Mastering NMR Lipoprofile Case Based Approach Tara Dall

Mastering NMR Lipoprofile Case Based Approach Tara Dall, MD Advanced Lipidology Delafield, Wisconsin Diplomate, American Board of Clinical Lipidology www. advlip. com
 are the causal agents in")
LDL Particles Cause Atherosclerosis Low Density Lipoprotein particles (LDL) are the causal agents in atherosclerosis. 1 The more lipoprotein particles a person has, the higher the risk for plaque buildup that causes heart attacks, regardless of how much cholesterol those particles carry. 1 Fredrickson et al. NEJM 1967; 276: 148

Small LDL Particles Contain Less Cholesterol Than Large LDL Particles Up to 70% More Particles 100 mg/d. L Large LDL Small LDL Cholesterol Balance

Even LDL Particles of the Same Size can Differ in Cholesterol Content Up to 40% More Particles 100 mg/d. L Normal Cholesterol Per Particle Less Cholesterol Per Particle Cholesterol Balance

Disease States where LDL-Particle and LDL-Cholesterol are most likely to Differ and NMR testing should be considered F Known Coronary Heart Disease F Metabolic Syndrome F Diabetes F Family history premature heart disease F High Triglyceride and low HDL
 in microns")
Small, Dense LDL Subclass Relations with Carotid IMT in MESA ΔIMT (SE) in microns per 1 -SD Variable IDL-P Separate Models Joint Model 26. 7 (4. 1)** Large LDL-P 4. 9 (4. 4) Small LDL-P 31. 7 (4. 2)** LDL Size# -20. 9 (4. 5)** From linear regression analyses adjusted for age, sex, race, smoking, and hypertension. **p<0. 0001 Mora et al. Atherosclerosis 2007; 192: 211 -1
 in microns per")
Small, Dense LDL Relations with Carotid IMT in MESA ΔIMT (SE) in microns per 1 -SD Separate Models Joint Model 26. 7 (4. 1)** 10. 9 (5. 4) Large LDL-P 4. 9 (4. 4) 42. 9 (6. 7)** Small LDL-P 31. 7 (4. 2)** 39. 1 (7. 1)** LDL Size# -20. 9 (4. 5)** 14. 5 (7. 2) Variable IDL-P From linear regression analyses adjusted for age, sex, race, **p<0. 0001 smoking, and hypertension. # “Joint Model” included both LDL size and LDL-P. Mora et al. Atherosclerosis 2007; 192: 211 -1

Small, Dense LDL Published studies confirm there is no association of LDL size with CHD events independent of LDL-P: VA-HITCirculation 2006; 113: 1556 -63 EPIC-Norfolk. JACC 2007; 49: 547 -53

Small LDL-P Conclusions • NMR data confirm that patients with predominantly small LDL particles have higher CHD risk. • These patients also have LDL-P > LDL-C discordance. • Independent of LDL-P, there is no excess risk associated with small LDL size.

ADA and ACC Consensus Statement on Lipoprotein Management in Patients with Cardiometabolic Risk TREATMENT GOALS Highest-risk patients, including those with 1) known CVD or 2) Diabetes plus one or more additional CVD risk factor LDL-C Non-HDL-C Apo. B (mg/d. L) < 70 High-risk patients, including those with 1) no diabetes or < 100 known clinical CVD but 2 or more additional major CVD risk factors or 2) Diabetes but no other CVD risk factors < 100 < 130 < 80 < 90 Brunzell JD, Davidson M, Furberg CD et al. Diabetes Care 2008; 31: 811 -822

Clinical Cutpoints for LDL Percentile: 20 th 50 th 80 th Optimal High LDL Cholesterol Framingham Offspring 70 MESA 100 130 160 190 220 250 mg/d. L LDL Particle Number 700 1000 1300 1600 1900 Percent of Subjects 2200 2500 nmol/L

Recommendations from AACC Lipoproteins and Vascular Diseases Division Working Group on Best Practices Suggested Treatment Goals Apo. B LDL-C Non-HDL-C mg/d. L < 70 < 80 < 100 < 80 < 120 < 100 < 130 < 150 LDL-P nmol/L < 1100 < 1400 Contois. JH, et al. Clinical Chemistry 2009; 55: 407 -419

