Managing Chronic Pain 2018 Biofeedback Clinical Update with

Managing Chronic Pain: 2018 Biofeedback Clinical Update with Bill Dougherty, Psy. D, CPS

Agenda n n Welcome 1: 00 -1: 15 Opening Remarks. Program Overview Brief Introductions Participant Backgrounds Pre-Test

Agenda n n n n n 1: 15 -2: 15 Assessing Psychological Factors Associated with Chronic Pain P 3 Pain Patient Profile Measuring Anxiety, Depression, & Somatization Clinical Recommendations Mc Gill Pain Questionnaire Assessing Nature & Quality of Pain & Mechanisms Development of Treatment Plan for Chronic Pain & Opioid Abuse 2: 15 - 2: 30 Break 2: 30 - 4: 00 Biofeedback and Demonstration
 n n Substance Use Disorder is chronic Disorder (Disease) characterized by")
Addiction Defined (SUD) n n Substance Use Disorder is chronic Disorder (Disease) characterized by drug misuse/abuse, drug craving, preoccupation, seeking a drug, and frequently abusing a drug despite the evidence of adverse consequences. And. . . Continued use despite Social, Legal, Physical, Psychological, and other adverse events.

Denial n n n n Rationalization Justification Minimizing Avoidance Dishonesty Blaming others The addict is using to attain Drug Euphoria

Pain Defined: n n An unpleasant sensory and emotional experience which is caused by tissue injury damage, or dysfunction and produces within the individual, some impairment in level of physical and psychological functioning. There exist assessments used to quantitatively and qualitatively assess pain.

Analgesia n n n Pain patients without a history of substance abuse generally use medication (opioids) as directed for pain relief UNTIL tolerance develops. Therapeutic Dependence Defined Some patients with pain may not be attaining an adequate level of analgesia. Pseudoaddiction –the clock watchers Patients may exhibit indicators more or less predictive of addiction disorder.

Visual analog pain scales n n Two types used in practice O to 10 point Scale with O=mild pain annoying/nagging and 5=distressing, miserable, agonizing and 10=unbearable, torturing.

5 point Visual analog Scale n n n n Correlates with the Mc. Gill pain Questionnaire More descriptive more precise O = no pain 1 = mild 2 = discomforting 3 = distressing 4 = horrible 5 = excruciating

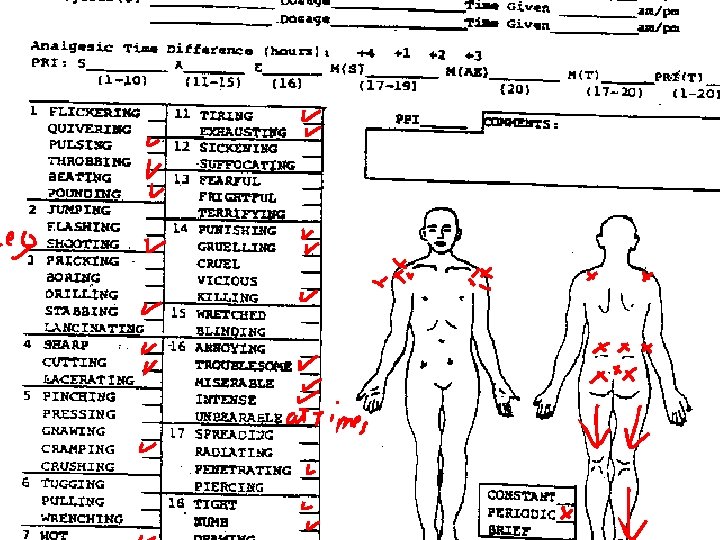
Mc. Gill pain Questionnaire n n n Assists in giving both patients and the Clinician a more accurate assessment of the nature, location, and quality of pain. Patients usually do not have the language to describe their pain Pain is subjective. It is important not to Compare your patient with others who are experiencing pain

