MEASURING BLOOD PRESSURE Blood pressure is indicates your

MEASURING BLOOD PRESSURE Blood pressure is indicates your heart health It is determined by the contractions of the heart Your pressure varies depending on the condition of your heart and blood vessels Pressure is measured in millimeters of mercury (mm Hg)

WHAT IS BLOOD PRESSURE Blood pressure is the force that blood exerts against blood vessel walls. The pumping action of the heart generates the flow Pressure occurs when the flow is met by resistance from blood vessel walls

BLOOD PRESSURE GRAPH Pulse Pressure Systolic By Dicrotic Notch Diastolic Average Pressure taking your pulse, you can feel that blood pressure fluctuation with each heartbeat. The pulse which you feel is actually a pressure wave that travels from your heart though your arteries

SYSTOLIC PRESSURE Systolic pressure is the maximum pressure exerted by the blood against the artery walls. It results when the ventricles contract. Normally, it measures 120 mm Hg. Systolic

DICROTIC NOTCH The Dicrotic Notch represents the interruption of blood flow due to the brief backflow of blood that closes the aortic semilunar valve when the ventricles relax. Dicrotic Notch

DIASTOLIC PRESSURE Diastolic Pressure is the lowest pressure in the artery. It result when the ventricles are relaxed and is usually around 80 mm Hg. Diastolic

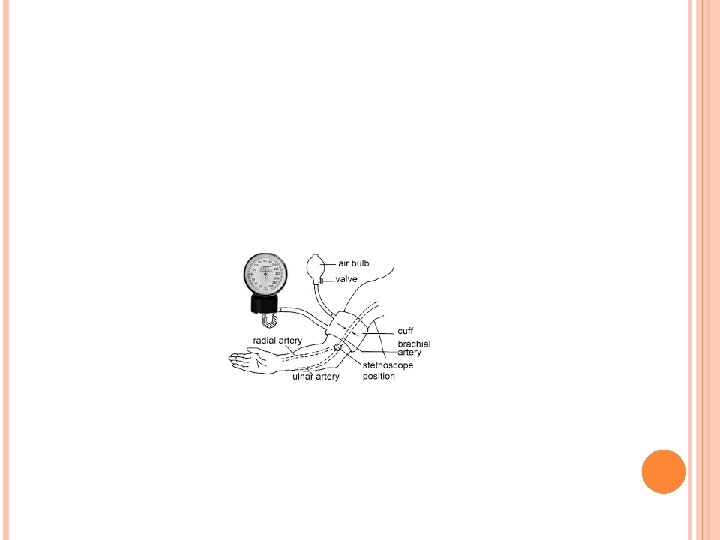
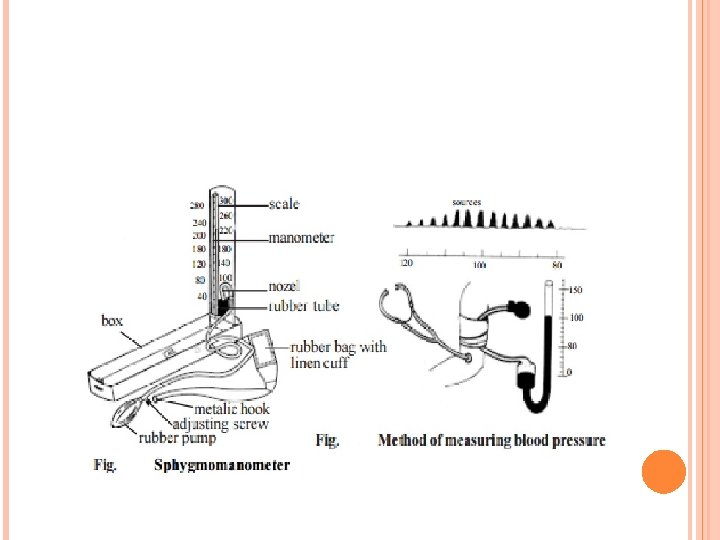
MEASUREMENT DEVICE Aneroid sphygmomanometer Simple mercury sphygmomanometer Automated bp device