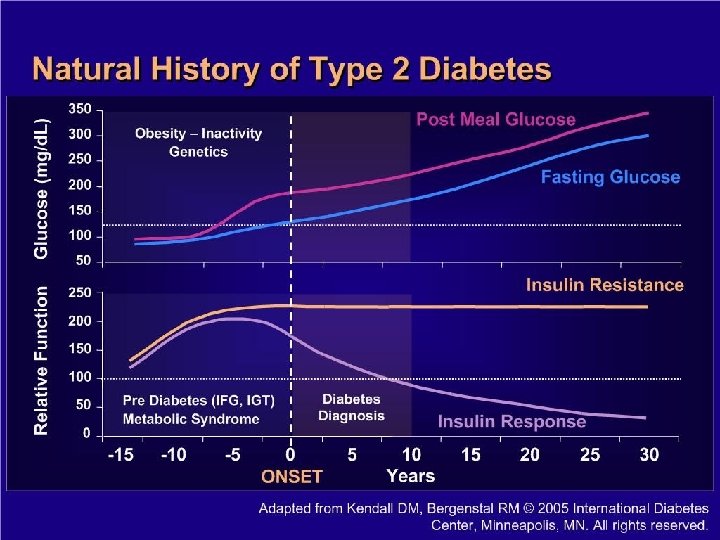
New NMR Report provides Information Regarding Insulin Resistance Possibly years before Diabetes diagnosis Presents with abnormal Glucose

Case Studies

Particle Size may not provide independent prediction of CV risk however…. . Size is helpful however in determining treatment approach
 freq associated with Insulin")
Particle size F Small Dense LDL particles (Pattern B ) freq associated with Insulin resistance, diabetes, metabolic syndrome F Large Bouyant LDL particles (Pattern A) associated with Familial Hypercholesterolemia F Bottom line: too many LDL particles puts patient at risk regardless of whether they are large or small

ML 38 yr Obesity, Fam History Premature CAD

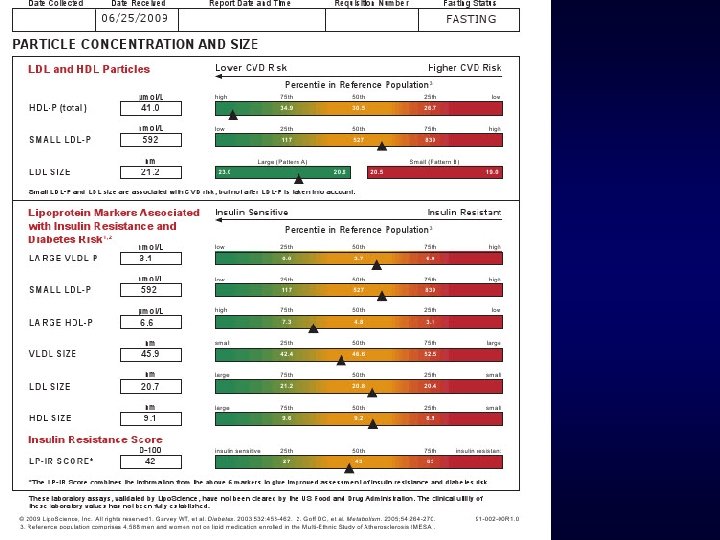
ML 38 yr old Male initial 3/18/2009 F Vitals: 3/18/2009 F Wt 396. 6 lb, Ht 73 in, BMI 52 F WC 64 inches F BP 146/88 pulse 84 reg F Hg. AIC 5. 8 F Glucose 119 fasting

