Maternal Cardiopulmonary Resuscitation Basic and Advanced Life Support

Maternal Cardiopulmonary Resuscitation: Basic and Advanced Life Support By Dr. nataj Anesthesiologist & ICU fellwoship

AVPU A=Allert V=Verbal P=Painfull U=Unresponse


CARDIOPULMONARY RESUCITATION CPR 2015 GUIDLINE
 date back to 1966, when a")
• contemporary approaches to cardiopulmonary resuscitation (CPR) date back to 1966, when a National Academy of Sciences National Research Council conference generated consensus standards for the performance of CPR. • Since that time, successive conferences have reviewed the practice of CPR in light of available experimental and clinical data and have prepared revisions of previous standards. •

• The most recent recommendations, the 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (2015 AHA Guidelines for CPR and ECC), represent the forth internationally recognized resuscitation guidelines developed by experts from the American Heart Association (AHA) and the European Resuscitation Council (ERC); as such, these guidelines represent a variety of countries, cultures, and medical specialties.

SUDDEN CARDIAC ARREST AND CARDIOPULMONARY RESUSCITATION SCA is a complex and dynamic process. Antegrade systemic arterial blood flow continues after cardiac arrest until the pressure gradient between the aorta and right heart structures reach equilibrium. A similar process occurs during cardiac arrest with antegrade pulmonary blood flow between the pulmonary artery and the left atrium. the arteriovenous pressure gradients dissipate, the left heart becomes less filled, the right heart becomes more filled, and the venous capacitance vessels become increasingly distended. When the arterial and venous pressures equilibrate (approximately 5 minutes after cardiac arrest), coronary perfusion and cerebral blood flow stop.

• During cardiopulmonary arrest, oxygen delivery to maternal tissue and the uterus is dramatically reduced or eliminated completely. • Maternal or fetal adaptations to such severe insult are insufficient to sustain tissue viability. Death begins in minutes

• Cardiopulmonary arrest in pregnancy is very uncommon occurring only one in every 30000 pregnancies. • Even at busiest medical centers, this will only total a few cases per year. • Because it is uncommon, it is difficult to study.

During pregnancy arrest most often occurs in previously healthy woman related to acute events such as pulmonary embolism or hemorrhage.

• Review of the ACLS guidelines reveal three major modifications for the pregnant patient that we will explain in detail: 1)focus on early endotracheal intubation 2)leftward displacement of the uterus during chest compressions 3)consideration of perimortem cesarean delivery whithin 4 minutes of onset of arrest.

Pathophysiological rationale for leftward displacement • Uterine aortocaval compression has tow important clinical consequences during maternal arrest: • 1)it must be temporarily relieved to optimize the effectiveness of CPR. • 2)it provides an opportunity to definitively improve maternal survival, since perimortem delivery can have a profound benefit on maternal hemodynamics.

• In non pregnant patients, chest compression is estimated to produce cardiac output approximately 30% of normal but it is likely that the effectiveness of chest compressions, diminished in pregnancy, by aortocaval compression.
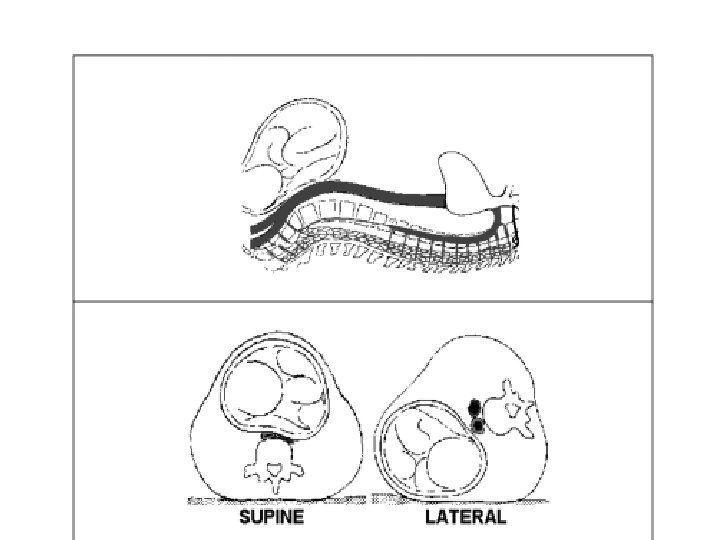
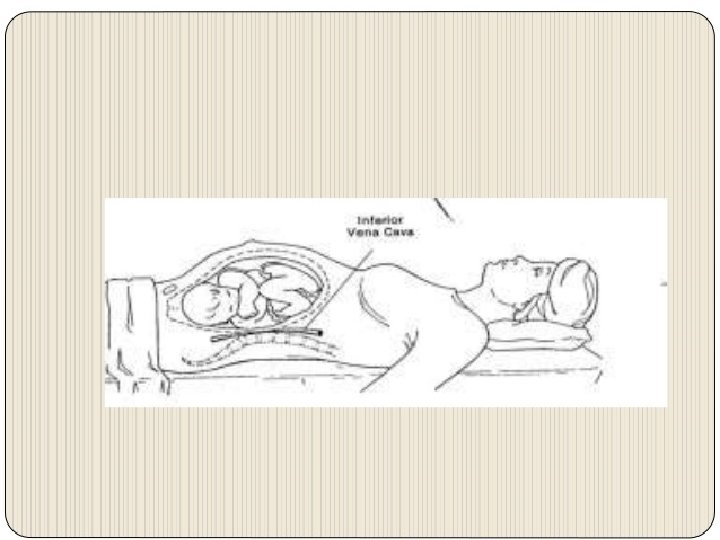

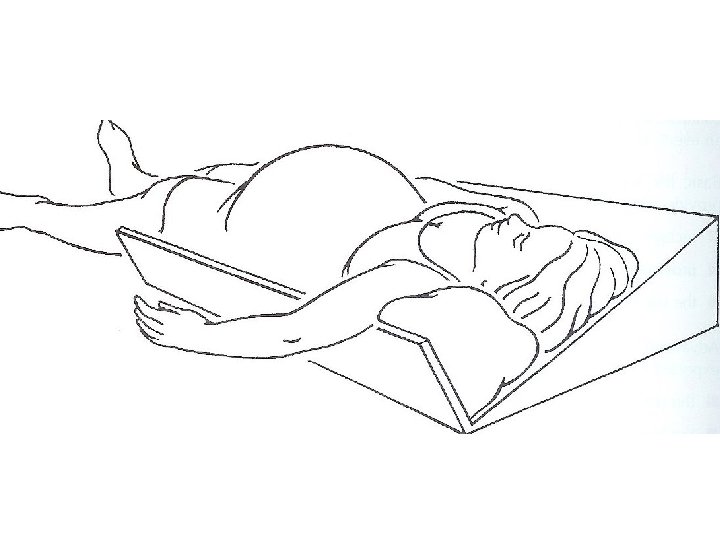
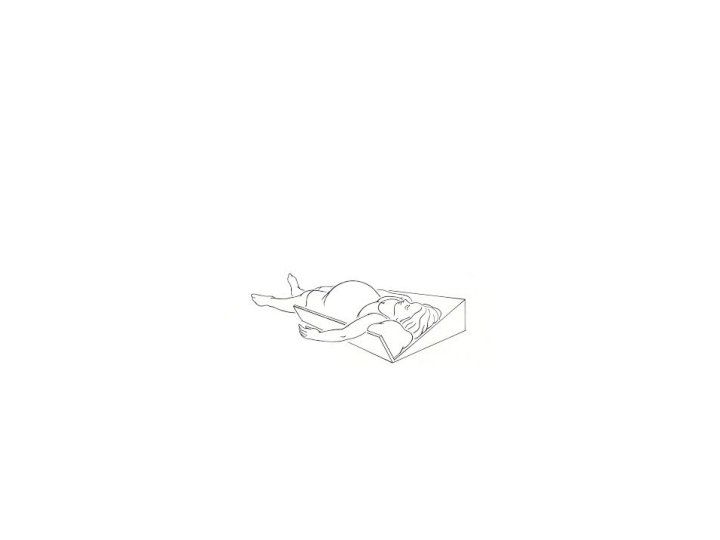
• In healthy late term pregnancy, the gravid uterus can be shift of the inferior vena cava if the patient is positioned in 15º left lateral deceits position. This has been shown to result in a 25% increase in cardiac output. • Therefore when performing CPR on the patient with a gestational age >25 week, manual displacement of the uterus to the left and upward, or rotating the patient so that their left hip is down ( blanket roll under the right hip), is recommended. • Alternately, a Cardiff resuscitation wedge, specially designed to maintain the patientin 27º left lateral decubitus position, can be used.