n Afternoon Break We will resume in ten minutes.
")
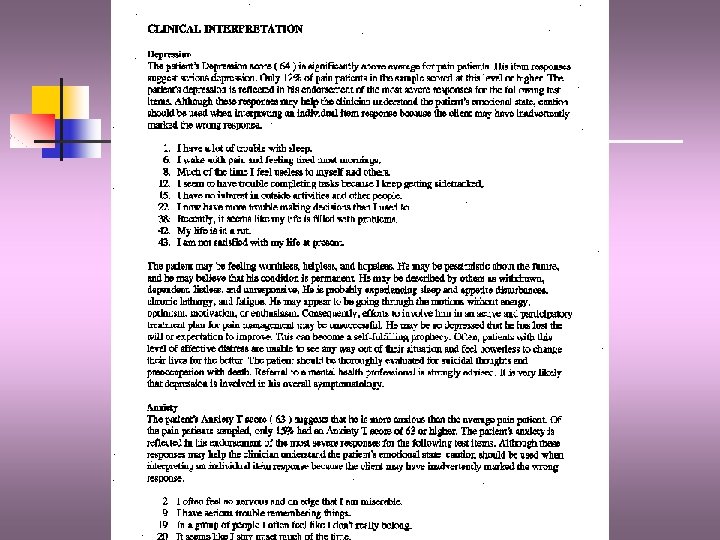
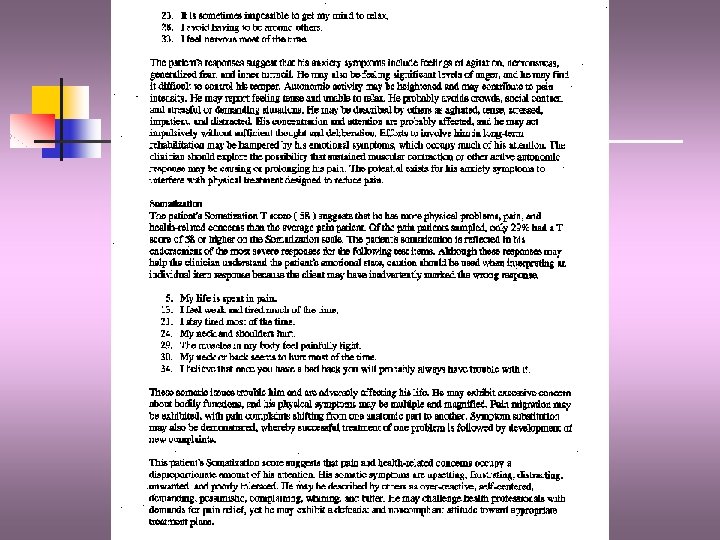
Assessing psychological factors n n n Depression Anxiety Somatization Check for pre-existing disorders (pre-pain) Dual Diagnosis Triple Diagnosis we need to be specific as to what we are talking about. Pain and addiction can be dual diagnoses

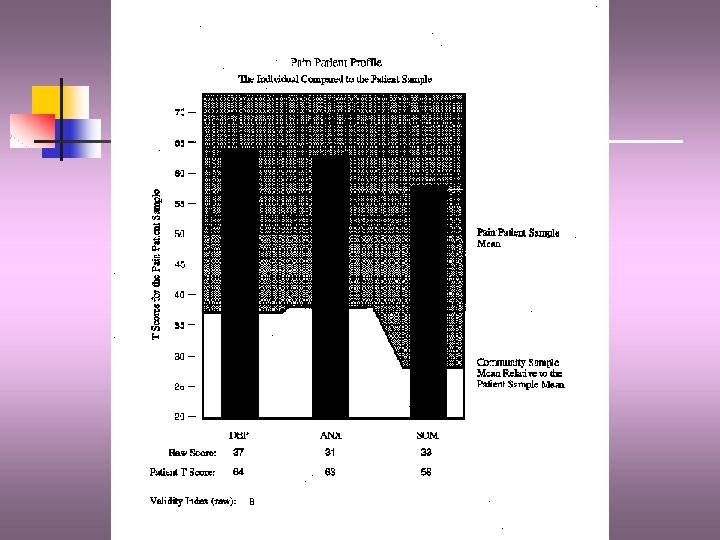
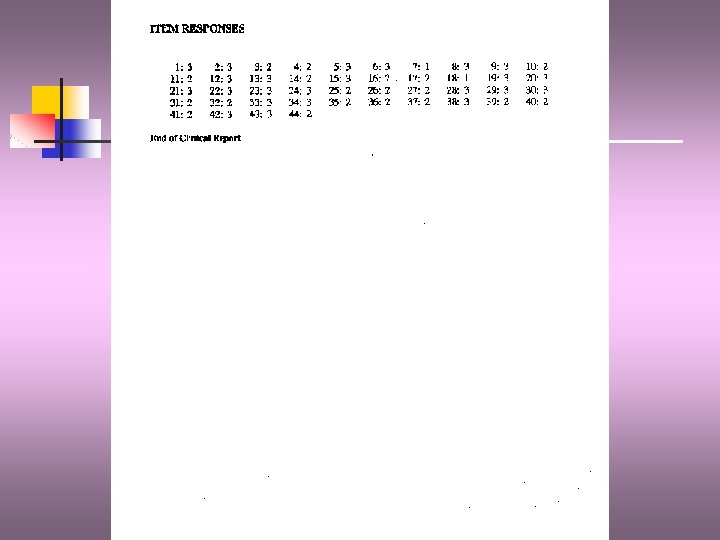
P 3 -pain Patient profile n n Designed specifically for use with chronic pain patients Measures levels of anxiety, depression, and somatization (excessive focus on pain or other somatic complaints) Reliability and Validity Administered in 50 min session.