ML 38 yr Male F PMH: hypertension untreated, IFG F Medications: none F Fam. Hx: Premature Heart Disease mgma age 64 deceased, M grandfather age 54 MI, Paternal granmother age 60 MI, Mom, Maternal grandfather, Paternal Grandmother diabetes F SH: married nonsmoker (quit 2001), no alcohol, no regular exercise, American diet
 LDL –C 112 Non HDL-C 137 Low HDL 34")
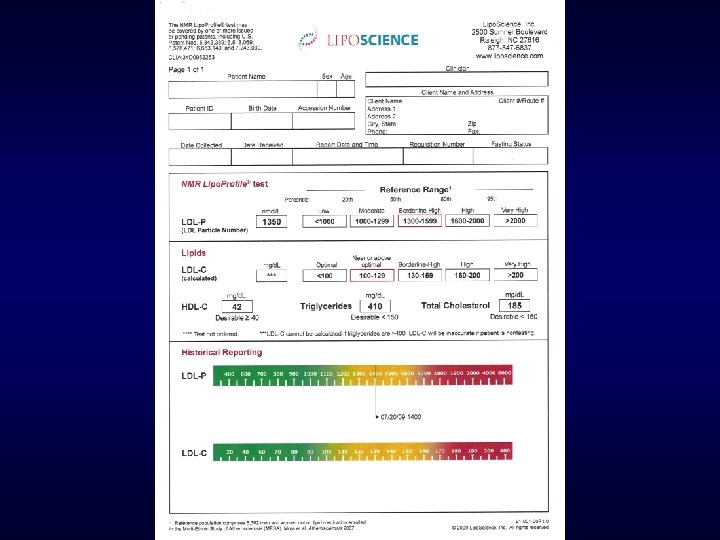
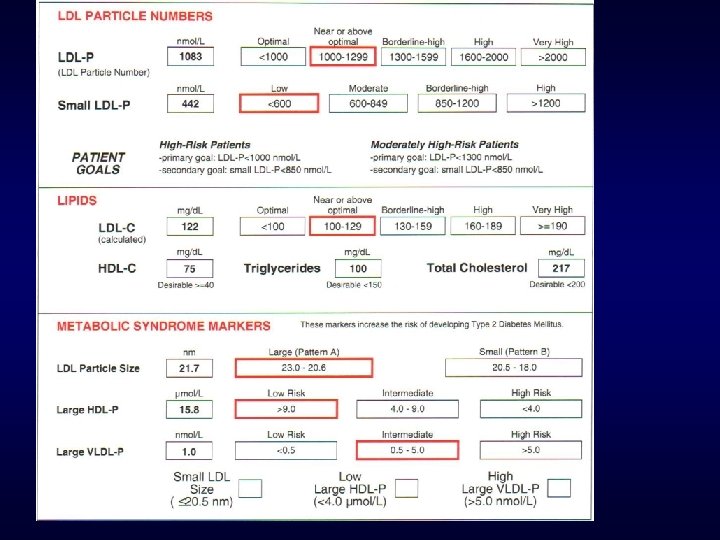
LDL -P 1906 (optimal <1000) LDL –C 112 Non HDL-C 137 Low HDL 34 Triglyceride 124
 Also")
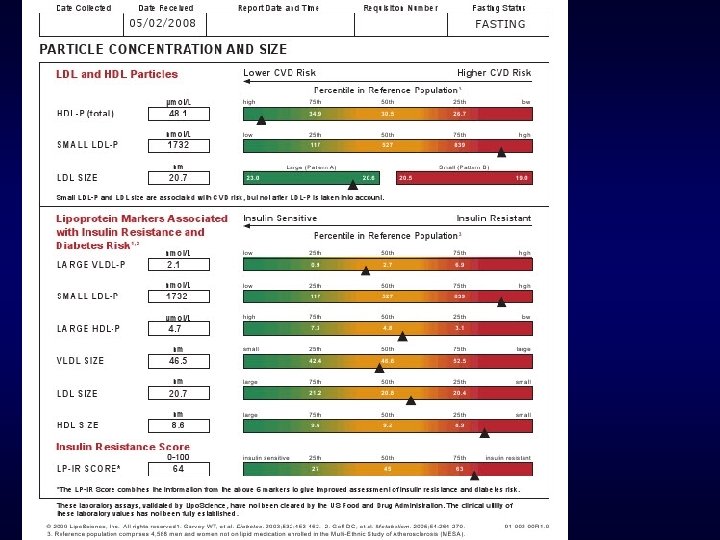
Total LDL P 1906 Small LDL P 1444 IR score 79 (abnormal >45) Also 4/5 metabolic syndrome criteria met