Physiology of pregnancy • Respiratory System 1. 60% increase in oxygen consumption & decreased FRC Implications – rapid desaturation & hypoxemia 2. increased minute ventilation and hypoxic ventilatory response Implications - chronic respiratory alkalosis, difficult determining benign vs. sinister causes of dyspnea 3. increased capillary engorgement & mucosal edema Implications – airway bleeding, nasal congestion, difficult airway, failed intubation

Physiology of pregnancy • 1. Cardiovascular System cardiac output increases by 50% (due to increased HR & SV). Increased contractility and LVEF. 2. SVR and PVR fall by up to 35%. SBP, DBP, MAP decrease during mid preganancy, return to baseline near term 3. Aorto-caval compression occurs from 13 -16 weeks Implications - supine hypotension - higher femoral/IVC pressures

Physiology of Pregnancy • Gastrointestinal System 1. Anatomical changes 2. Reduced lower esophageal sphincter pressure 3. Increased intra-gastric pressure 4. Delayed gastric emptying in labour but probably normal at other times • Implications - High incidence of gastro-oesophageal reflux - Increased risk of aspiration from ~ 16 -20 weeks gestation

Physiology of Pregnancy • Hematological System 1. 50% increase in plasma volume 2. 30% increase in red cell volume 3. Increased platelet turnover, clotting and fibrinolysis Implications - delayed presentation of hypovolaemia - physiological anemia of pregnancy - pro-coagulopathic state

Maternal CPR

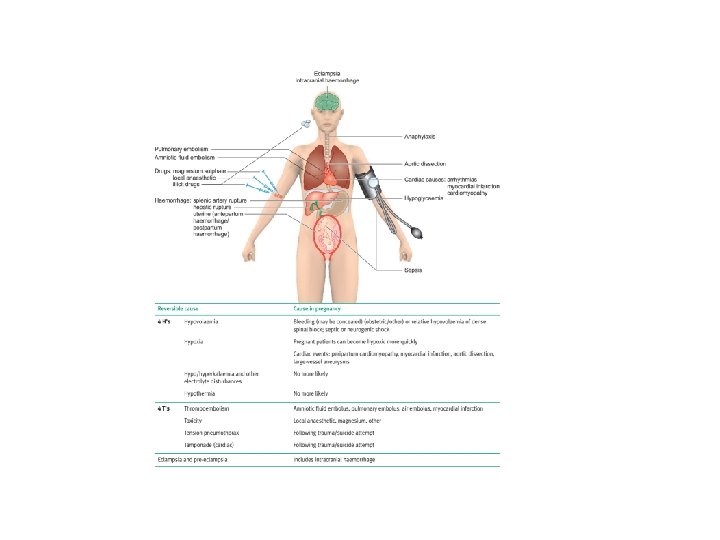
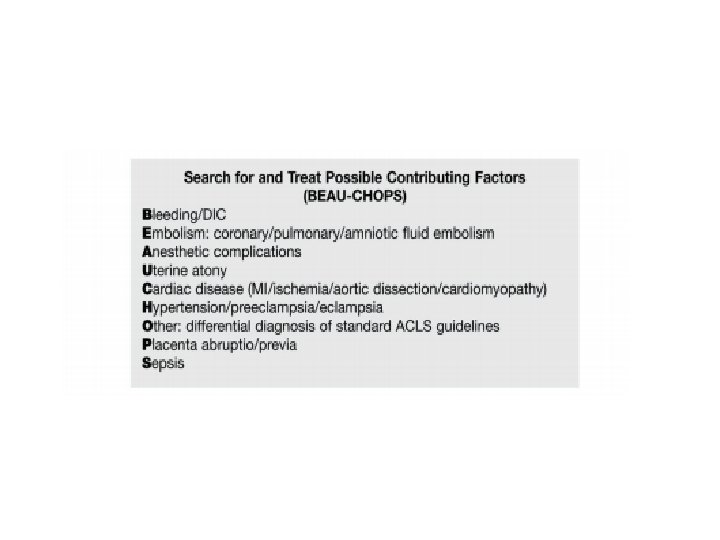
Maternal Collapse Cardiac Arrest -1: 30 000 deliveries The reversible causes in pregnancy n 1. 2. 3. 4. 4 T’s *Thromboembolic (PE, AFE) *Toxic &therapeutic Tension Pneumothorax Tamponade 4 H’s Hypoxia *Hypovolaemia Hypo/Hypekalemia Hypothermia

Effects of Pregnancy • Mass effect of the uterus • Reduced venous return (venal caval occlusion) • Reduced stroke volume (by 30%) • 20% reduction in pulmonary residual capacity • Increased oxygen requirement • Foetus, placenta and uterus (20% increase in demand) • Breast hypertrophy • Makes ventilation difficult • Oesophageal sphincter relaxation • Risk of reflux & aspiration

CPR in Pregnacy • Follow basic and advanced life support • Use drugs as normal • Left lateral tilt • Intubate early or use cricoid pressure • Defibrillation ok • Early recourse to delivery

Recognition • Ensure safe environment • Stimulate and assess response • Left later tilt • Wedge • Knees • Manual displacement • Get help • Send someone/ring buzzer • Shout • Go and get someone • Think of cause

Personnel • Head • Tilt • Airway/Oxygen/talk to the women • Wedge/Knees/Manual displacment • Chest • CPR (rotate every 2 minutes) • Arms • IV access/ Bloods/ fluids/ drugs • Uterus/Pelvis • Perimortem Caesarean section/ PPH • Scribe/Timekeeper • Runner

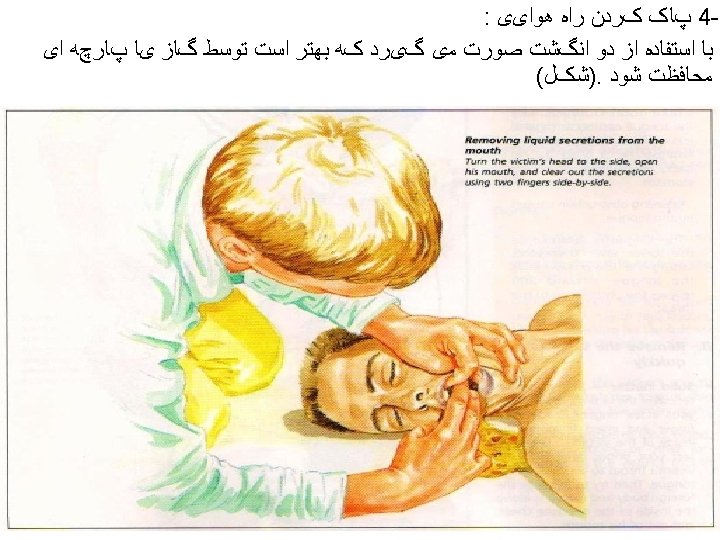
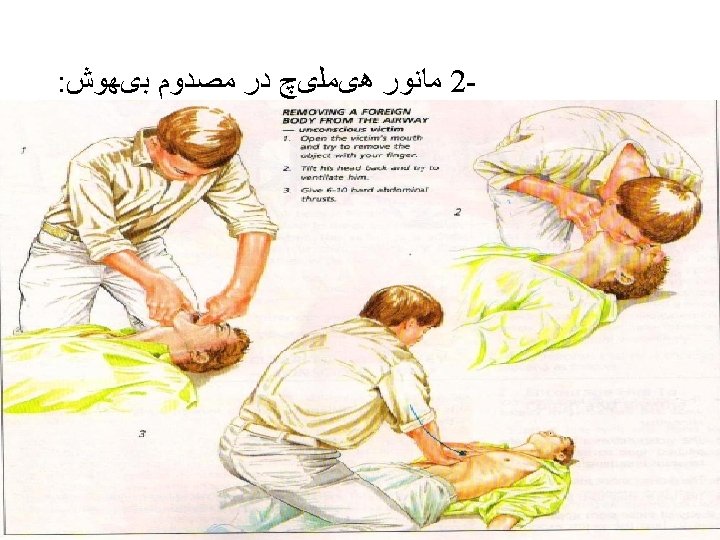
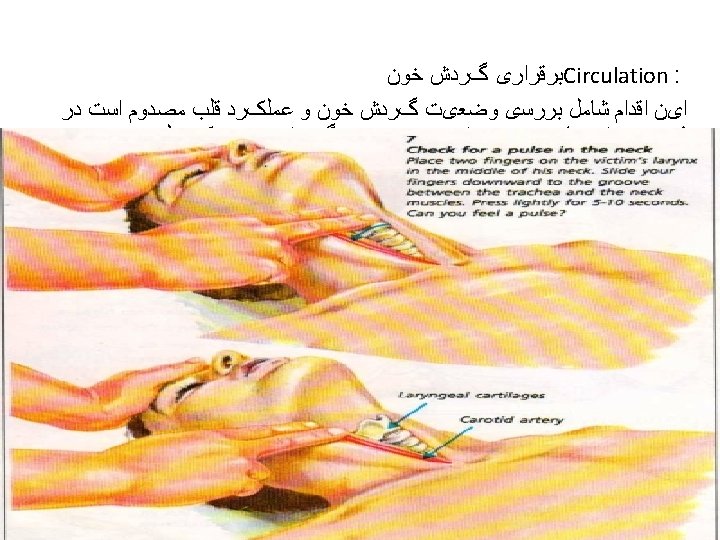
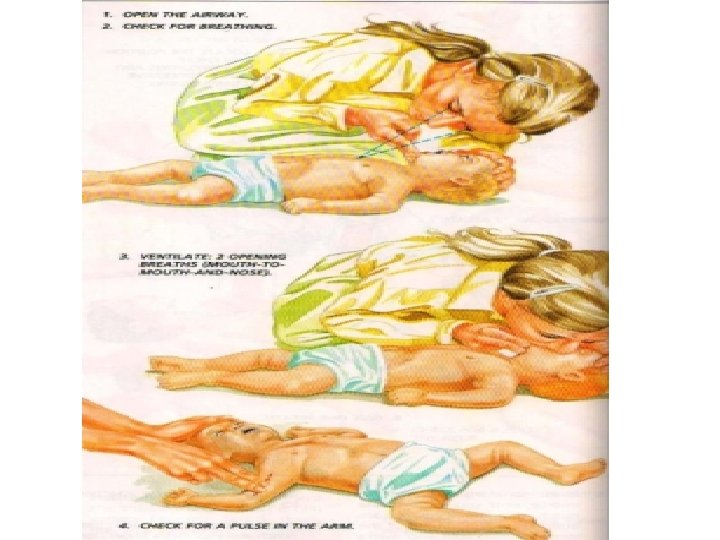
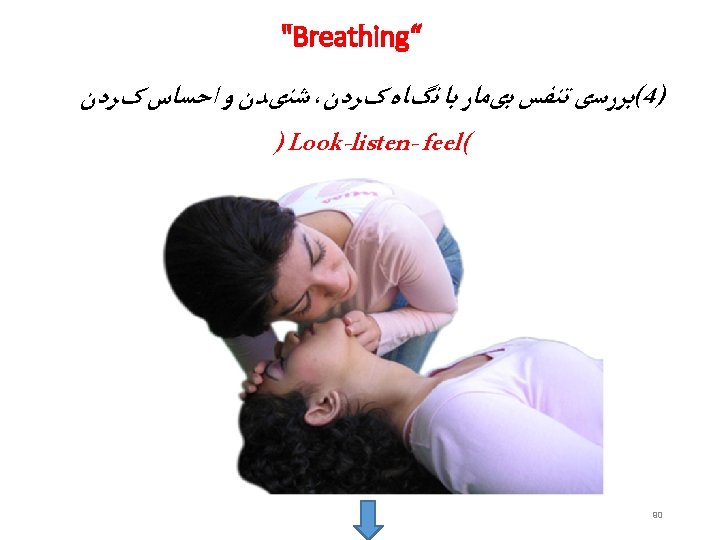
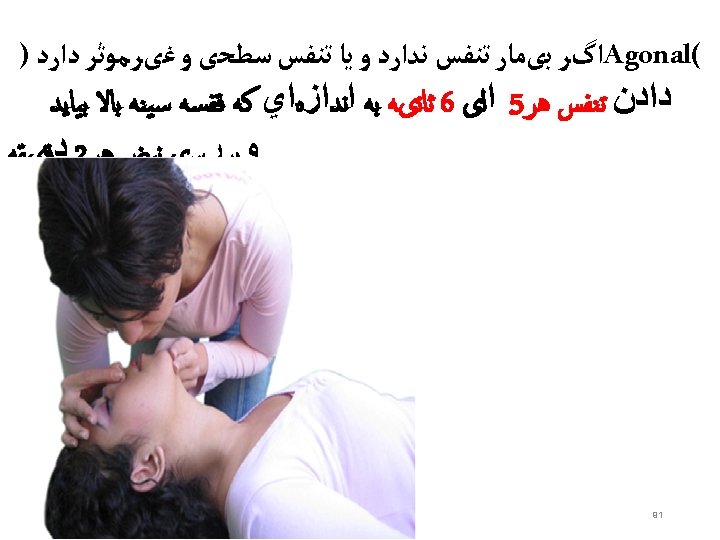
Airway • Check mouth foreign body • Open airway • Head tilt/chin lift • Jaw thrust • Assess for breathing • Look-chest wall movement • Listen- breath sounds • Feel- air movement • No breathing with a clear airway= no circulation – don’t need to feel for a pulse – start CPR • Gasping/ agonal breathing =sign of dying –start CPR • Think of cause

