Mechanics of respiration Dr Kalpana B Specific Learning

Mechanics of respiration Dr. Kalpana B

Specific Learning objectives • At the end of class students should be able to 1. List the muscles of inspiration and expiration 2. Explain the mechanism of action of muscles of respiration 3. Explain the volume and pressure changes during respiration 4. Explain the physiological significance of respiratory pressures.

5. Explain with a spirogram various static lung volumes and capacities 6. Define vital capacity. List the factors affecting it 7. List the functions of surfactant

The Respiratory System The Mechanics of Breathing GCSE PE Mechanics of Breathing
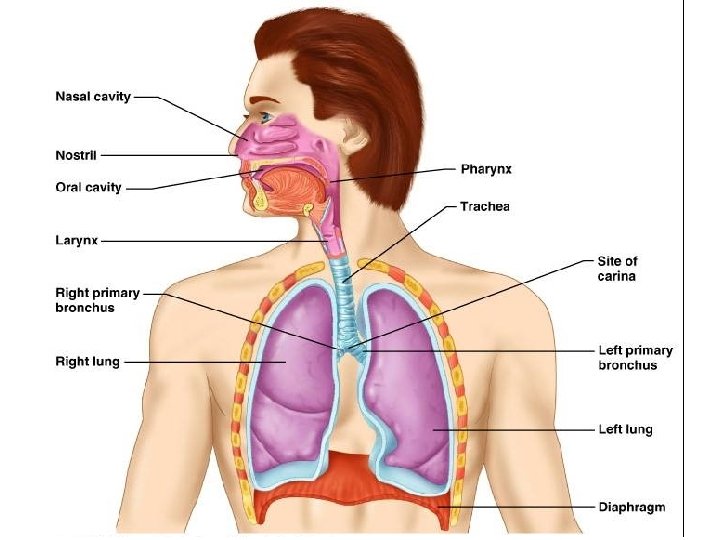

VENTILATION o Breathing in – inspiration / inhalation o Breathing out – expiration / exhalation

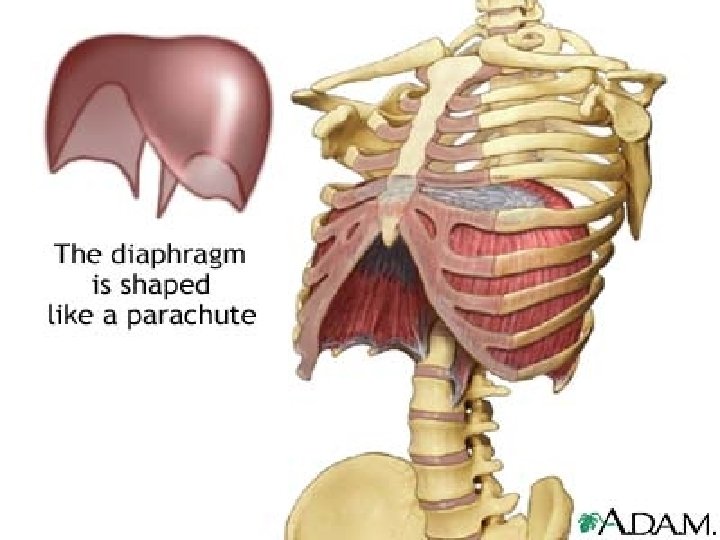
MUSCLES OF INSPIRATION § Diaphragm - increases the vertical diameter of chest wall § External intercostals - increase the transverse and A-P diameters of chest wall

ACCESSORY MUSCLES OF INSPIRATION ü Sternocleidomastoid ü Scaleni ü Pectoralis minor ( Work during forced inspiration, exercise, airway obstruction)

• Expiration is passive at rest, results from elastic recoil of chest wall and lung • But uses internal intercostals and abdominal muscles during forced expiration. • Breathing rate is 10 -20 breaths / minute at rest, 40 - 45 at maximum exercise in adults

External intercostal muscle

EXPIRATION v Passive process v Results from elastic recoil of chest wall and lungs

MUSCLES OF FORCED EXPIRATION Ø Abdominal recti, transversus abdominis, obliques. Ø Internal intercostals

Internal intercostal muscle Abdominals

Movement of the Diaphragm Figure 17 -9 b

Pressures That Cause the Movement of Air In and Out of the Lungs (Pressure changes during ventilation)

