MCB 135 K Discussion April 20 2005 Topics

MCB 135 K Discussion April 20, 2005

Topics • Adaptation to Stress • Hypothalamo-Pituitary-Thyroid Axis • Carbohydrate Metabolism, Diabetes, and Aging

Beneficial effects of Hormesis may be due to: DNA repair Immune competence Neurologic acuity Neuromuscular activity Better memory Resistance/ adaptation to stress

Several lines of investigations have shown that manipulation of the genome will result in changes of the phenome. These changes involve alteration of the endocrine signaling with a shift From • High energy consumption • Active growth & development • Active reproductive function To • Reduce energy consumption • Arrest of growth, development, reproductive function • High resistance to stress

Shift in HPA secretory priorities during stress

Suppressing signaling from hormones such as: insulin, growth hormone, insulin-like growth hormone and others by constructing mutants with lack of the hormone or the hormone receptors can prolong the lifespan as much as six times the lifespan in C. Elegans, delaying the aging process

“I cannot, and should not, be cured of my stress but merely taught to enjoy it” Hans Selye, l 950 Responses to stress are indispensable to our survival as they allow us to maintain the internal equilibrium necessary for optimal function Responses to stress are multifactorial (depend on interactions of several systems)

• If response to stress is severe & prolonged it may represent a major risk for the “diseases of adaptation” (e. g. cardiovascular, cognitive, emotional, metabolic diseases) & shorten the lifespan • If the response to stress is moderate & of short duration, it may stimulate hormesis: – – – the functions of alertness, vigilance & motivation a greater availability & utilization of metabolic energy favor DNA repair improve protein folding (chaperone stimulation) prevent/decrease free radical accumulation promote survival and may delay aging
 Of genes involved in")
ON FLIES, WORMS, RODENTS: LONGEVITY is associated With stimulation (up-regulation) Of genes involved in response to stress including those of HSPs act as chaperones and promote greater tolerance/resistance to stress (thermic and others) Hence, increased longevity and hormesis may depend on Increased HSPs and their actions as chaperones

Table 13. 3 Major Actions of Thyroid Hormones • Calorigenesis • Metabolism • Brain maturation • Behavior • Growth & development
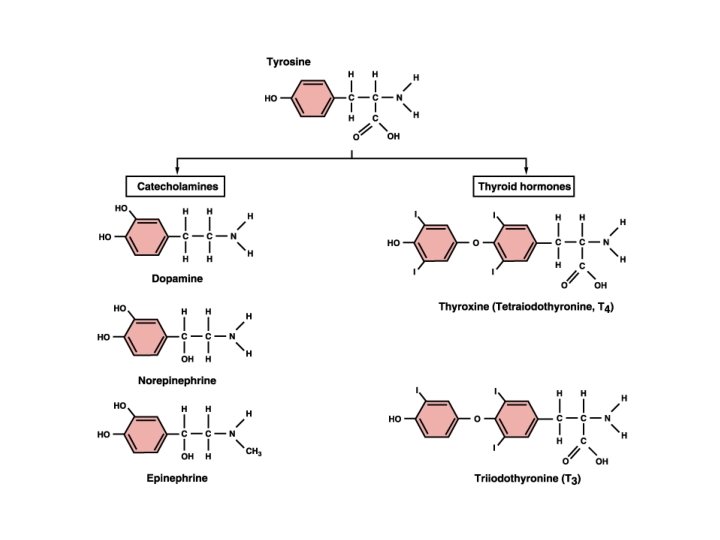
 3, 5, 3’ Triiodothyroine (T 3)")
3, 5, 3’, 5’ Tetraiodothyronine (thyroxine, T 4) 3, 5, 3’ Triiodothyroine (T 3)
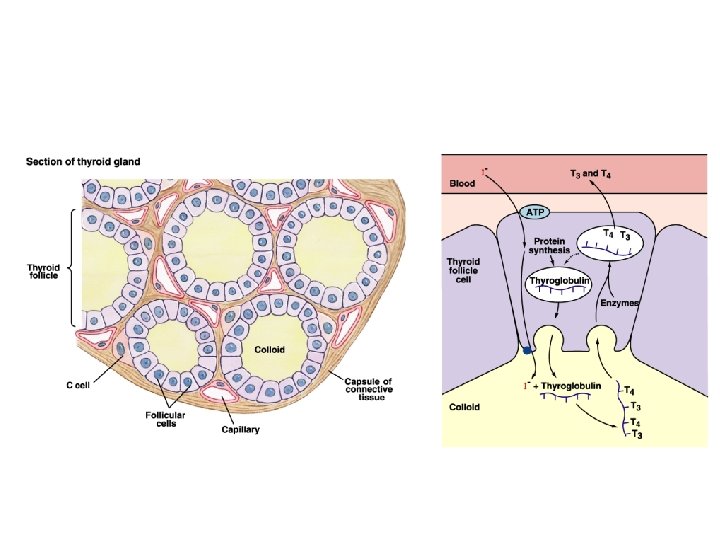