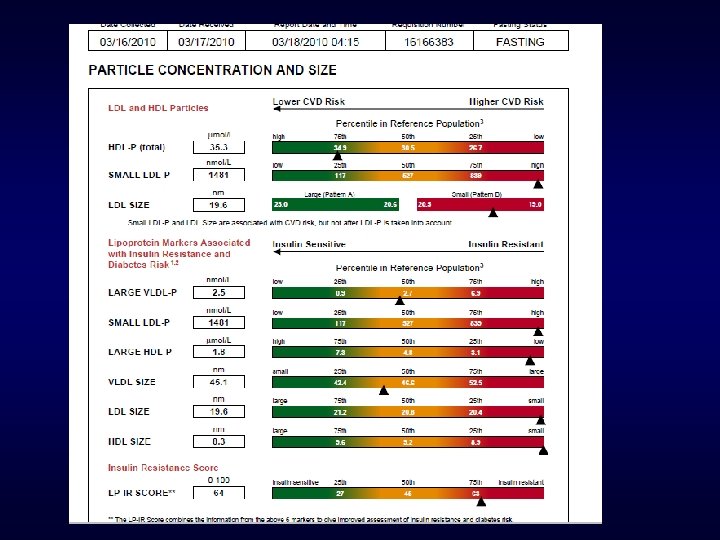
What therapy? LDL P dropped 750 points Non HDL C dropped to 90 from 137

BP 120/80, Hg. AIC 5. 2 Glucose 68 IR SCORE dropped From 79 to 38

What therapy? LDL P dropped 750 points Non HDL C dropped from 137 to 90 1. 2. 3. 4. 5. Statin Niacin Fibrate Weight loss Metformin


5 months later 133 lb weight loss
 over 9 months time")
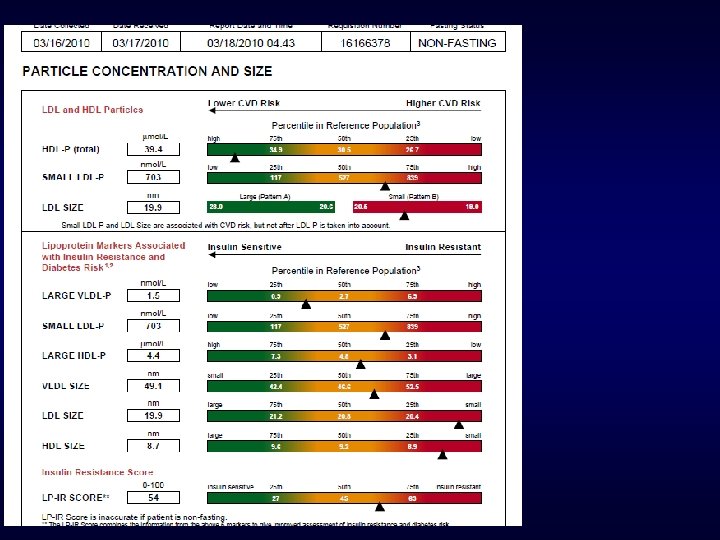
ML Sept 2009 F Wt: 263 (133 pound weight loss!) over 9 months time F BMI 34. 69 WC 41 inches (lost 23 inches) F BP 120/80, pulse 88 F Hg. AIC 5. 2 F Glucose 68

March 2010 Weight loss maintained. March 2009

45 yr Female Dyslipidemia Excellent Diet and Exercises Daily

45 yr Female Dyslipidemia F Lipids • Total Cholesterol • LDL-C • HDL-C • Triglycerides Fasting Glucose F BP F BMI F Treatment options? F 250 150 56 220 120/82 25

AHA Guidelines for CVD Prevention in Women Clinical Recommendations Major Risk Factor Interventions F Lipids - Lipoproteins: • Optimal levels of lipids and lipoproteins in women: • LDL-C < 100 mg/d. L • Triglycerides < 150 mg/d. L • HDL-C > 50 mg/d. L • Non HDL-C < 130 mg/d. L Mosca, L. et al. Circulation 2004; 109: 672 -693

AHA Women’s Guidelines for Lipid Management n Initiate TLC for all women, regardless of risk level – – – Intermediate Risk Initiate statin if LDL-C ≥ 130 mg/d. L on TLC Initiate niacin or fibrate for low HDL-C, after LDL-C goal is reached Initiate niacin or fibrate for high non–HDL-C, after LDL-C goal is reached – – – High Risk Initiate statin if LDL-C ≥ 100 mg/d. L concomitant with TLC Initiate niacin or fibrate for low HDL-C Initiate niacin or fibrate for high non–HDL-C Mosca L, et al. Circulation. 2004; 109: 672 -693.