Multi modal pain Management n n n Current Trends in Pharmacology 4 pain mechanisms: transmission, transduction, perception. and modulation Target each mechanism with various TX’s including drugs without an abuse liability
, oxycodone (percocet/oxycontin), morphine, hydrocodone (vicodin, norco), opana,")
Pharmacology n n Mu agonists: Heroin (diacetlymorphine), oxycodone (percocet/oxycontin), morphine, hydrocodone (vicodin, norco), opana, fentanyl. Mixed agonists: methadone, Suboxone (buprenorphine). Stadol NS (butorphanol) Mixed agonists/antagonists: pentazocine w/naloxone (Talwin NX) and levorphanol tartrate

Pharmacology n Newer Anti Depressants: SSRI’s: Prozac, Paxil, Zoloft, Celexa, Lexapro. All work on serotonin systems. Luvox & Effexor- SNRI’s and Wellbutrin, a dopamine enhancer. Cymbalta (duloxetine), is a novel antidepressant originally designed for use in diabetic neuropathy.

Pharmacology n n n Tricyclic antidepressants: Elavil, Pamelor, Tofranil. Europe: Stablon—tianeptine. Designed to enhance the quality of sleep. Neuroprotective Trazadone is also effective What about Tramadol? Ultram contraindicated in pts with history of seizure or concominant use of tricyclic antidepressants, and in pts w/history of opioid abuse. The metabolite is a mu receptor agonist.
 Ketoprofen (Orudis) Relafen")
Pharmacology n n n NSAID’s non-steroidal anti- inflammatory drugs Ibuprofen (Advil/Motrin) Ketoprofen (Orudis) Relafen Ketorolac=Toradol Naproxen sodium-Anaprox Daypro Voltaren (diclofenac) Indomethacin (Indocin) Dolobid Tolectin

Pharmacology n n n Cox-2 inhibitors Block prostaglandin E-2 at the cycloxygenase site. Celebrex Mobic (meloxicam) Works on transduction mechanism Some pts. may require Histamine H 2 antagonists prilosec, zantac, protonix
 Topomax")
Pharmacology n n n n Anti-seizure Drugs Gabapentin Lyrica (does have abuse liability) Topomax Lamictal Dilantin Tegretol n Burning, sharp, shooting pains

Pharmacology n n n n Avoid use of benzodiazepines ex: diazepam, ativan, xanax, klonopin, etc. Buspirone (Buspar-good choice for tx anxiety) Caffeine (migraines, pros/cons) Nicotine, a stimulant elevates BP Baclofen - only muscle relaxant approved Ethyl Alcohol - rebound pain Stimulants ADD meds provigil, methylphenidate (concerta) adderal. Corticosteroids
 Ketamine infusion NMDA")
Pharmacology n n Lidocaine infusion or Lidoderm patch Duragesic patch (fentanyl) Ketamine infusion NMDA receptor antagonists n n Memantine Mechanism of action Role of aspartate and glutamate Problems with mu agonist drugs-oxycodone, hydromorphone (Dilaudid) and hydrocodone.
 Chiropractic")
Alternatives Nonpharmacological n n n Spinal cord stimulator TENS Intrathecal pumps (morphine, baclofen) Chiropractic Physiatry—Physical medicine/therapy massage, accupressure Heat/Cold applications, aquatic exercise

WHAT IS BIOFEEDBACK? n Biofeedback is a method for learned control of physiological responses of the body. These responses can be either in the voluntary system, such as skeletal musculature, or in the involuntary, or autonomic nervous system, such as heart rate, vascular responses (frequently indirectly measured as temperature), and sympathetic discharges (measured by the electrical skin response).