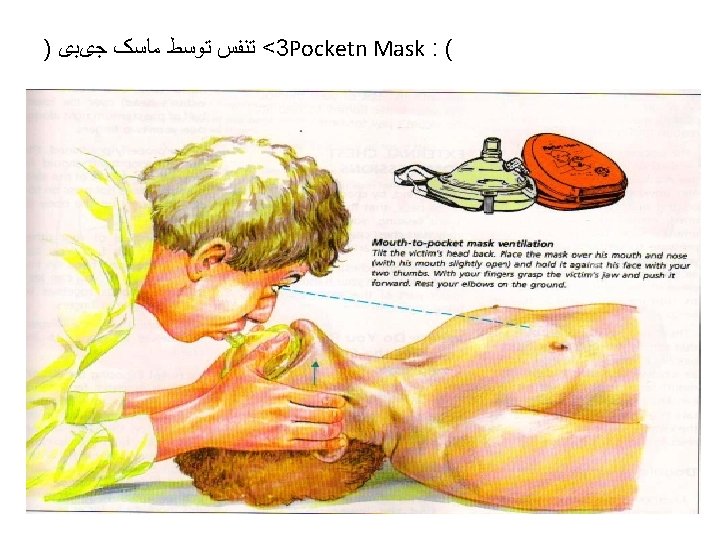
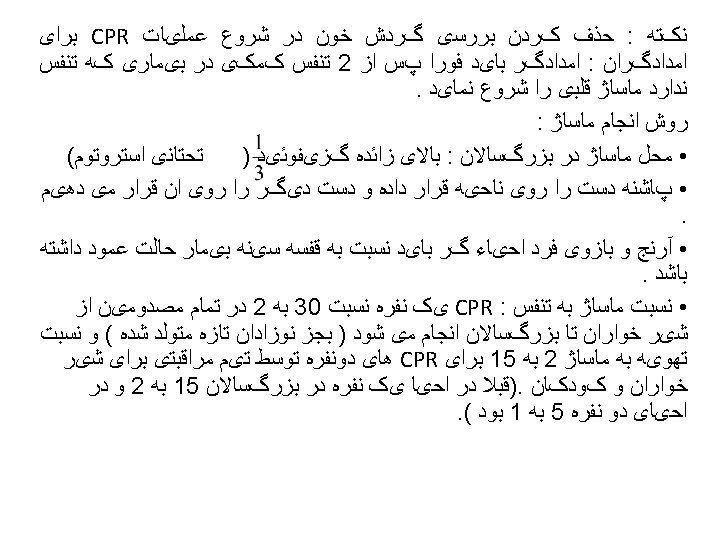
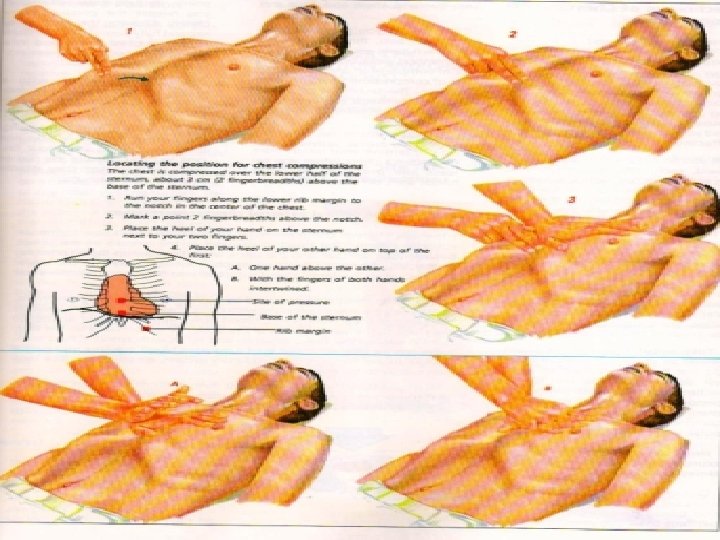
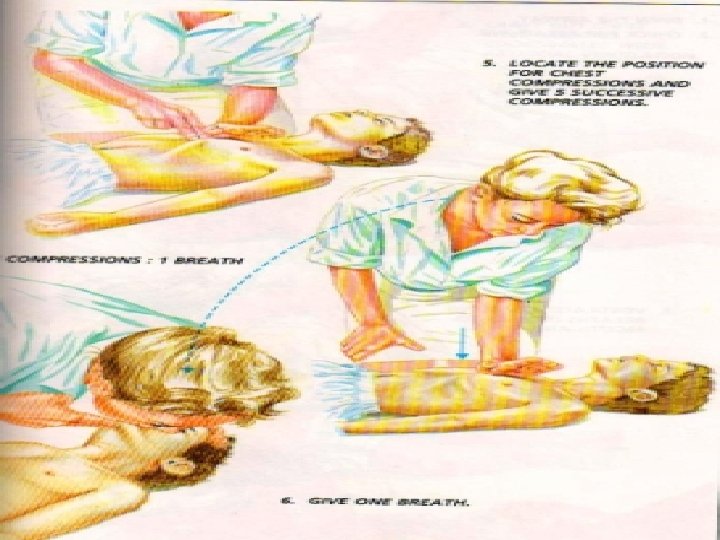
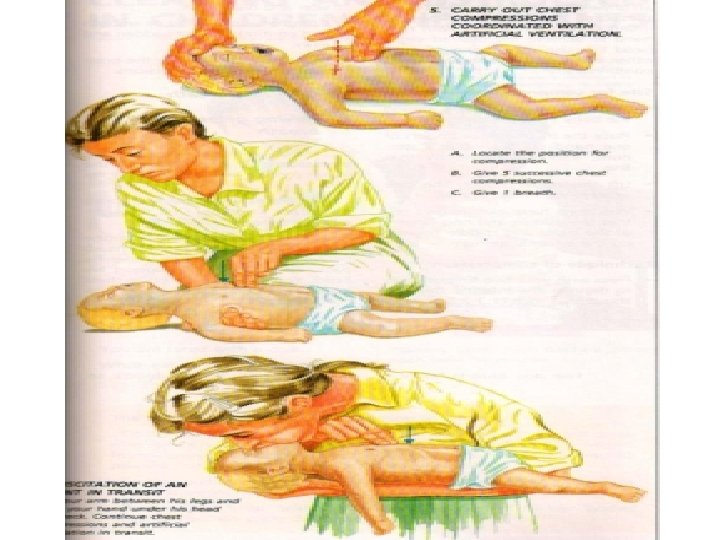
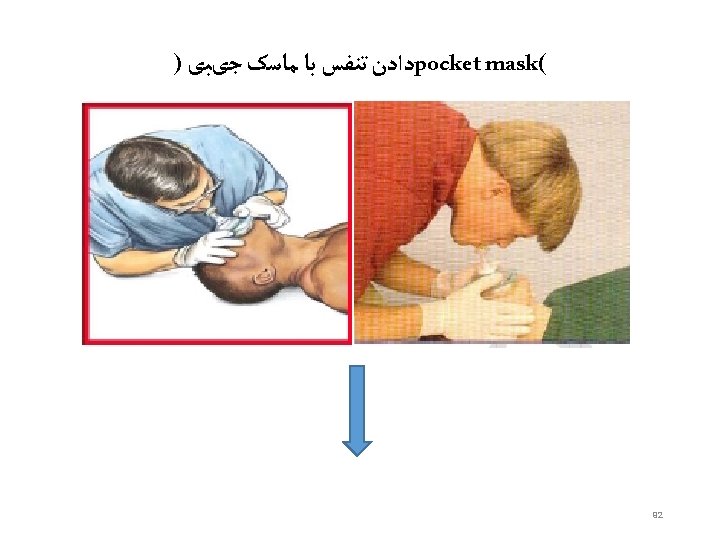
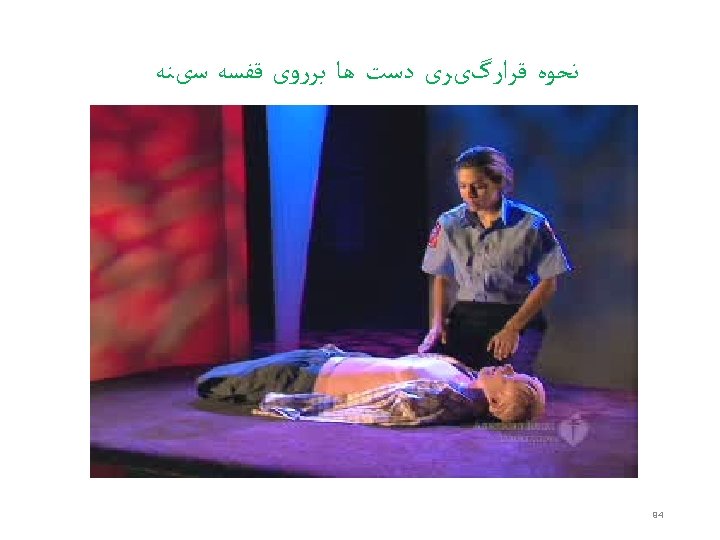
No Circulation or Not sure • 30 Chest compressions • • • Middle of lower half of sternum Depress 4 -5 cm 100 per minute Change person every 2 minutes Difficult in left lateral • Followed by 2 ventilations • • Pocket mask/oral airway/bag and mask/ ET tube Ensure chest rises Add high flow oxygen ASAP Once intubated- 10 breaths per minute , unsynchronised • Think of cause