LDL-P 2552 Small LDL-P 1882 Treatment options: Lifestyle Statin Niaspan Fibrate Combination Metformin TZD Others
 brought LDL-P down 1068 points?")
2 Months later What treatment (s) brought LDL-P down 1068 points?
 brought LDL-P down 1068 points? 1. Statin monotherapy 2. Combo therapy")
What treatment (s) brought LDL-P down 1068 points? 1. Statin monotherapy 2. Combo therapy with statin plus 3. Niacin 4. Fibrate 5. Metformin
 brought LDL-P down 1068 points? 5 pound weight")
2 Months later What treatment (s) brought LDL-P down 1068 points? 5 pound weight loss & Metformin ER 1000 mg/day

63 yr Diabetes on meds LDL c 70, normal HDL C and triglycerides on Simvastatin 40 mg Twin brother died this year of MI Is there residual risk?

RESIDUAL RISK NOTED LDL c 70 Trigs 69 HDL C 46 Non HDL C 84 LDL p not <700

H. L 68 yr WM prior Stroke F BP: 130/85 F PMH: CVA (Stroke = cardiac risk equivalent) • No lipid meds • LDL cholesterol at goal 70

H. L. NMR lipoprofile no meds F F F F F LDL particle 1879 (optimal <700 -1000) Small LDL p 1870 LDL cholesterol 70 HDL 36 Triglyceride 273 Total chol 161 LDL particle size Pattern B Large HDL p 4. 1 intermediate risk Large VLDL p 10. 4 High risk TSH, CMP normal

Follow up NMR 1 month later Simvastatin 40 mg Omega 3 fish oil 4 grams LDL particle was 1879 now 1115 LDL cholesterol was 70 now 53 Hg. AIC 5. 9

What treatment do you advise now along with Diet and Exercise? F 1. no further treatment F 2. Increase Simvastatin to 80 F 3. Add Metformin F 4. Add Fibrate F 5. Add Niacin

78 yr old WF hypercholesterolemia on Simvastatin 20 mg primary prevention LDL c 122 HDL and Triglycerides optimal

78 yr old Primary Prevention LDL 122 F 1. Increase simvastatin dose F 2. Switch to alternative more potent statin F 3. Do nothing F 4. Add Fibrate F 5. Add Niacin F 6. Add Bile Acid Sequestrant

LDL Particles 1083, LDL C 122 Tx? F 1. Increase simvastatin dose F 2. Switch to alternative statin F 3. Do nothing LDL P close to goal <1000 F 4. Add Fibrate F 5. Add Niacin F 6. Add Bile Acid Sequestrant

Pediatric Obesity

Pediatric Case 11 yr old Obesity

Pediatric Obesity F PMH: Metabolic syndrome diagnosed by Pediatrician F Fam hx: Mom hypothyroid, GDM, Father hypertension, Mgma hypothyroid, diabetes F Vital Signs: Ht: 62. 25 in. Wt: 191 lbs. BMI: 34. 65 BP : 122 / 82
 F Small LDL P 1231")
Labs Pediatric Obesity F LDL Particles 1775 (optimal <1100) F Small LDL P 1231 F Total Cholesterol 206 F HDL 45 F LDL 137 (optimal <110) F Trig 119 F IR Score 78

Labs Pediatric Obesity F Insulin 14, Hg. AIC 6. 0; glucose 75 F CRP 3. 2 (optimal <1) F TSH 2. 71, Anti TPO Antibodies 832

Treatment F Thyroid treated with Levothyroxine 0. 05 mg/day F Insulin resistance treatment: • diet, exercise and Metformin ER 1000 mg/day F 1 year later……. .