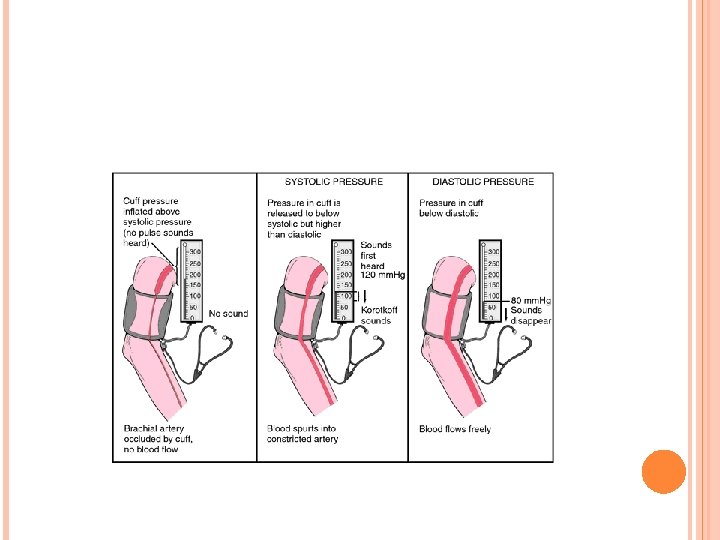
BLOOD PRESSURE SOUNDS A cuff is inflated to constrict an artery so that no blood flows. As the cuff pressure is slowly released, but the artery is still partially constricted, blood flow begins again. Sounds can be heard because the blood flows violently causing audible sounds. When the artery is fully open, the blood flows freely and the sounds disappear.
.")
CHECKING BLOOD PRESSURE The first sounds that are heard indicate systolic pressure (top number). When the sounds stop, diastolic pressure has been reached (bottom number). Average blood pressure is: 120 80

THE ‘SILENT KILLER’ Causes death from: Strokes Heart Attacks Peripheral Vascular Disease If untreated, leads to: Renal failure, heart failure
 Grade 2 (moderate)")
BLOOD PRESSURE CLASSIFICATION Category Optimal High normal BP Grade 1 (mild) Grade 2 (moderate) Grade 3 (severe) ISH (Grade 1) ISH (Grade 2) Systolic BP Diastolic BP <120 <80 <130 130 -139 140 -150 160 -179 ≥ 180 140 -159 <85 85 -89 90 -99 100 -109 ≥ 110 <90 ≥ 160 <90

THRESHOLDS FOR INTERVENTION BP ≥ 220/120 mm. Hg: treat immediately BP >180 -189/110/119 mm. Hg: confirm over 1 -2 weeks, then treat BP 160 -179/100 -109 mm. Hg: with CVD complications: confirm over 3 -4 weeks, then treat BP 140 -159/90 -99 mm. Hg: with CVD risk confirm over 12 weeks, then treat.

BLOOD PRESSURE MEASUREMENT SOURCES OF ERROR Errors due to manometer Errors due to cuff Errors due to the observer Errors due to the patient.

BP MEASUREMENT Three or more readings, separated by 1 minute Discard first reading and average last two If large difference take further readings.

BP MEASUREMENT -CUFFS Cuff too small or too big Normal Cuff cuff too small for 15% of patients not level with the heart Leaky rubber tubing or bladder* Faulty inflation/deflation device* * Applies to mercury manometers only.

BLOOD PRESSURE ASSESSMENT: PATIENT PREPARATION AND POSTURE Standardized Preparation: Patient 1. No acute anxiety, stress or pain. 2. No caffeine, smoking or nicotine in the preceding 30 minutes. 3. No use of substances containing adrenergic stimulants such as phenylephrine or pseudoephedrine (may be present in nasal decongestants or ophthalmic drops). 4. Bladder and bowel comfortable. 5. No tight clothing on arm or forearm. 6. Quiet room with comfortable temperature 7. Rest for at least 5 minutes before measurement 8. Patient should stay silent prior and during the procedure.

BLOOD PRESSURE ASSESSMENT: PATIENT PREPARATION AND POSTURE Standardized technique: Posture The patient should be calmly seated with his or her back well supported and arm supported at the level of the heart. His or her feet should touch the floor and legs should not be crossed.

BLOOD PRESSURE ASSESSMENT: PATIENT POSITION X

RECOMMENDED EQUIPMENT FOR MEASURING BLOOD PRESSURE Use a mercury manometer or a recently calibrated aneroid or a validated automated device. Aneroid devices should only be used if there is an established calibration check every 12 months.