Pleural Cavity Very small space Maintained at negative pressure Transmits pressure changes Allows lung and ribs to slide Lungs Gas Exchange Chest Wall (muscle, ribs) Pleural Cavity Diaphragm (muscle) Imaginary Space between Lungs and chest wall 17

Pressure Relationships in the Thoracic Cavity • Respiratory pressure is always described relative to atmospheric pressure • Atmospheric pressure (Patm) - pressure exerted by the air surrounding the body

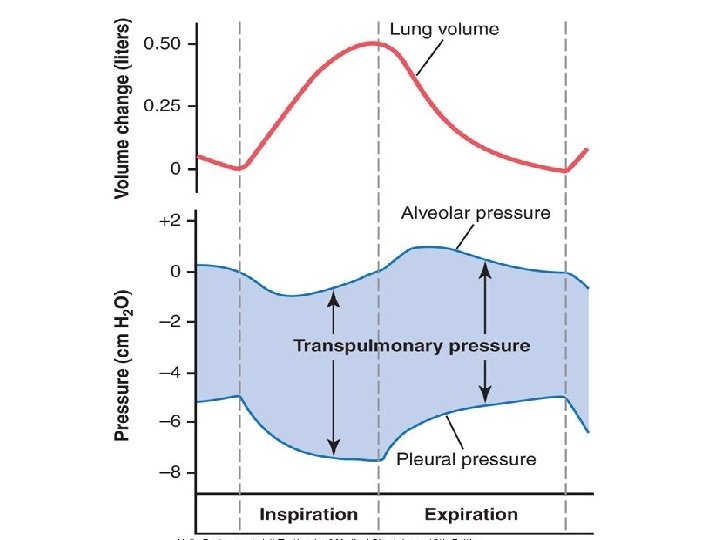
Intra pulmonary pressure/ alveolar pressure: pressure in the alveolus Expiration +1 mm Hg Inspiration -1 mm Hg Intrapleural pressure in the pleural space Expiration -2. 5 Inspiration -6 mm Hg Transmural pressure: pressure difference across the lung

Injury to the Chest Wall • Pneumothorax: – allows air into pleural cavity • Atelectasis: – also called a collapsed lung – result of pneumothorax

Pressure in the Pleural Cavity Pneumothorax results in collapsed lung that can not function normally Figure 17 -12 b

Inspiration • Contraction of diaphragm • Expansion of thoracic cage • Intrapleural pressure becomes more negative (2. 5 to -6 mm Hg) • Increased transpulmonary pressure • Inflation of lung • Decreased alveolar pressure which becomes sub atmospheric (-1 mm Hg) • Airflows into airway and lungs • Cessation of contraction of inspiratory muscles ends inspiration

Expiration • Relaxation of inspiratory muscles • Dropping of rib cage • Intrapleural ressure becomes less negative (6 mm Hg to -2. 5 mm Hg) • Decrease transpulmonary pressure • Deflation of lung • Increased alveolar pressure which becomes more than atmospheric pressure (to +1 mm Hg) • Airflows pushed out of lungs • Expiration continues till alveolar pressure equals atmospheric pressure.

Alveolar surface tension - the force that pulls the surface molecules together of a liquid at a air liquid interface is called surface tension.

Type II

SURFACE TENSION AIR LIQUID

WHAT PREVENTS ALVEOLI FROM COLLAPSING?

Type I cell Type II cell

Surfactant ü Dipalmitoyl phosphatidylcholine ü Secreted by type II pneumocytes ü Present in the alveolar fluid

Functions of surfactant • • • Prevents lung collapse Promotes alveolar stability Helps prevent edema in lungs Decreases work of breathing Promote phagocytosis of bacteria and viruses by alveolar macophage.
 • Deficiency")
Respiratory distress syndrome • Occurs in premature infants(born before 7 completed months) • Deficiency of surfactant • Alveoli collapse after the first breath • Baby goes to severe respiratory distress

WORK OF BREATHING • Under resting conditions, the respiratory muscles normally perform work to cause inspiration but not to cause expiration. • The work of inspiration can be divided into three fractions: (1) Elastic work (65%) (2) Tissue resistance work (7%) (3) Airway resistance work (28%).

