Managing fibromyalgia in Stockport Jayne Little Rheumatology Consultant
 Jayne Little Rheumatology Consultant SHH")
Managing fibromyalgia (in Stockport) Jayne Little Rheumatology Consultant SHH

Outline Diagnosis • What is fibromyalgia • Diagnostic criteria Resources available • GP and patient info • Useful phrases – And how to diagnose Management • Guidelines on management – And how to manage • Relevant services in Stockport Session being recorded

Hello! Our services Abbas Ismail Charlotte Filer – GCA – EIA – Specialty Louise Mercer • • Ultrasound Psoriatic arthritis SLE / CTD Osteoporosis – Routine referrals • >1/3 fibromyalgia Qasim Akram Hiba Bacha


We are committed to supporting the diagnosis and management of fibromyalgia in Stockport

Diagnosing Fibromyalgia

What is fibromyalgia? • Chronic widespread pain – Heightened pain response / allodynia – Bones / joints / muscles – Debilitating / distressing • • Sleep disturbance and fatigue Cognitive disturbance Anxiety and depression Headaches / Paraesthesia / IBS / urinary symp

Why diagnose fibromyalgia? Aid patient’s understanding Avoid inappropriate investigations, referrals & treatment Instigate treatment

Steps in diagnosis Understand FM Suspect FM Convince yourself: Confirm FM Exclude anything else Convince the patient

Understanding FM Academic understanding Personal understanding

Fibromyalgia is a real clinical entity The pathophysiology is incompletely understood The patient’s pain is very real

Epidemiology • • • 2 -5% prevalence Strong association with anxiety & depression 25% in inflammatory arthritis and CTD 1: 6 male: female Delay between symptom onset and diagnosis Ave 3. 7 consultations before diagnosis

1990 ACR classification criteria

2016 ACR diagnostic criteria • Meet threshold on: – Widespread pain index – Symptom severity score

2016 ACR criteria
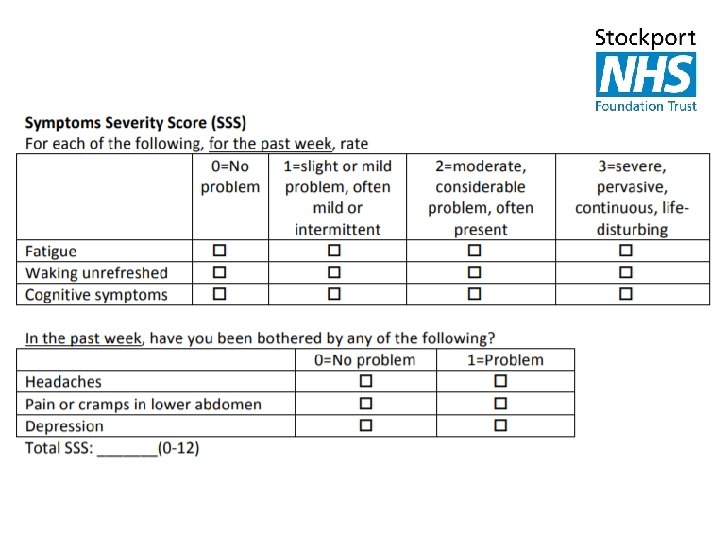

2016 ACR diagnostic criteria • Meet threshold on: – Widespread pain index – Symptom severity score • Pain in 4+ of 5 regions • Symptoms present >3 months Diagnosis is valid irrespective of other diagnoses

Fibromyalgia is NOT a diagnosis of exclusion
 • Thorough examination (make")
What do I do • Listen, Listen (inc review list) • Thorough examination (make this explicit) – Joints – Neurological exam • muscle bulk, asymmetry, function • sensation – Tender points

Differential diagnosis There are very few conditions that cause chronic widespread pain with normal investigations and normal examination

