MECHANICAL VENTILATION Seyed Alireza Mahdavi Ventilator settings Ventilator







 What is PEEP? What is the goal of PEEP? l")









 l Low")
 l Applicable")






- Slides: 28
MECHANICAL VENTILATION Seyed Alireza Mahdavi
Ventilator settings
Ventilator settings 1. 2. 3. 4. 5. 6. 7. 8. Ventilator mode Respiratory rate Tidal volume or pressure settings Inspiratory flow I: E ratio PEEP Fi. O 2 Inspiratory trigger
CMV
A/CV
SIMV
Concepts and Modes of Mechanical Ventilation Bivent Pressure SIMV Pressure CMV Mechanical Ventilation Time CPAP Pressure APRV Pressure Time Spontaneous Breathing
Positive End-expiratory Pressure (PEEP) What is PEEP? What is the goal of PEEP? l Improve oxygenation l Diminish the work of breathing l Different potential effects
PEEP What are the secondary effects of PEEP? l l l Barotrauma Diminish cardiac output Regional hypoperfusion Na. Cl retention Augmentation of I. C. P. ? Paradoxal hypoxemia
Monitoring of the patient
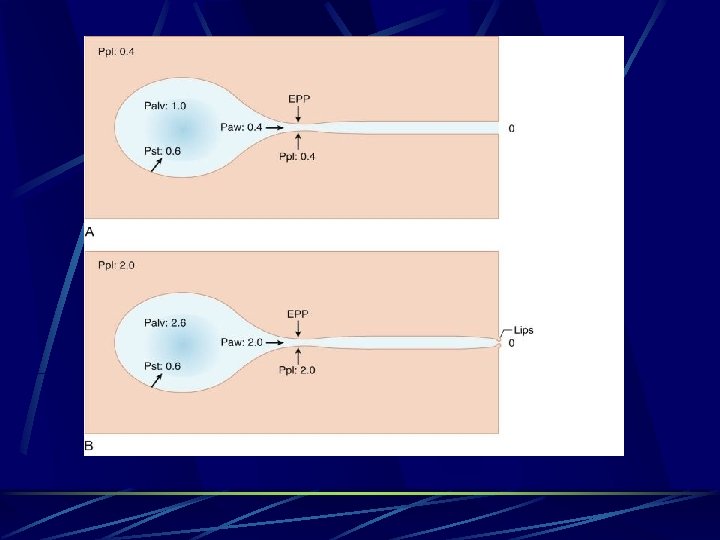
Auto-PEEP or Intrinsic PEEP What is Auto-PEEP? l Normally, at end expiration, the lung volume is equal to the FRC l When PEEPi occurs, the lung volume at end expiration is greater than the FRC
Auto-PEEP or Intrinsic PEEP Why does hyperinflation occur? Airflow limitation because of dynamic collapse l No time to expire all the lung volume (high RR or Vt) l Expiratory muscle activity l Lesions that increase expiratory resistance l
Auto-PEEP or Intrinsic PEEP Auto-PEEP is measured in a relaxed pt with an end-expiratory hold maneuver on a mechanical ventilator immediately before the onset of the next breath
Auto-PEEP or Intrinsic PEEP Adverse effects: l l l Predisposes to barotrauma Predisposes hemodynamic compromises Diminishes the efficiency of the force generated by respiratory muscles Augments the work of breathing Augments the effort to trigger the ventilator
Different types of patient
COPD and Asthma Goals: l Diminish dynamic hyperinflation l Diminish work of breathing l Controlled hypoventilation (permissive hypercapnia)
Diminish DHI Why?
Diminish DHI How? l Diminish minute ventilation Low Vt (6 -8 cc/kg) l Low RR (8 -10 b/min) l Maximize expiratory time l
Diminish work of breathing How: l Add PEEP (about 85% of PEEPi) l Applicable in COPD and Asthma.
Controlled hypercapnia Why? l Limit high airway pressures and thus diminish the risk of complications
Controlled hypercapnia How? l Control the ventilation to keep adequate pressures up to a PH > 7. 20 and/or a Pa. CO 2 of 80 mm. Hg
Controlled hypercapnia CI: Head pathologies l Severe HTN l Severe metabolic acidosis l Hypovolemia l Severe refractory hypoxia l Severe pulmonary HTN l Coronary disease l
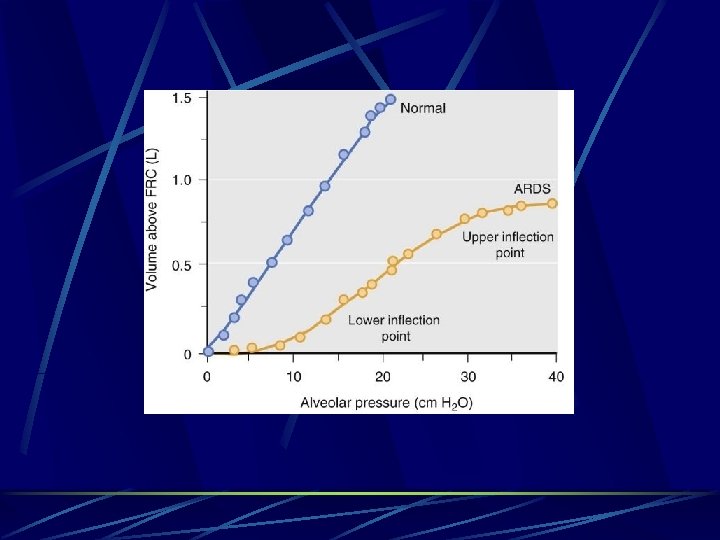
Restrictive Pattern Intrapulmonary: Intra-alveolar filling processes Alterations in lung interstitium Extrapulmonary Pleural disease Chest wall abnormalities Neuromuscular disease
Management of Mechanical Ventilation Volume Pressure I: E ratio Mode
Thank You