PULMONARY FUNCTION TESTS

Specific Learning objectives • At the end of class students should be able to: 1. Explain a spirogram and various static and dynamic lung volumes and capacities 2. Explain FRC alongwith experiments to measure it 3. Differentiate between obstructive and restrictive lung diseases

FPulmonary function tests are useful in assessing the functional status of the respiratory system both in physiological and pathological conditions
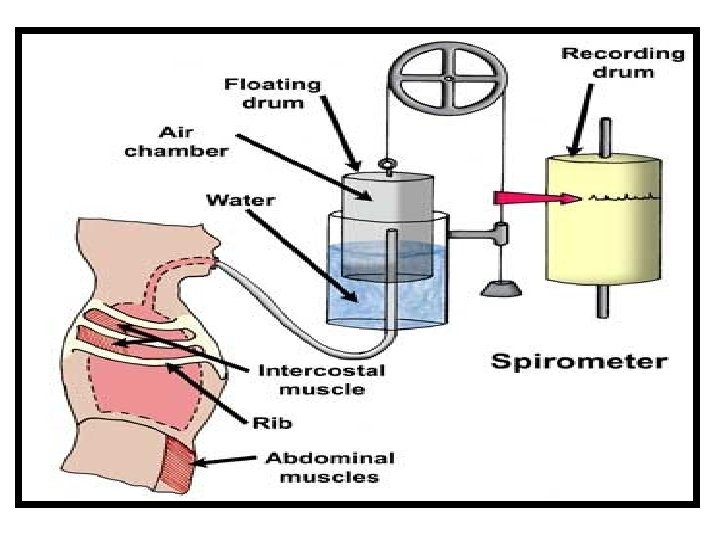
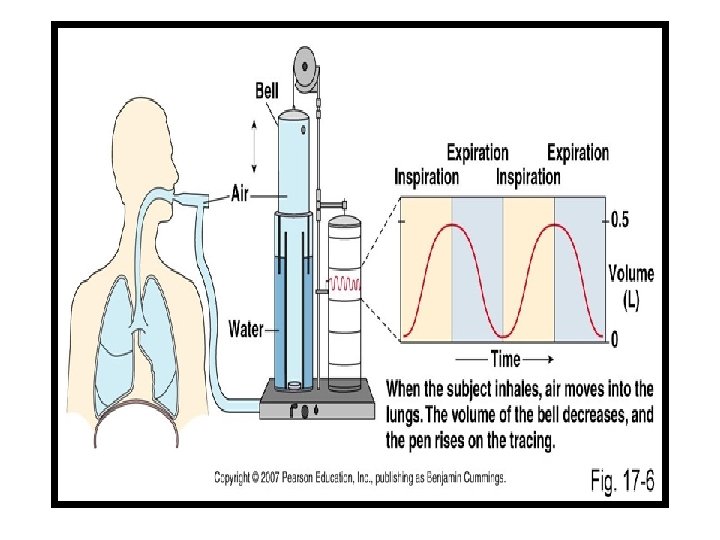