• Lateral decubitus positioning greater than 30% have been shown to be associated whit significantly reduced force generation during chest compressions.

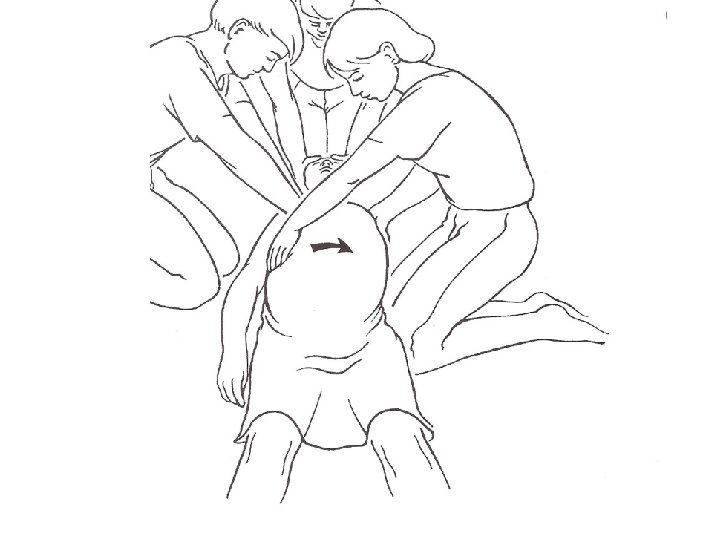
• An alternative to maternal tilt is lateral manual uterin displacement, which allows for the maintenance of the supine position and maximizes the force of the chest compressions • The AHA 2015 guidelines recommended initially performing manual displacement with a two-or one- handed technique while performing chest compressions in the supine position. if this is unsuccessful, then using a firm wedge to support the pelvis and thorax and provide 27 -30º of tilt is recommended.

Pathophysiological rationale for perimortem cesarean delivery-the 4 -Minute Rule • Although the maneuver discussed above may partially relieve vascular compression , perimortem cesarean delivery should theoretically be more effective. • It has been shown that cesarean delivery immediately increases the cardiac output in heathy women by 30%.


• Delivery should drastically reduce the cardiac output demand of the uterus and placenta, which consume approximately 30% of maternal cardiac output near term, and also provide approximately a 500 cc autotransfusion. • Additionally, delivery allows resuscitative access to the infant.

The 4 - minute Rule • If the mother remain pulseless, and the baby is viable, cesarean delivery should be started by 4 minutes and completed by 5 minutes into the code. • There is no rule that says delivery cannot be initiated before 4 minutes. if CPR is ineffective, or the cause of arrest is unlikely to be reversed whitin 4 minutes , it is prudent to proceed directly to cesarean.
less than 20 week’s gestation. Insignificant hemodynamic compromise from uterus, baby nonviable, no")
thus 1)less than 20 week’s gestation. Insignificant hemodynamic compromise from uterus, baby nonviable, no benefit in perimortem cesarean delivery. 2)20 to 23 week’s gestation. possibie hemodynamic compromise from uterus, baby nonviable, perimortem cesarean delivery may be considered to save mother. 3) 24 week’s or greater gestation. possible hemodynamic compromise from uterus, baby viable, perform perimortem cesarean delivery as indicated during arrest to benefit mother and baby.

Pathophysiological rationale for early endotracheal intubation • Physiological changes of late pregnancy increase the risk of life threatening complications of endotracheal intubation about tenfold. • Increase maternal oxygen consumption and a 20% reduction in the FRC of the lung due to compression by the gravid uterus, result in rapid oxygen desaturation if gas exchange is interrupted.

The causes of cardiopulmonary arrest in pregnancy • The approach of ACLS in non pregnant patients has a strong focus on managing the complication of ischemic heart disease, particularly shockable ventricular arrhythmias. • By contrast, obstetric arrest usually has a non arrhythmogenic cause. in the standard ACLS terminology, this equate whit pulseless electrical activity(PEA).

• The american college of cardiology has offered the memory aid “HS and TS”to help clinicians remember the cause of PEA/asystole. • Pregnancy entails some causes of cardiac arrest never seen in non pregnant patients, such as amniotic fluid embolism, and hypermagnesemia.