1 year later after 53 pound wt loss

1 yr later 53 pound weight loss, Metformin

69 yr Female with Familial Combined Hypercholesterolemia prior CVA and statin intolerance

High risk Hx: CVA F 69 y/o Fe with Hypercholesterol X 15 yrs F PMH: HTN, Hypothyroid, Rheumatoid Arthritis F No lipid meds due to statin intolerance: myalgias, resistance to meds F Medication Synthroid, MTX, ASA F FH CAD >age 75

Initial Labs and Plan F LDL-P 3434, small LDL-P 2095 F TRG 238, HDL 76, LDL-C 263 F Very high vascular inflammation: Lp. PLA 2 465 (optimal <200) F LDL P convinced her to trial medications F Started Rosuvastatin 5 mg, Ezetamibe 10 mg, Omega 3 FA 4 G and TLC

Statin Tolerabilty Issues with RA F Due to myalgias/cramping, case discussed with rheumatologist F Supplementation with Co Q 10 and vitamin D 3 improved tolerability

1 yr later Insulin Resistance noted F Hg. AIC 6. 0, Glucose 101, LDL P 1620 , small LDL P 1139 (borderline high) F TLC made with hydrotherapy and treadmill exercise F Reduced high-glycemic carbs and increased omega 3 F Metformin 500 BID added

Dramatic Risk Reduction Achieved! 8/15/06 Intolerant to statins no meds 7/11/07 Rosuvastatin 5, Ezetamibe 10, Omega 3 4 Vit D 3, Co Q 10 7/16/08 Rosuvastin 5, Ezetamibe 10, Omega 3 4 Metformin 1000 Total Cholesterol 384 208 153 Triglyceride 238 74 88 HDL-C 76 70 74 LDL-C 263 123 62 LDL-P Small LDL P 3434 2095 1620 1139 958 781 Non HDL-C 308 158 82 Lipoprotein (a) mg/dl (optimal <30) 30 `Lp. PLA 2 465 161

LDL particles/Apo B for Risk Management • When you have reached goals on traditional lipid panel in high risk patients check LDL P or Apo B • High risk family history: LDL Particle concentration or Apo B may help ascertain risk not seen in traditional lipid panel

2 New Patient referrals Secondary Prevention 3/16/2010 F Both patients recent Myocardial Infarction referred for lipid treatment and work up genetic etiology F Both patients on Moderate dose stain at time NMR drawn

Consult #1 Secondary Prevention on statin LDL cholesterol 57 At NCEP goal LDL Particle very High risk 1835 (Optimal <700) Discordance Additional Therapy needed

Consult #2 Secondary Prevention on statin LDL cholesterol 60 at NCEP Goal LDL Particle Concentration 1006 Also at Goal No further treatment needed

Same Day 2 Consults Completely different decision making based on NMR results

58 yr WF strong Family History Normal Lipid panel

58 yr old F Fam hx Mother CABG age 53, Sister CABG age 52 F Lipid panel Feb 2007 • Total cholesterol 250 • HDL-c 116 • LDL-c 110 • Triglyceride 29 • Non HDL 134

What is her risk? Family history, age >55 Framingham 3 %

2 months later F Chest pain F F Diagnosed GERD placed on PPI Lipids: cholesterol 259, Trig 42, HDL 90, LDL c 136, chol/HDL 2. 9 F 2 weeks later……atypical chest pain, abnormal EKG F 70 % Left Main disease, CABG severe 3 vessel F Started on Atorvastatin 40 mg, omega 3 1 gram OTC, Plavix post op

58 yr old recent CABG 3 weeks later in lipid clinic May 2007 on Atorvastatin 40 mg and Omega 3, 1 g F Lipid Panel • Total Cholesterol • LDL c • HDL c • Triglyceride 203 141 44 89 • Lipoprotein (a) 76 mg/dl (elevated >30 mg/d. L)
 F TSH 0. 57 normal F hs. CRP")
Other labs (On Atorvastatin 40 mg) F TSH 0. 57 normal F hs. CRP 47 very high F CMP ALT 80 (elevated) , AST 34, Alk. Phos 162 F NMR?
 high 76 mg/dl")
LDLpart icle 3002 Lp (a) high 76 mg/dl