FSpirometer can be used only for single breath FRepeated cycles of respiration cannot be recorded
 Inspiratory reserve volume (IRV) Expiratory reserve volume (ERV) Residual")
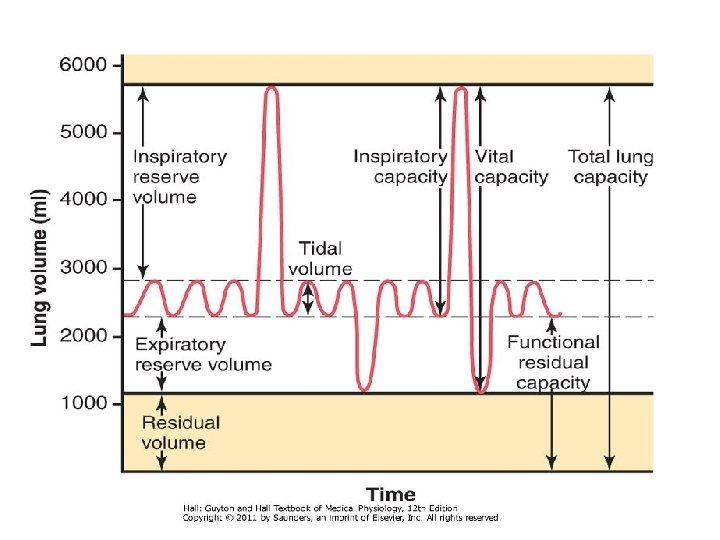
Lung Volumes Tidal volume (TV) Inspiratory reserve volume (IRV) Expiratory reserve volume (ERV) Residual volume (RV)
 – 500 ml Volume of air breathed in or out")
Tidal volume (TV) – 500 ml Volume of air breathed in or out of the lungs in a single normal quiet respiration. Inspiratory reserve volume (IRV) – 3300 ml It is the maximal volume of air which can be inspired after completing a normal tidal inspiration Expiratory reserve volume (ERV) – 1000 ml It is the maximal volume of air which an be expired after a normal tidal expiration
 – 1200 ml It is the volume of the gas")
Residual volume (RV) – 1200 ml It is the volume of the gas which remains in the lungs after maximal expiration 1. It helps to aerate the blood in between breathing and during expiration 2. It maintains the contour of lungs
 =IRV + TV =3800 ml It is the maximum")
Lung Capacities Inspiratory capacity (IC) =IRV + TV =3800 ml It is the maximum volume of air that is inspired from the end expiratory position Expiratory capacity (EC) =ERV + TV =1500 ml It is the maximum volume of air that is expired from the end inspiratory position Functional residual capacity (FRC) or Functional residual volume (FRV) RV + ERV = 2200 ml It is the normal amount of air present in the lungs after normal expiration
 = IRV + TV + ERV =4800 ml It is")
Vital capacity (VC) = IRV + TV + ERV =4800 ml It is the maximum amount of air that is expelled out forcefully after a maximal (deep ) inspiration Total lung capacity (TLC) IRV + TV + ERV + RV = 6000 ml (6 liters) The amount of air present in the lungs after maximal deep inspiration

Variations All lung volumes & Capacities Varies depend upon sex, size & body build of the individual It increases proportionate to size About 20 to 25% less in female than male More in athletic & large persons

Limitation of spirometry Øthe volume which cannot be measured by spirometry are– ØResidual volume (as it cannot expired out) ØSo, also, FRC & TLC (as these include RV)
 or Forced Vital Capacity in unit time (FVC) or Forced")
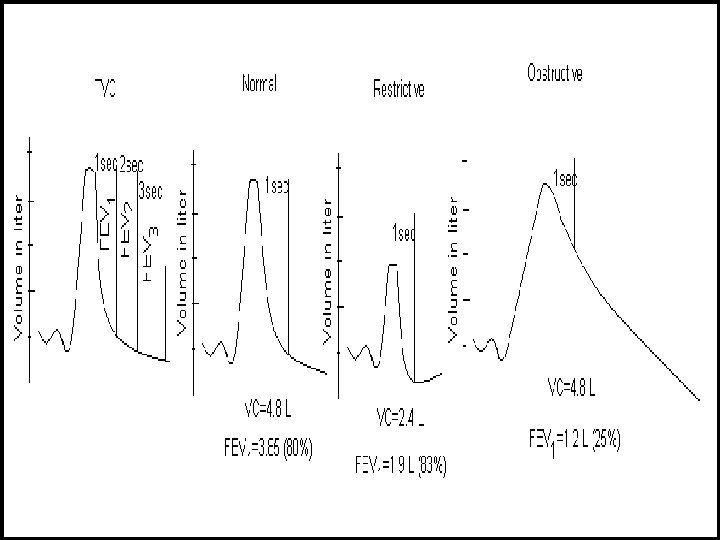
Timed Vital Capacity (TVC) or Forced Vital Capacity in unit time (FVC) or Forced expiratory volumes (FEV) vital capacity measured at each unit time (second). Accordingly, volume expired each unit time is measured and expressed as % of TVC

The amount of air which can expired in given unit time is called forced expiratory volume FEV 1 – 80 to 85% (1 st second) FEV 2 – 90 to 95% (2 nd second) FEV 3 -- >97% (3 rd second) After 3 rd second = 100% of total vital capacity

n Helps to differentiate Restrictive with Obstructive type of respiratory diseases.
 The amount of air moved in and out of the")
Respiratory minute volume (RMV) The amount of air moved in and out of the lungs every minute TV X RR = RMV 500 X 12 = 6000 ml (6 litres)
 or Maximum Breathing capacity (MBC) The maximum amount of air")
Maximum Voluntary Ventilation (MVV) or Maximum Breathing capacity (MBC) The maximum amount of air which can be breathed in and out of the lungs by means of forceful respiration (hyperventilation) per minute