Differential of PEA/ asystol in pregnant patients: the Hsand TS Hs Hypovolemia • Abruptio placentae • Placenta previa/accreta/increta • Subcapsular hepatic hematoma • Ectopic pregnancy • Uterin rupture Hypoxia Hyperkalemia/hypermagnesemia h⁺↑(acidosis) Hypoglycemia Hypertention related complication of eclampsia/preeclampsia

Ts Thrombosis /embolism • Pulmonary embolism • Myocardial infarction • Amniotic fluid embolism • Venous air embolism Tention pneumothorax tamponade toxins

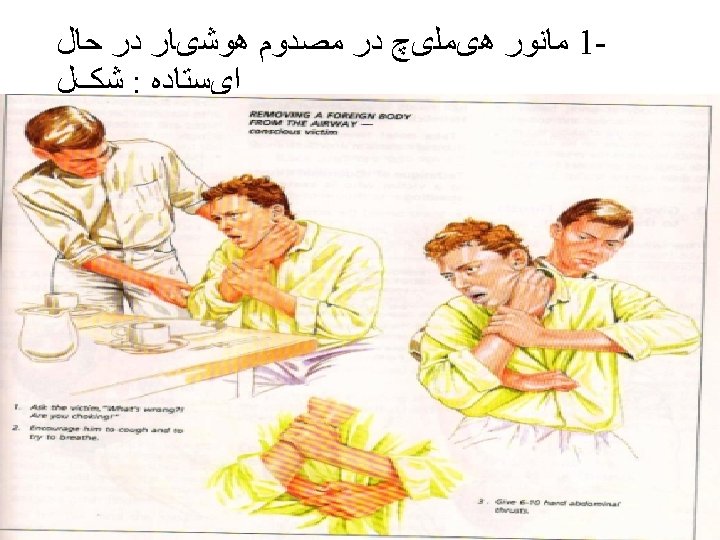
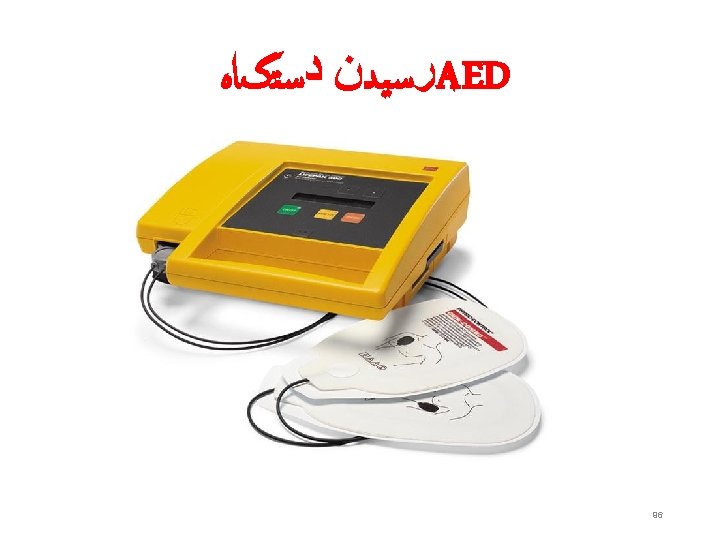
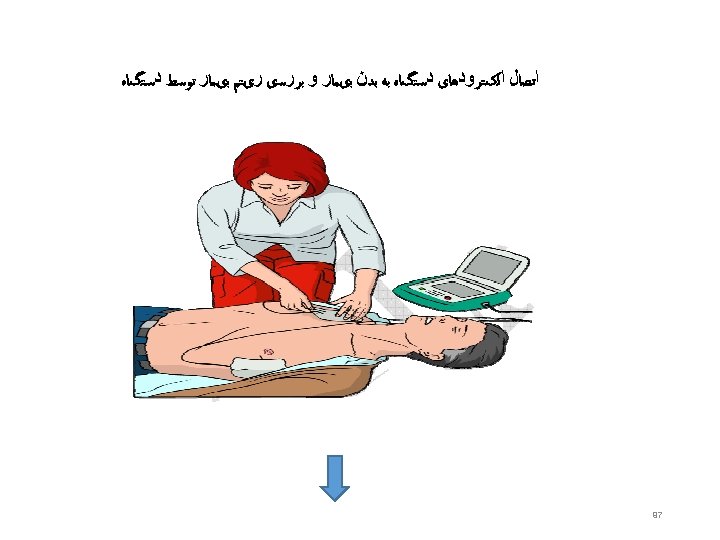
BASIC LIFE SUPPORT • BLS involves the early recognition of a medical emergency, activation of an emergency response system (e. g. , dialing 9 -1 -1 in the United States), and interventions made in response to SCA, heart attack, stroke, and foreign body airway obstruction (FBAO). • No equipment is required for these interventions, except for access to a telephone or an automated external defibrillator (AED), or both. • AEDs are included in BLS interventions because of their widespread availability in public spaces (e. g. , airports, schools, shopping centers, hospitals, casinos, sporting arenas), their uncomplicated application, automated cardiac rhythm analysis, and administered shocks (if indicated, based upon AED cardiac rhythm analysis).

BLS Dos and Don’ts of Adult High-Quality CPR • Rescuers Should Rescuers Should Not • Perform chest compressions at a rate of 100 -120/min Compress at a rate slower than 100/min or faster than 120/min Compress to a depth of at least 2 inches (5 cm) Compress to a depth of less than 2 inches (5 cm) or greater than 2. 4 inches (6 cm) • Allow full recoil after each compression Lean on the chest between compressions • Minimize pauses in compressions • Ventilate adequately (2 breaths after 30 compressions, each breath • delivered over 1 second, each causing chest rise) Provide excessive ventilation (ie, too many breaths or breaths with excessive force)

• In the 5 -year interim between the 2005 and 2010, the AHA BLS recommendations, clinical evidence, and survivor outcomes after sudden cardiac death support making uninterrupted chest compressions the priority intervention, above airway management, rescue breathing, and pulse check. • Airway, breathing, circulation (ABC) has been replaced by circulation, airway, breathing (CAB) for both adult and child resuscitations.

Push hard and push fast” remains the recommendation for chest compressions during CPR • Although evidence from human studies that identify the ideal chest compression rate is insufficient, current recommendations are for chest compressions to occur at a rate of > 100 per minute with minimal interruptions in both adult and childhood cardiac arrests. • adults, chest compressions should be at least 2 inches (5 cm) deep. • In children, chest compressions should be one-third the depth of the thorax.

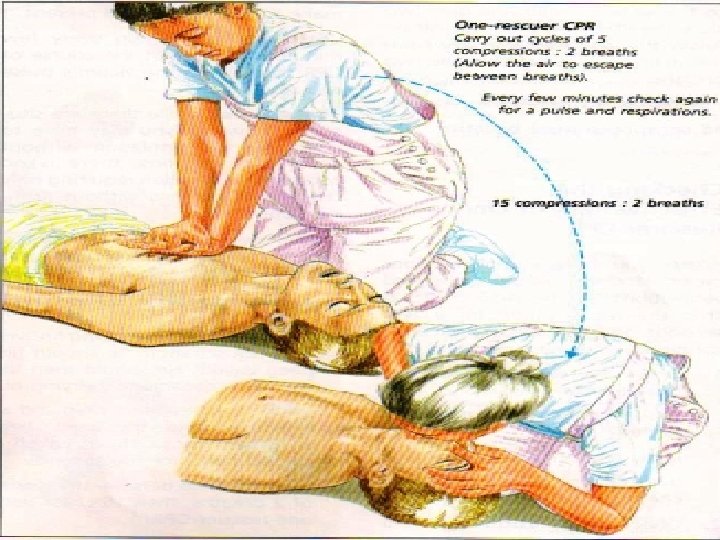
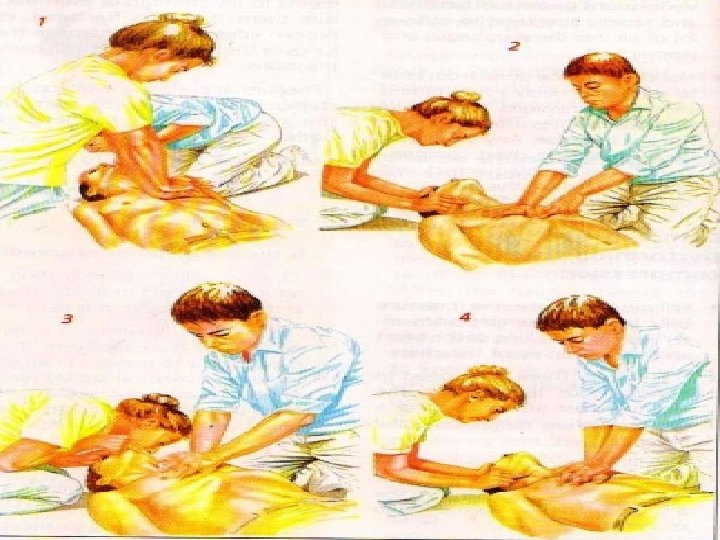
• Interruptions in chest compressions negatively affect coronary and cerebral perfusion, ROSC, and survival. The 2010 AHA Guidelines for CPR and ECC reflect these observations with an increased emphasis on limiting interruptions in chest compressions, even for other resuscitative measures (e. g. , rescue breaths, advanced airway placement, defibrillation, postshock rhythm analysis, pulse checks). • During single- and two-person CPR, the 2010 AHA Guidelines for CPR and ECC recommend compression: ventilation ratios of 30: 2 in both scenarios with minimal interruptions in chest compressions for rescue breaths. Although CPR is far less efficient than native circulation, when properly performed with limited interruptions, CPR can provide coronary circulation and cerebral blood flow sufficient to afford full recovery in many patients if ROSC can be re-established.

• Compression-only resuscitation may be a potential mechanism for encouraging resuscitation in the general population when potential rescuers are uncomfortable or unwilling to provide rescue breaths. • Without question, prompt initiation of chest compressions in the individual with SCA can be lifesaving.

