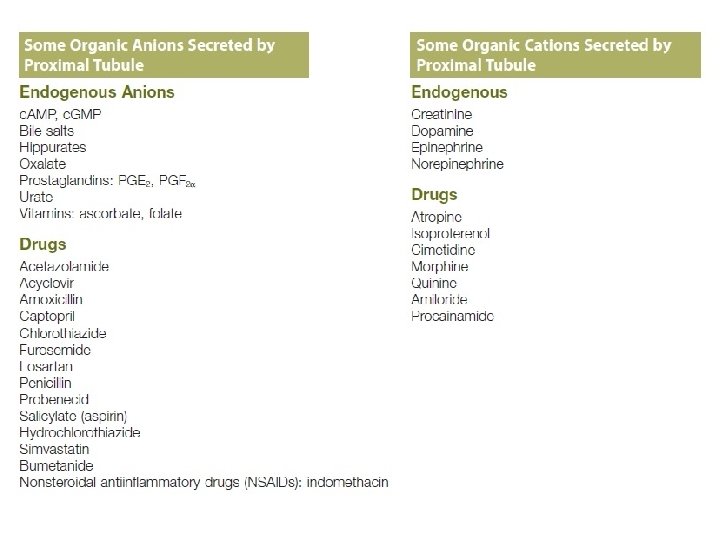
Tubular secretion: In the Proximal Tubule 1. Organic anions - are conjugate bases of organic acids. Many of these organic compounds are bound to plasma proteins and thus are not readily filtered. Examples of organic anions actively secreted in the proximal tubule include penicillin and Para Aminohippuric Acid (PAH). 2. Organic cations - Entry of these cations into the cell across the basolateral membrane is favored by the inside negative membrane potential and occurs via facilitated diffusion, mediated by an organic cation transporter. The exit of organic cations across the luminal membrane is accomplished by an organic cation/H+ exchanger. In addition to being actively secreted, some lipid-soluble non-ionized organic compounds passively diffuse across the tubular epithelium down concentration gradients (example; the ammonia NH 3).

Tubular secretion: In the Cortical Collecting Duct 1. Under normal circumstances, the cortical collecting ducts secrete most of the excreted K+. Whereas, with severe K+ depletion, the cortical collecting duct reabsorb K+. 2. K+ secretion appears to be the function of the collecting duct principal cells. This mechanism is highly dependent on sodium reabsorption by the principal cells (Aldosterone effect). 3. Increased amounts of Na+ in the collecting duct lumen (e. g. , as a result of inhibition of Na+ reabsorption by a loop diuretic drug) result in increased entry of Na+ into principal cells, increased activity of the Na+/K+-ATPase, and increased K+ secretion.

Test Question: Q. In a suicide attempt, a nurse took an overdose of the sedative phenobarbital. This substance is a weak, lipid-soluble organic acid that is reabsorbed by nonionic diffusion in the kidneys. Which of the following would be the best way to promote urinary excretion of this substance? A. Abstain from all fluids B. Acidify the urine by ingesting NH 4 Cl tablets C. Administer a drug that inhibits tubular secretion of organic anions D. Alkalinize the urine by infusing a Na. HCO 3 solution intravenously. E. Increase the GFR
- Slides: 20