4 months: Rosuvastatin 40, Omega 3 - 2 g F Wt 136. 5 down 9. 5 pounds F BMI 25 F 126/74 pulse 80
 Add Niacin 500")
Rosuvastatin 40 Omega 3 - 2 g High Lp (a) Add Niacin 500

6 months later on Niacin 500, Rosuvastatin 40 F F F F F LDL p 965 Small LDL p 661 LDL c 86 Previous 3002 on Atorva 40 Previous 3002 Previous 140 Total HDL p 25 large 18. 5 (optimal >4) HDL c 152 Previous 40 Total Chol 250 Triglycerides 60 Apo B 72 CMP normal

1 year later F Medications: Rosuvastatin 40 mg, Niacin 1000 mg, Omega 3 -1 g F Lipid panel • Total Cholesterol 252 • LDL- C 129 • HDL –C 111 • Triglycerides 59

LDL c 129 on Rosuva 40 and Niaspan 1 g 1. Increase Niaspan 2. Add Zetia 3. Add fibrate 4. Add Bile acid Sequestrant 5. Nothing

On Rosuva 40 mg Niacin 1000 mg Omega 3 1 g Vitamin D 3 5000 LDL-P 616 LDL-C 129 Lipoprotein (a) 63

LDL c 129 with LDL Particle 616 on Rosuva 40 and Niaspan 1 g 1. Increase Niaspan 2. Add Zetia 3. Add fibrate 4. Add Bile acid Sequestrant 5. Nothing

Lipoproteins Pre and Post treatment NO Medication Atorvastatin 40. 1 year later Pre CABG OM 3 Rosuvastatin 40, Niaspan 1 g, OM 3 Total Cholesterol 250 203 252 Triglyceride 29 89 59 HDL-C 116 44 111 LDL-C 110 141 129 3002 616 159 141 76 63 LDL-P Non HDL-C Lipoprotein (a) mg/dl (optimal <30) ` 134

Comparison of 2 43 year old white females Both high HDL, no Family History Heart Disease

What does the lipid panel tell us about these women’s risk for heart disease? F C. H. 43 yrs F D. L. 43 yrs F Lipid panel F Lipid Panel F Total chol 251 F Total chol 232 • LDL 130 • HDL 88 • HDL 82 • Trig 166 • Trig 101 • Tchol/HDL 2. 9 • Tchol/HDL 2. 8 • Non HDL 163 • Non HDL 150 • Framingham 2. 2% • Framingham 2. 1%

2 very different LDL particle concentrations F C. H. NMR High Risk F D. L NMR Low Risk

LDL C goal <100, LDL P goal <1000 LDL C goal <100 Requires 22% reduction Alternative measure of LDL : LDL Particle goal <1000 requires 64% Reduction of LDL P to get to goal

Office visits two women same day Primary prevention Lets assess their cardiovascular risk

2 women One Day in May F BK F 45 yr old BMI 29, 120/72 Total chol 154 F LDL c 71 F HDL c 70 F Triglyceride 64 F LDL particle size B F LDL particle # F • LDL p 1042 F JS F 41 yr old BMI 29, BP 122/78 Total chol 165 F LDL c 74 F HDL c 71 F Triglyceride 98 F LDL particle size B F LDL particle # F • LDL p 2102

BK 45 yr WF JS 41 yr WF

JS age 41 Does not meet criteria for Metabolic syndrome Normal Triglyceride, normal HDL Normal BP 122/78 Has increased waist circumference 36 inches 1/5 clinical criteria NMR shows markers of metabolic syndrome 2007 Hg. AIC 5. 4 2008 fasting glucose 107

Conclusions: LDL Particle/Apo B for Risk Assessment Primary Prevention: risk stratify more accurately, target therapy appropriately Avoid overtreatment of high LDL –C when LDL P optimal Pediatric patients : better assess who should be treated more aggressively with statins

Risk Management Patient Compliance with therapy: Bigger numbers instill more fear Identify Metabolic syndrome/Insulin resistance before traditional tests become abnormal Its our “window into Diabetes” Target therapy based on whether Metabolic markers present or not

Risk Management Clinical Pearl Combination drug therapy fixes LDL Particle elevations more then high dose statinmonotherapy

Questions? taradall@advlip. com www. advlip. com
- Slides: 99