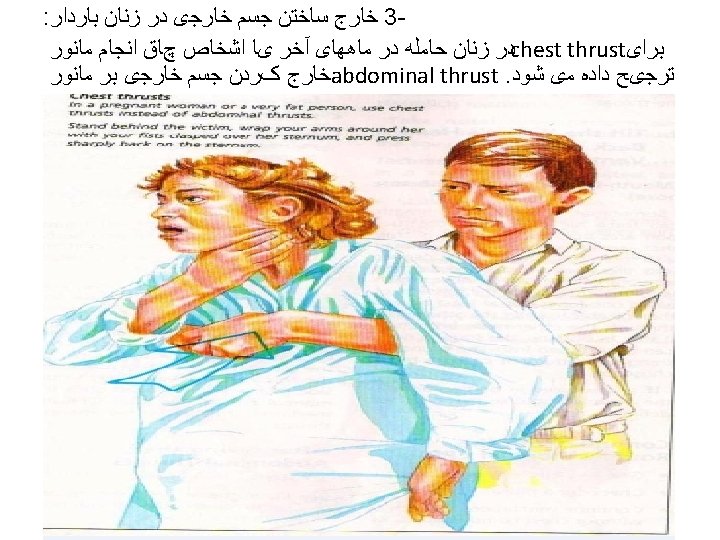
In pregnancy • Chest compressions should be provided at a position that is slightly higher on the sternum to adjust for the elevation of the diaphragm and abdominal contents caused by the gravid uterus.
: In adult victims of cardiac")
Chest Compression Rate: 100 to 120/min* • 2015 (Updated): In adult victims of cardiac arrest, it is reasonable for rescuers to perform chest compressions at a rate of 100 to 120/min. • 2010 (Old): It is reasonable for lay rescuers and HCPs to perform chest compressions at a rate of at least 100/min.
: During manual CPR, rescuers should perform chest compressions")
Chest Compression Depth* • 2015 (Updated): During manual CPR, rescuers should perform chest compressions to a depth of at least 2 inches (5 cm) for an average adult while avoiding excessive chest compression depths (greater than 2. 4 inches [6 cm]). • 2010 (Old): The adult sternum should be depressed at least 2 inches (5 cm).
: It is reasonable for rescuers to avoid leaning on")
Chest Recoil* • 2015 (Updated): It is reasonable for rescuers to avoid leaning on the chest between compressions, to allow full chest wall recoil for adults in cardiac arrest. • 2010 (Old): Rescuers should allow complete recoil of the chest after each compression, to allow the heart to fill completely before the next compression.
: Rescuers should attempt to")
Minimizing Interruptions in Chest Compressions* • 2015 (Reaffirmation of 2010): Rescuers should attempt to minimize the frequency and duration of interruptions in compressions to maximize the number of compressions delivered per minute. • 2015 (New): For adults in cardiac arrest who receive CPR without an advanced airway, it may be reasonable to perform CPR with the goal of a chest compression fraction as high as possible, with a target of at least 60%.

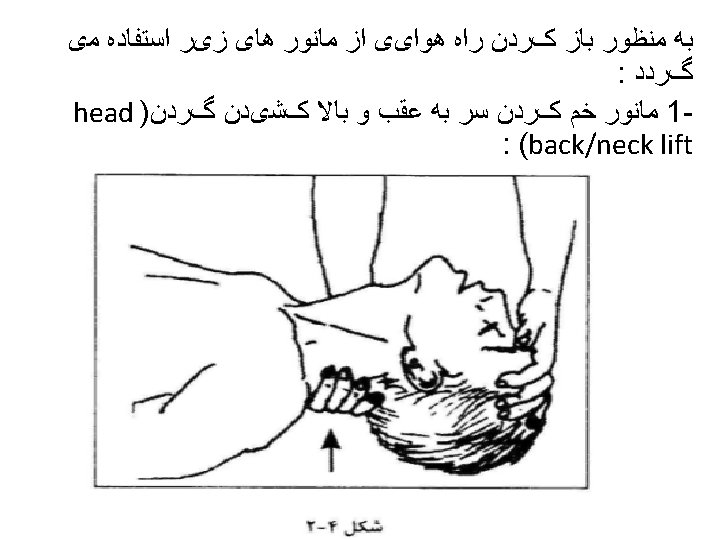
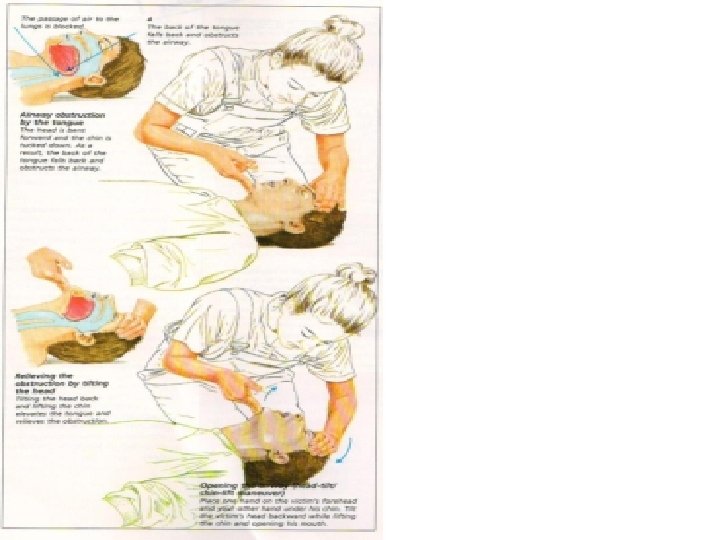
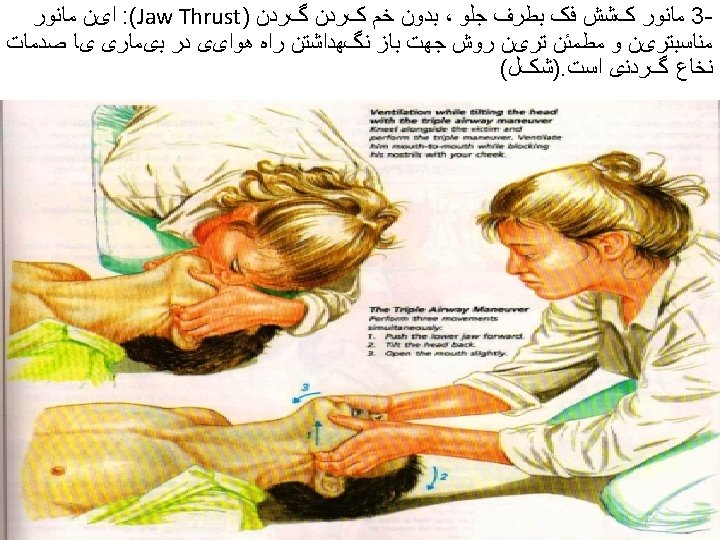
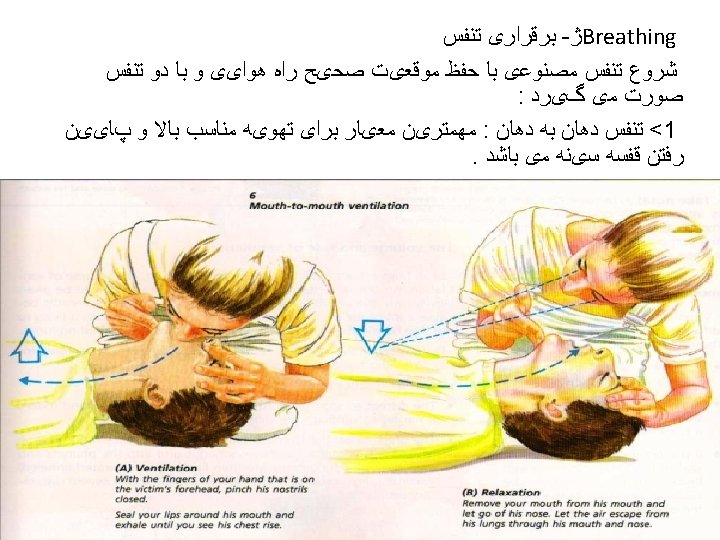
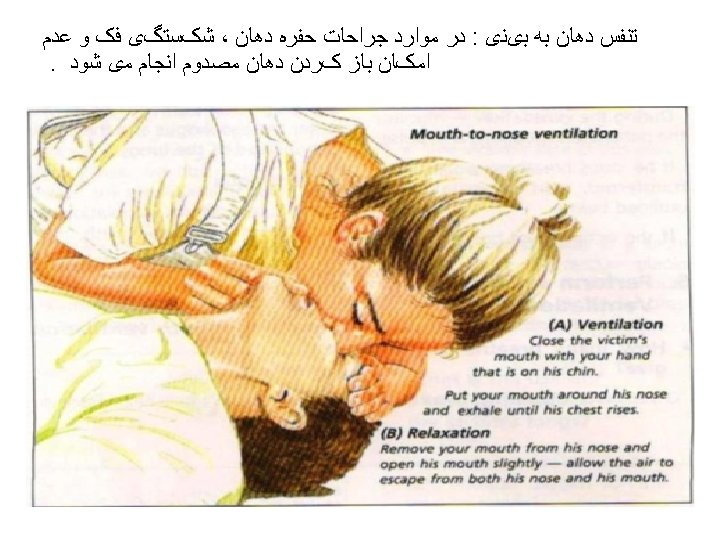
Airway Management and Ventilation in Cardiac Arrest • Anesthesia providers know that ventilation is critical for ROSC and for organ preservation during cardiac arrest. • The AHA ACLS training program has effectively conveyed this treatment as a priority but after the initiation of chest compressions and with minimal interruption of chest compressions in accordance with the 2010 AHA Guidelines for CPR and ECC. • The techniques for providing ventilation are dependent on the clinical situation. The head tilt–chin lift maneuver is recommended for initial airway control in most circumstances. The epiglottis, rather than the tongue, is the major cause of upper airway obstruction in the individual who is unconscious or sedated. Because of its ligamentous attachments to the hyoid bone, the epiglottis can be lifted by manual maneuvers that anteriorly displace the hyoid bone. These observations provide anatomic confirmation of the efficacy of the head tilt–chin lift technique for opening an obstructed airway. • The head tilt–jaw thrust maneuver accomplishes the same purpose in restoring airway patency.