Table 13 -2: Some MORPHOLOGIC Changes in the Thyroid Gland with Aging FOLLICLES: - Are distended - Change in color - Epithelium flattened w/ reduced secretion Fewer mitoses Increased connective tissue; Fibrosis Atherosclerotic changes
: Some SECRETORY Changes in the Thyroid Gland with Aging")
Table 13 -2 (con’t. ): Some SECRETORY Changes in the Thyroid Gland with Aging circulating T 3 levels but generally within the normal (lower) range peripheral conversion of T 4 to T 3 Simultaneously decreased secretion and metabolic clearance of T 4 with resulting essentially normal levels Failure of up-regulation of T 3 nuclear receptors TSH levels in 10% of the elderly, associated in antithyroid antibodies, present even in the absence of manifestations of hypothyroidism

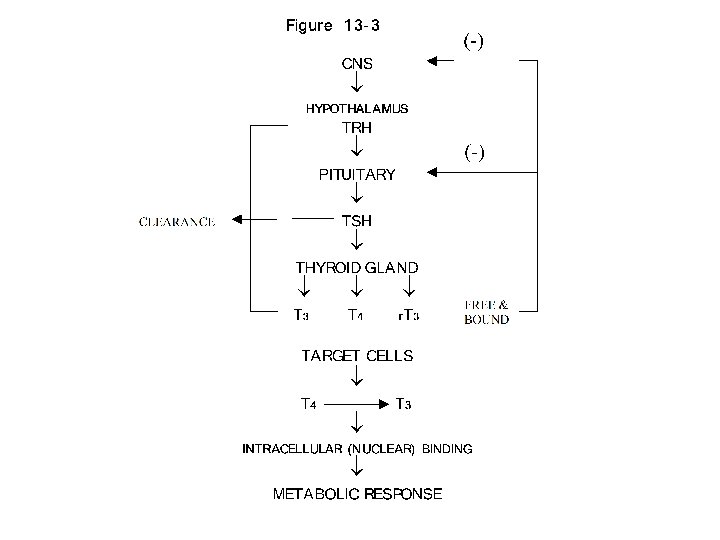
Table 13 -1: Some Critical Aspects of Thyroid Hormone Regulation 1. Major source of circulating T 3 from peripheral deiodination of T 4 (NOT from thyroid gland secretion) 2. The negative feedback at the pituitary anterior lobe is mainly through T 4 (taken from circulation & converted into T 3) 3. The peripheral deiodination of T 4 depends on the physiological state of the organism. It allows an autonomy of response of the tissues to the hormones. 4. Deiodination can convert T 4 (a less biologically active hormone) to T 3 (a more active hormone). This conversion depends on the activity of the various deiodinating enzymes.

Table 13 -6 Autoimmune Diseases of the Thyroid Gland Characteristics Graves’ Disease Hashimoto’s Thyroiditis Thyroid Status Hyperthyroid Hypothyroid TSH Generally undetectable Normal to elevated T 4, T 3 (serum) Above normal Below normal Antibodies(ABs) Stimulatory ABs compete with TSH at receptor sites Loss of TSH control over thyroid function Some ABs block TSH actions Autoantibodies against Generally present thyroglobulin, T 3, T 4, thyroid destroy thyroid microsomal and nuclear components Generally present Lymphocytic Invasion Limited Marked Female: Male Ratio As high as 10: 1

Table 13 -7 Common Signs and Symptoms of Hyperthyroidism in the Elderly Cardiovascular Congestive heart failure Atrial fibrillation Angina (coronary heat disease) Pulmonary edema CNS Tremor Nervousness Weakness Weight loss and anorexia Exothalmos (protrusion of eyeball) THYROID Goiter? Thyroid nodules? **Also, apathetic hyperthyroidism (see page 244)**

Table 13 -8 Frequently Missed Common Signs and Symptoms of Hypothyroidism in Elderly Patients Cardiovascular Dyspnea (shortness of breath) Chest pain Enlarged heart Bradycardia (slow heart beat) MISC. Anorexia and constipation Muscular weakness Mild anemia Depression Cold intolerance Joint pain

With Age: • Incidence of Diabetes Mellitus Type 2 (late onset diabetes, non-insulin dependent diabetes) increases considerably • Diabetes Mellitus Type 2 is the most common form of diabetes • Onset occurs years before symptoms are appreciated – therefore, it is important to screen high risk individuals
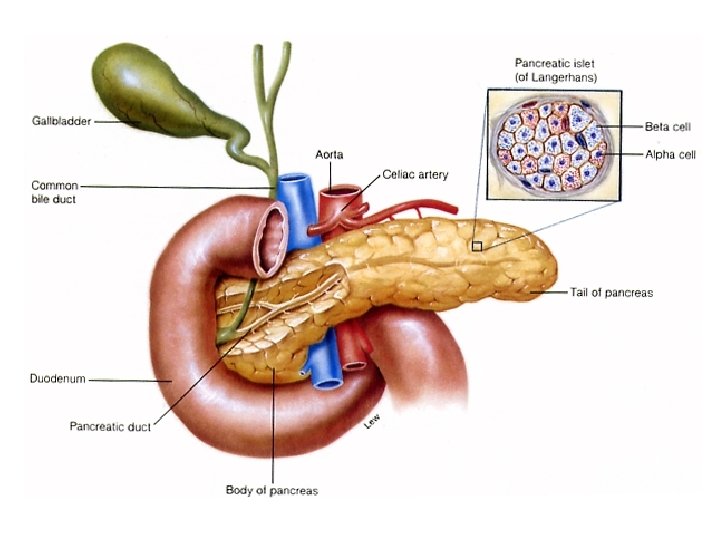