RECOMMENDED EQUIPMENT FOR MEASURING BLOOD PRESSURE Automated oscillometric devices: Use a validated automated device according to BHS, AAMI or IP clinical protocols. For home blood pressure measurement devices, a logo on the packaging ensures that this type of device and model meets the international standards for accurate blood pressure measurement. AAMI=Association for the Advancement of Medical Instrumentation; BHS=British Hypertension Society; IP: International Protocol.
 Select a device with an appropriate")
RECOMMENDED TECHNIQUE FOR MEASURING BLOOD PRESSURE (CONT. ) Select a device with an appropriate size cuff
 Size of Cuff (cm) From 18")
USE AN APPROPRIATE SIZE CUFF Arm circumference (cm) Size of Cuff (cm) From 18 to 26 9 x 18 (child) From 26 to 33 12 x 23 (standard adult model) From 33 to 41 15 x 33 (large) More than 41 18 x 36 (extra large, obese) For automated devices, follow the manufacturer’s directions. For manual readings using a stethoscope and sphygmomanometer, use the table as a guide.
 Locate the brachial pulse and centre")
RECOMMENDED TECHNIQUE FOR MEASURING BLOOD PRESSURE (CONT. ) Locate the brachial pulse and centre the cuff bladder over it Position cuff at the heart level Arm should be supported
 To exclude possibility of auscultatory gap,")
RECOMMENDED TECHNIQUE FOR MEASURING BLOOD PRESSURE* (CONT. ) To exclude possibility of auscultatory gap, increase cuff pressure rapidly to 30 mm. Hg above level of disappearance of radial pulse Place stethoscope over the brachial artery *with manual or semi automated devices
 Drop pressure by 2 mm. Hg")
RECOMMENDED TECHNIQUE FOR MEASURING BLOOD PRESSURE* (CONT. ) Drop pressure by 2 mm. Hg / beat � Appearance of sound (phase I Korotkoff) = systolic pressure Drop pressure by 2 mm. Hg / beat � Disappearance of sound (phase V Korotkoff) = diastolic pressure Record measurement Take at least 2 blood pressure measurements, 1 minute apart *with manual or semi automated devices

KOROTKOFF SOUNDS AND AUSCULTATORY GAPS Korotkoff sounds 200 180 160 No sound Clear sound Phase 1 Muffling 140 No sound Phase 2 Auscultatory gap 120 Clear sound Phase 3 100 Muffled sound Phase 4 No sound Phase 5 80 60 40 20 0 mm. Hg Systolic BP Phase 3 Phase 4 Diastolic BP

BP MEASUREMENT - OBSERVER Mercury column not level with the eyes Failure to hear the Korotkoff sounds Wrong diastolic endpoint (K 4 or K 5) Subjective detection of Korotkoff sounds Rapid cuff deflation Single one off reading.
 Place gently over")
STETHOSCOPE Good quality Short tubing Well fitting ear pieces (cleaned regularly) Place gently over the brachial artery Avoid touching the cuff and tubing.
 and")
POSTURE Routine - seated Standing in patients with symptoms or diabetic (diabetic nephropathy) and the elderly Supine position unnecessary, inconvenient and cuff position often below the heart.

EXPLANATION TO THE PATIENT Tell the patient their blood pressure reading Write BP down – use co-operation cards Give relevant leaflets/booklets on life style issues (not too many at a time) Reassure patient that this is a risk factor not a disease (unless left untreated) Do not lose to follow-up.

‘WHITE COAT’ HYPERTENSION Effective method of diagnosing a rise in blood pressure associated with having blood pressure measured Maybe from anxiety 10 -20% of subjects labelled ‘hypertensive’ may have ‘white coat’ effect.
- INDICATIONS Borderline hypertension White coat hypertension Isolated systolic hypertension")
AMBULATORY BLOOD PRESSURE MEASUREMENT (ABPM)- INDICATIONS Borderline hypertension White coat hypertension Isolated systolic hypertension Nocturnal blood pressure Resistant hypertension Hypotensive symptoms.

HOME MONITORING Gives patients empowerment May improve medication concordance Device used must be validated Multiple day time recordings, over 7 days (eliminating ‘white coat’ effect) with BP taken in the morning and evening First 24 hour readings should be discarded Home measurements usually lower than clinic readings.

CONCLUSIONS Traditionally � Protocol can be standardized � Requires Extensive training Passed audiogram for the measurers Automated � Problems devices often used with the comparability between devices and in time trends HES Workshop, Luxembourg, 9 -11 April 2008 mercury sphygmomanometers are recommended
- Slides: 38