• When rescue breathing is indicated for an individual in tracheal non intubated cardiac arrest, 2 breaths are delivered after 30 chest compressions during one- and two person CPR, providing that the rescuer(s) is(are) trained in CPR. 24 The 2010 AHA Guidelines for CPR and ECC excuse untrained rescuers from providing rescue breaths to ensure that uninterrupted chest compressions are provided until more qualified rescuers arrive. (Fig. 1085). 24 When performed, rescue breaths should be provided with only enough force and volume to cause the chest to rise. • Chest compressions are only minimally interrupted for the provision of rescue breaths (until a secure airway is established). 24 Oxygen delivery to tissues with CPR is limited more by blood flow and low cardiac output than arterial content. 60 Low cardiac output associated with CPR results in low oxygen uptake from the lungs that, in turn, reduces the need to ventilate the patient during this low flow state. 60

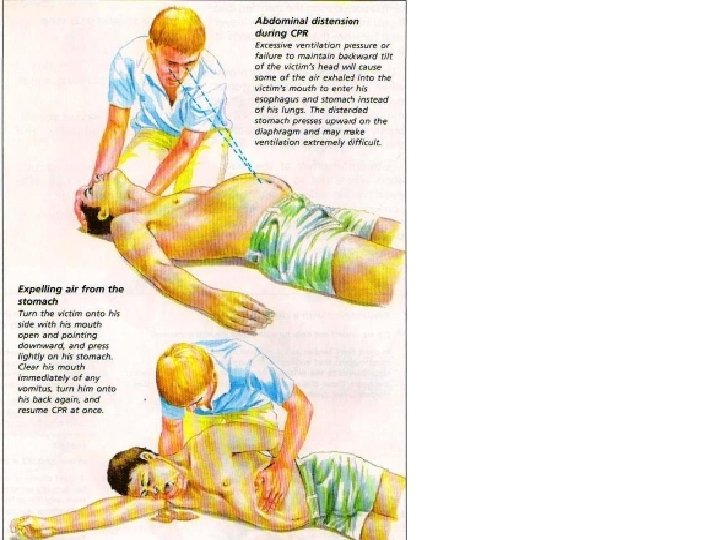
Excessive ventilation • Excessive ventilation force or tidal volume risks overcoming the esophageal opening pressure, contributing to gastric inflation, the potential for regurgitation, and its consequences. • If tracheal intubation is performed, then ventilation can occur at a rate of 10 breaths per minute with small tidal volumes and without interrupting chest compressions. Optimal tidal volumes or respiratory rates in the setting of cardiac arrest are not known. • Rescuers must avoid hyperventilation during resuscitation. The increased intrathoracic pressure from ventilation impedes venous return to the heart, decreases cardiac output, and compromises resuscitation efforts.

• During the first few minutes after the onset of cardiac arrest, chest compressions are the priority intervention, unless the cardiac arrest is due to • asphyxiation, drowning, or suffocation, which are the only circumstances that ventilation must be provided before chest compressions.

AVPU A=Allert V=Verbal P=Painfull U=Unresponse



saeid-mehri 65


Head tilt – chin lift




95


• Advanced airway placement during cardiac arrest is no longer a priority and is not mandated in the 2010 AHA Guidelines for CPR and ECC. • Attempting to place endotracheal intubation frequently causes significant interruptions in chest compressions, particularly when the provider undertaking intubation is inexperienced or lacks proficiency with the intervention. • Insufficient evidence demonstrates improved ROSC when an endotracheal tube is placed. However, in a large retrospective study of a 25, 000 in-hospital cardiac arrest database, an endotracheal tube placed during the first 5 minutes of cardiac arrest resuscitation did not improve the rates of ROSC but was associated with an improved 24 -hour survival.

• Once an advanced airway is inserted, its placement • must be confirmed by verification of breath sounds, chest • rise, and the presence of carbon dioxide during ventilation. • These parameters are assessed with each airway • manipulation in elective surgical cases and represent a • standard of care in the anesthesia environment. These • parameters—breath sounds, chest rise, and the presence • of carbon dioxide—are applicable and, because of • the unstable and high-risk environment (either out-ofhospital • or in-hospital) of a cardiac arrest, are mandatory • assessments when an airway is placed outside the surgical • department environment.

• Continuous monitoring of Pet. CO 2 is recommended during resuscitation attempts to ensure that the airway placement is secure, to guide compression quality, and to detect ROSC as demonstrated by a sudden increase in end-tidal carbon dioxide content.
: It may be reasonable")
Ventilation During CPR With an Advanced Airway • 2015 (Updated): It may be reasonable for the provider to deliver 1 breath every 6 seconds (10 breaths per minute) while continuous chest compressions are being performed (ie, during CPR with an advanced airway). • 2010 (Old): When an advanced airway (ie, endotracheal tube, Combitube, or laryngeal mask airway) is in place during 2 -person CPR, give 1 breath every 6 to 8 seconds without attempting to synchronize breaths between compressions (this will result in delivery of 8 to 10 breaths per minute).

Adult Advanced Cardiovascular Life Support All physicians, particularly those involved with invasive procedures in which sedation or anesthesia is administered, should be capable of performing CPR and other resuscitative interventions.

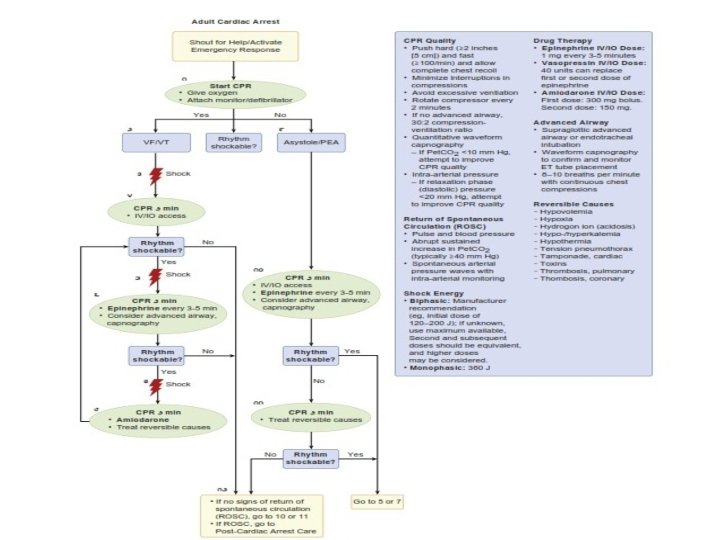
PULSELESS VENTRICULAR TACHYCARDIA OR VENTRICULAR FIBRILLATION • For therapeutic purposes, pulseless VT and VF are considered the same lethal entity in need of the same interventions, beginning with prompt defibrillation. Fortunately, these arrhythmias are the most treatable and yield the greatest likelihood of immediate and long -term survival in both in-hospital and out-of-hospital settings. Early defibrillation, not pharmacologic interventions, is responsible for the improved survival after VF cardiac arrest. As a result, PAD puts AEDs in public places so that defibrillation can occur at the earliest possible opportunity toindividuals in cardiac arrest, regardless of rescuer training. In operating rooms, ICUs, or other environments where continuous monitoring of cardiac rhythm is used and when a VT or VF arrest occurs, chest compressions should be immediately provided and defibrillation performed at the earliest opportunity. A period of chest compression before defibrillation is not recommended in the 2010 AHAGuidelines for CPR and ECC. If a monophasic defibrillator is available, then a single 360 J shock should be delivered. With biphasic defibrillators, biphasic truncated exponential waveforms should use 150 to 200 J for first shock, depending on the manufacturer’s recommendation. Energy settings for rectilinear biphasic waveforms should use 120 J for the initial shock. For simplicity and improved decision-making during resuscitation efforts, if the rescuer is unfamiliar with the waveform used or the manufacturer recommendations, then the maximal available energy should be used as the default energy. 61 Chest compressions should be immediately resumed after the delivery of shock and continued for 2 minutes before reassessing the underlying cardiac rhythm, unless obvious evidence for ROSC occurs. The 2010 AHA Guidelines for CPR and ECC recommend three stacked shocks to be used only in the coronary catheterization laboratory or in the cardiac surgical operating rooms after weaning from cardiopulmonary bypass.

• • • • • No evidence supports one biphasic waveform over another. All biphasic defibrillators available today areimpedance compensated and adjust the delivered dose of energy in response to the measured transthoracic impedance (TTI) with each shock. (This technology has resulted in greater first-shock efficacy and is not used in monophasic defibrillators. ) Defibrillation energies should be increased until VF is terminated or maximal defibrillator energy output is reached. In circumstances in which VT or VF is terminated with defibrillation but VT or VF recurs, defibrillation should use the previously successful energy level. If ROSC has not occurred after an initial defibrillatory attempt, then five cycles of CPR consisting of 30 compressions to 2 ventilations should be performed before cardiac rhythm reanalysis. Placement of a supraglottic airway or endotracheal intubation can be considered in this interval. During this opportunity, peripheral IV access should be attempted if not already established.