Differential diagnosis Investigation Examination Connective tissue disease ANA PMR ESR / CRP Infection ESR / CRP Thyroid / endocrine TFTs / U&E / bone prof Arthritis (inflammatory) RF / anti-CCP Swollen JOINTS Muscle disease CK Important Cancer FBC / LFTs Do not order vitamin D

What do I do? Investigation Examination Connective tissue disease ANA PMR ESR / CRP Infection ESR / CRP Thyroid / endocrine TFTs / U&E / bone prof Arthritis (inflammatory) RF / anti-CCP Swollen JOINTS Muscle disease CK Important Cancer FBC / LFTs Ensure all done since symptoms started

What do I say? • • • Clear and positive diagnosis Explanation of pain processing Your problem is in your brain Your pain is real and not ‘in your head’ It is an important distinction – We can target treatment appropriately – You will not damage your joints through exercise

What should you do? I am not a GP / physio / nurse Very dependent on the patient

What could you do? • • Make suggestion early and don’t apologise ? Use the 2016 criteria Full symptom history and examination Request investigations – FBC / U&Es / LFTs / Bone / TFTs / CRP / ESR – RF / CCP / ANA / CK with caution • Explanation and planning - resources

What should you say? • What you believe / feel comfortable saying • Things to avoid: – Psychosomatic – Low pain threshold – Unable to find any other explanation

Management of fibromyalgia

2016 EULAR Guidelines Optimal management requires prompt diagnosis and provision of information, including written information.

2016 EULAR Guidelines Optimal management requires prompt diagnosis and provision of information, including written information. Pain / function / psychosocial context Goal Improved Qo. L Focus on non-pharm therapies

Aim is not to eliminate pain Expectation setting is essential

Specific treatments • The ONLY intervention with strong evidence for is exercise (strengthening or aerobic) • Weak evidence for: – CBT – Acupuncture / hydrotherapy – Meditative movement / mindfulness

Pharmacological treatments All have weak evidence base • Amitriptyline • Pregabalin • Duloxetine • Tramadol

Management recommendations as flow chart. G J Macfarlane et al. Ann Rheum Dis 2017; 76: 318 -328 © 2017 by BMJ Publishing Group Ltd and European League Against Rheumatism

Management recommendations as flow chart. G J Macfarlane et al. Ann Rheum Dis 2017; 76: 318 -328 © 2017 by BMJ Publishing Group Ltd and European League Against Rheumatism

Management recommendations as flow chart. Versus Arthritis website FMA UK website Patient information letter G J Macfarlane et al. Ann Rheum Dis 2017; 76: 318 -328 © 2017 by BMJ Publishing Group Ltd and European League Against Rheumatism

Management recommendations as flow chart. G J Macfarlane et al. Ann Rheum Dis 2017; 76: 318 -328 © 2017 by BMJ Publishing Group Ltd and European League Against Rheumatism

What do I say? • • Aim: Reduce pain and improve Q of L The cause is multi-factorial The treatment needs to be multi-factorial The treatment has to be patient led – This is hard • Sleep • Exercise Mental health

What do I say? • • Aim: Reduce pain and improve Q of L The cause is multi-factorial The treatment needs to be multi-factorial The treatment has to be patient led – This is hard • Sleep • Exercise Mental health Drugs

Services in Stockport • • • Physical Activity Referral in Stockport Healthy Minds Stockport Expert Patient Programme Health and Wellbeing College Stepping Hill Pain Clinic ?

Who to refer to secondary care? • When it doesn’t fit – Pain not widespread – No sleep or mood disturbance or precipitant – ANY SOLID objective pathology • When the patient remains unconvinced • Rheumatology / Neurology / Pain / Psychiatry

How can we help you? • Advice and guidance • Information to patient – Letter – Patient info videos • Diagnosis in difficult patients: – Other possible diagnosis – Patient not accepting of diagnosis Please make reason for secondary care opinion explicit We can not help with management of fibromyalgia
")
? Jayne. little@stockport. nhs. uk 0161 419 5049 (Wed – Fri)
- Slides: 43