§ Normal value: In healthy adult male it is 150 -170 litres/min and in females it is 80 – 100 litres/min
 rate Ø The maximum rate at which the air")
PEFR (Peak expiratory flow rate) rate Ø The maximum rate at which the air an expired after deep inspiration Ø >400 L/min (respiratory Muscle endurance) ØUseful for assessing the respiratory diseases especially to differentiate the obstructive and restrictive diseases.

Compliance • Compliance is the measure of stretchability or elasticity or distensibility • Compliance is change in volume by unit change in pressure (∆V/∆P) : ml/cm H 2 O (L/cm H 2 O)

Types of compliances • As both lungs & thoracic cage has elastic nature –in the respiratory system the various compliances are; • Lung compliance (L. C) • Thoracic compliance (Th. C) • Total compliance (T. C) -- (both L. C & Th. C)

Normal value Compliance in relation to intrapleural pressure Compliance of lungs and thorax • 130 ml / 1 cm H 2 O pressure Compliance of lungs alone • 220 ml / 1 cm H 2 O pressure • compliance of lung alone is 2 times compliance of lung and thorax

• This is because , inside thorax, some energy is required to expand the thorax • lung can be distended such an extent due to • presence of large number of elastic fibers • And the peculiar arrangement of elastic fibers.

• Specific compliance – It is the compliance per unit volume • Compliance/FRC (in L per cm H 2 O per L)

Hysteresis loop

• P-V relationship is curved • At identical Ppl volume is less in I phase than in E phase. • Difference in distensibility of the lungs between I and E phase. • Viscous resistance • Airway resistance

Measurement of compliance Lung Compliance measured in static condition • Measured by inspiring a series of known volume of air and simultaneously recording the intrapleural pressure of each. • The air is expired in steps till the volume returns to the original prerespiratory level

Dead Space The part of the respiratory tract where the gaseous exchange does not take place Function – Purification, Humidification & Airconditioning Types – 2 üAnatomical dead space volume– volume Volume of gas in respiratory tract ( nose - terminal bronchiole). üNormal value – 150 ml üPhysiological dead space volume - Total dead space volume Anatomical DSV + Volume of air in the alveoli which does not take part in the exchange of gas Normal healthy person – Physiological DSV = Anatomical DSV

Alveolar ventilation It indicates the volume of air which is utilized for gaseous exchange every minute (TV – DSV) X RR (500 – 150) x 12 = 4, 200 ml/min

Ventilation-Perfusion ratio • • Ratio of alveolar ventilation and the amount of the blood that perfuses the alveoli Rate of alveolar ventilation (VA) – 4 liters/min Rate of alveolar perfusion (Q) =5 liters The ventilation-perfusion ratio = VA/Q = 4/5 = 0. 8 Important to maintain the alveolar PO 2 & PCO 2

Normal variation in VA/Q ratio n. Normal individual, in upright posture— VA/Q ratio variation from Top to Bottom of lungs is –from 3 at top to 0. 6 at bottom n. Reasons – 1) Effect of gravity 2) Variation in intra-pleural pressure

• Apex of lung ventilation is greater than perfusion. • Base perfusion is greater than apex.

Physiological importance • So more PAO 2. Thus tuberculosis is more common in apex because of favorable environment for mycobacterium tuberculosis.

Pathalogical importance • Decreased VA/Q: bronchial obstruction • Increased VA/Q: vascular obstruction.

Sequence of events in lungs • Hb –oxygenated forming oxyhaemoglobin-mobilize chloride shift in the reverse order. • Chloride of KCl comes out of cell reacts with Na. HCO 3 in plasma forming Na. Cl and liberating HCO 3. • HCO 3 released from KHCO 3 joins with H+ • To form H 2 Co 3 which splits into water and carbon-dioxide which diffuses into plasma and then through alveoli.

References • Text book of medical physiology A P Krishna • Essentials of medical physiology (6 th edition) K Sembulingam and Prema Sembulingam AEJ 73
- Slides: 73