VASOPRESSOR THERAPY IN CARDIAC ARREST • The 2010 AHA Guidelines for CPR and ECC de-emphasizes the use of medications in resuscitation attempts. Emphasis is placed on providing quality, uninterrupted chest compressions and defibrillation attempts every 2 minutes as needed for ongoing resuscitation efforts. Although epinephrine has been a mainstay of pharmacologic therapy in resuscitation efforts for many years, clinical evidence is lacking for improved survival and neurologic recovery after cardiac arrest when epinephrine is administered. Vasopressin and amiodarone are two other pharmacologic agents commonly administered during cardiac arrest. Just as with epinephrine, vasopressin and amiodarone lack convincing clinical evidence for improved hospital discharge and neurologic recovery when administered during resuscitation efforts. All three medications have demonstrated benefit in ROSC during cardiac arrest but no benefit on hospital discharge. Epinephrine’s benefit in cardiac arrest states arises from its potent α- and β-adrenergic stimulation effects, resulting from a 1 mg (10 m. L of a 1: 10, 000 solution) IV dose. α 1– and α 2– receptor stimulation results in peripheral vasoconstriction, leading to increased aortic diastolic pressure. Increased aortic diastolic pressure improves coronary blood flow. The modest increase in aortic diastolic pressure might provide improved coronary blood flow during cardiac arrest or other low coronary blood flow states, resulting in ROSC. Epinephrine-induced β-adrenergic stimulation increases myocardial contractility. This consequence increases myocardial oxygen demand probably further exacerbates subendocardial ischemia during the low-flow states of cardiac arrest (also see Chapter 16).
 was included in previous resuscitation guidelines")
• • • • Vasopressin (40 units) was included in previous resuscitation guidelines based on observations that survivors of cardiac arrest had increased endogenous vasopressin levels. Vasopressin is an endogenous peptide hormone secreted by the posterior pituitary gland in response to hypovolemia or systemic hypoperfusion states. When intravenously administered, intense peripheral vasoconstriction results from the stimulation of V 1 receptors in the endothelium. Vasopressin lacks adrenergic stimulation and, as a result, has limited increases in myocardial contractility, myocardial and cerebral oxygen consumption, and metabolic demands. No survival benefit has been observed in humans when vasopressin was used with or without epinephrine in cardiac arrests.

• Amiodarone was included in the ACLS algorithms • because of its ability at an IV dose of 300 mg to terminate • ventricular arrhythmias during cardiac arrest that were • resistant to defibrillation after epinephrine administration. • Amiodarone’s antiarrhythmic effect occurs through • sodium and calcium channel blockade, potassium efflux • antagonism, and adrenergic (α- and β-) blocking effects, • producing prolonged action potentials and increased • refractoriness in all cardiac tissue. Similar to epinephrine, • amiodarone improves the rate of ROSC but has no • observed influence or benefit on hospital discharge or • neurologic outcomes.

• Substitution of one dose of IV epinephrine with 40 units IV vasopressin during resuscitative efforts in cardiac arrest is acceptable in the 2010 AHA Guidelines for CPR and ECC

• Amiodarone is a first-line antiarrhythmic medication used in cardiac arrest events and is endorsed for use in the 2010 AHA Guidelines for CPR and ECC. 61 In the study, Amiodarone in Out-of-Hospital Resuscitation of Refractory Sustained Ventricular Tachycardia (ARREST), Kudenchuk and colleagues 114 reported the results of a randomized, prospective study in which 300 mg IV amiodarone or placebo was administered to patients in out-of-hospital cardiac arrest with persistent VF after three defibrillation attempts and 1 mg IV epinephrine. The study demonstrated significant increases in survival to hospital admission in the amiodarone-treated group but was unable to demonstrate any difference in hospital discharge rates. In the Amiodarone versus Lidocaine in Pre-Hospital Ventricular Fibrillation Evaluation (ALIVE) study, Dorian and colleagues 115 reported the results of a double-blind, controlled clinical trial comparing amiodaronewith lidocaine in patients experiencing out-ofhospital cardiac arrest in Toronto, Canada. Their results demonstrated amiodarone’s superiority to lidocaine in terminating persistent VF in the out-of-hospital setting. Similar to the ARREST study, the ALIVE study was able to demonstrate the improvement produced by amiodarone only in survival to hospital admission, not to discharge, when compared with lidocaine or placebo. Based on these studies, VF resistant to defibrillation and epinephrine therapy warrants amiodarone therapy to augment the attempts to terminate the arrhythmia, recognizing that a longterm benefit for such therapy is lacking.

• • • • During resuscitation efforts, 1 mg IV epinephrine should be administered as the initial pharmacologic drug in VF or PVT. This dose can be repeated every 3 to 5 minutes as long as cardiac arrest persists. Defibrillation should be attempted 2 minutes after epinephrine injection. For VF resistant to defibrillation attempts, 300 mg IV amiodarone should be considered and can be repeated once at a 5 -minute period (if necessary) with a 150 mg IV dose. As with epinephrine, defibrillation should be attempted 2 minutes after amiodarone injection. No other vasopressors or antiarrhythmic medications should be administered than those studied and endorsed by the AHA in its resuscitation guidelines.
 refers to a heterogeneous group of")
PULSELESS ELECTRICAL ACTIVITY • Pulseless electrical activity (PEA) refers to a heterogeneous group of cardiac rhythm disorders, all characterized by pulselessness in the presence of organized electrical activity. High priority must be given to identifying possible reversible causes of PEA (Box 108 -4). Severe hypoxia in respiratory emergencies can result in PEA. In the traumatized patient, hypovolemia, cardiac tamponade, andtension pneumothorax are possible causes of cardiac arrest and must be considered and acutely treated. Unanticipated cardiac arrest occurring in the intraoperative and postoperative periods should include acute massive pulmonary thromboembolism or air emboli as possible causes. In the pregnant woman, uterine compression of the inferior vena cava, amniotic fluid embolism, or uterine rupture are possible sources of PEA (also see Chapter 77). Idioventricular rhythms might accompany derangements such as severe hyperkalemia, metabolic acidosis, or drug (e. g. , digitalis, β-blockers, calcium channel blockers, tricyclic antidepressants) overdose. In every circumstance, prompt initiation of chest compressions and the administration of 1 mg epinephrine are recommended as temporizing measures until more definitive therapy can be provided once the cause for the PEA is identified. Each of these scenarios has an associated intervention unique to that situation. Asystole or VF can develop if PEA is not corrected.

ASYSTOLE • Asystole is the complete and sustained absence of electrical activity and is often a terminal event. In most patients, systole is irreversible, but a brief trial of resuscitation, beginning with oxygen therapy and IV epinephrine after effective chest compressions, is indicated particularly in the setting of witnessed cardiac arrest. Occult VF is more theory than reality. The concern that asystole is actually VF is unrealistic and should not prompt defibrillation attempts. Atropine is no longer recommended for treating asystole. When resuscitation efforts are pursued for patients found in asystole, oxygenation, at least 2 minutes of chest compressions, and IV epinephrine should be provided before cardiac rhythm analysis occurs, for ROSC assessment, or electrical activity resumes.

• The combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest. Also, vasopressin does not offer an advantage over the use of epinephrine alone. Therefore, to simplify the algorithm, vasopressin has been removed from the Adult Cardiac Arrest Algorithm– 2015 Update.
 in intubated patients after 20")
• Low end-tidal carbon dioxide (ETCO 2 ) in intubated patients after 20 minutes of CPR is associated with a very low likelihood of resuscitation. While this parameter should not be used in isolation for decision making, providers may consider low ETCO 2 after 20 minutes of CPR in combination with other factors to help determine when to terminate resuscitation.
: In intubated patients, failure")
ETCO 2 for Prediction of Failed Resuscitation • 2015 (New): In intubated patients, failure to achieve an ETCO 2 of greater than 10 mm Hg by waveform capnography after 20 minutes of CPR may be considered as one component of a multimodal approach to decide when to end resuscitative efforts but should not be used in isolation.
: Vasopressin in combination with epinephrine offers no")
Vasopressors for Resuscitation: Vasopressin • 2015 (Updated): Vasopressin in combination with epinephrine offers no advantage as a substitute for standard-dose epinephrine in cardiac arrest. • 2010 (Old): One dose of vasopressin 40 units IV/ intraosseously may replace either the first or second dose of epinephrine in the treatment of cardiac arrest.
: It may be reasonable to administer epinephrine")
Vasopressors for Resuscitation: Epinephrine • 2015 (New): It may be reasonable to administer epinephrine as soon as feasible after the onset of cardiac arrest due to an initial nonshockable rhythm.

• If the local anesthetic- induced systemic toxicity is suspected, it should be treated whit the rapid infusion of a lipid emulsion(intralipid 20 % 1. 5 cc/kg as a bolus followed by an infusion of 0. 25 cc/kg per min; bolus can be repeated).

If you think the patient is hypermagnesemic or hypercalemic • Give cacl, 5 meq IV and repeat if warranted. • ECG abnormalities related to these electrolyte abnormalities generally normalize with 1 -2 doses.

thanx

- Slides: 136