Morphologic Changes • A certain degree of atrophy • An increased incidence of tumors • Presence of amyloid material & lipofuscin granules (signs of abnormal cellular metabolism)

Table 14 -1 Major pancreatic hormones Pancreas B-Cells A-Cells D-Cells F, DDor or. PP PPCells F, Hormone Alternate source Pre-proinsulin Proinsulin Insulin (+ connecting C-peptide) Proglucagon GI mucosa Glucagon(+ glicentin) Somatostatin GI mucosa CNS Pancreatic Polypepetide GImucosa GI

Table 14 -2 Major actions of insulin Glucose transport into muscle & adipose cells blood glucose intracellular metabolic use of glucose glycogen synthesis in liver and muscle cells gluconeogenesis (in liver) intracellular transport of amino acids & lipids & protein and triglyceride synthesis overall body growth (general effect)
, glucose balance is maintained by: Insulin secretion Glucose")
When blood glucose is high (hyperglycemia), glucose balance is maintained by: Insulin secretion Glucose cellular uptake (in muscle) Endogenous production of glucose Utilization of glucose (muscle & adipose cells) Storage of glucose (in liver as glycogen), fat & amino Acids arriving in the blood form GI tract
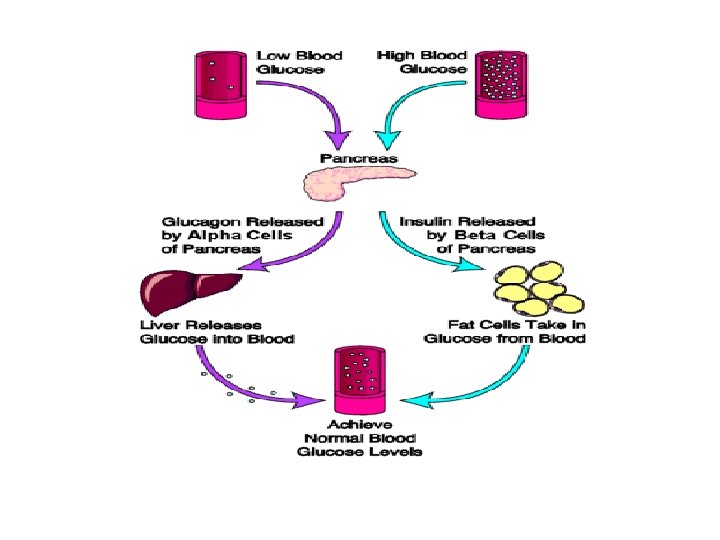
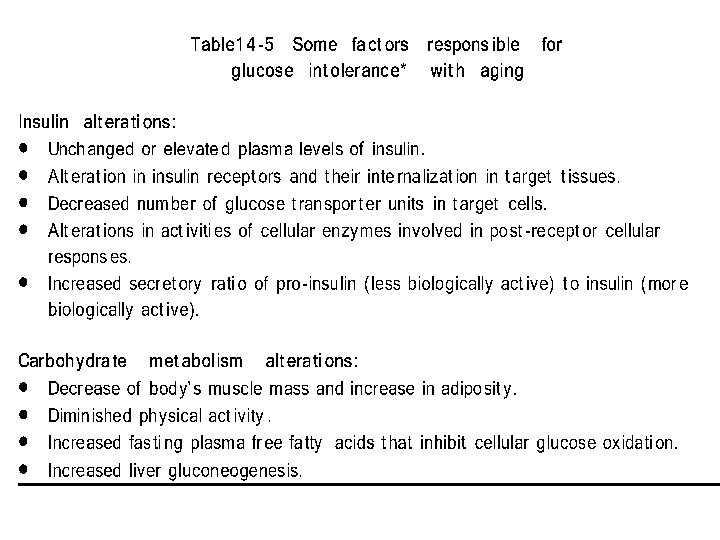

Table 14 -7 Characteristics of Diabetes Mellitus glucose uptake Hyperglycemia glycogenesis hepatogluconeogenesis Glycosuria Polydipsia Polyphagia protein catabolism plasma amino acid gluconeogenesis Weight loss, growth inhibition Negative nitrogen balance lipolysys free fatty acids Ketosis Acidosis Microangiopathies Vascular changes

Table 14 -8 Diabetes and Accelerated Aging DIABETES Microangiopathy Cataracts Neuropathy Accelerated Atherosclerosis Early decreased fibroblast proliferation Autoimmune involvement Skin changes AGING --Cataracts Neuropathy Atherosclerosis Decreased fibroblast proliferation Autoimmune involvement Skin changes
- Slides: 30