WHAT IS BIOFEEDBACK? n n n n Clinical biofeedback is used successfully in the following applications: Anxiety disorders Mild depression Epilepsy Headaches Concentration improvement for education and meditation Control of brain waves for spiritual development and inner tranquility Musculoskeletal disorders involving chronic muscle tension Relaxation therapies Stress management techniques Neuromuscular re-education of gait mechanics Chronic pain syndromes High blood pressure Asthma

HOW DOES AVS BIOFEEDBACK WORK? n Auditory Visual Stimulation or AVS biofeedback equipment, comes in a number of forms and flavors. The most well-known and effective measure the brain's electrical activity and then pulse lights and sounds to control that activity. Such devices, through flickering lights and precisely controlled rhythmic tones, stimulate and synchronize the hemispheres of the brain while entraining the brain wave frequencies into desirable states of consciousness. The study of these brainwave patterns, the summation of the brain's electrical activity, as represented by electroencephalography EEG), has led scientists to the discovery that different brainwave patterns are associated with different states of awareness.

HOW DOES AVS BIOFEEDBACK WORK? n n n Four main brainwave patterns have been recognized: Beta Waves 13 - 30 Hz Alert state Alpha Waves 8 - 12 Hz Relaxed wakefulness Theta Waves 4 - 7 Hz Imagery Delta Waves. 5 - 3 Hz Deep sleep

Biofeedback n With the relief of tension/stress/resistance in the body/mind, the user becomes receptive to information from "inside" and "outside" essential to fundamental change. Spoken words during certain L/S session will embed in deep layers of the user's consciousness to change thoughts, feelings and behavior automatically. The clinician’s digitally mastered voice has an amazing effect when combined with an individually developed AVS biofeedback program. Statistically, 72 percent of individuals receiving biofeedback are helped significantly; 20 percent moderately; and 8 percent marginally.

Biofeedback n By stimulating balanced, abundant neurotransmitter production, expanding neural pathways, and programming desirable, ecologically sound behaviors, AVS biofeedback can enhance physical healing and homeostasis, intellectual performance (creativity/IQ attentional flexibility), and greatly improved sense of well-being long after the session.

Biofeedback n The state of deep rest and hemispheric balance possible with AVS technology can rejuvenate the body/mind and have lasting effects in every area of one's life. To understand how this technology works, individuals are encouraged to schedule an initial session with a clinician who is trained and certified in biofeedback applications. The first session generally will include gathering a complete history and reviewing school or medical records. A sample introductory session will be provided and the individual will experience the results. For additional information regarding AVS biofeedback, or to schedule an appointment please call Bill Dougherty directly at 570 -480 -6140 for a personal response.
; Carroll, Douglas, Biofeedback in Practice")
References n Bibliography: Benjamin, John V. , Biofeedback (1999); Carroll, Douglas, Biofeedback in Practice (1984); Green, Elmer and Alyce, Beyond Biofeedback (1989); Hatch, J. P. , et al. , eds. , Biofeedback: Studies in Clinical Efficacy (1987); Jones, Marcer, Donald, Biofeedback and Related Therapies in Clinical Practice (1986); Richter-Heinrich, E. , and Miller, N. E. , Biofeedback (1982).

Chronic Pain and Addiction Clinical Update n n n Demonstration Summary and Conclusions Post-Test

Review of Objectives n n n 1. Recognize identifiable differences between opioid “addiction” versus “therapeutic dependence” in the treatment of chronic pain. 2. Identify situational, psychological, and physiological factors that distinguish addicts and non-addict patients. 3. Become familiar with comprehensive assessment instruments and methods to assist the clinician in the recognition of chronic painful conditions and addiction; specifically The Mc. Gill Pain Questionnaire, Two-Tier Pain Inventory, and P 3 Pain Patient Profile. 4. Define concepts including pseudoaddiction, iatrogenic addiction, pharmacological dependence, opiophobia, CAGE and Trauma Tests. 5. Estimate the likelihood of the development of narcotic addiction in a chronic pain patient with and without a history of substance abuse.

Review of Objectives n 6. Identify aberrant drug related behaviors that raise concern about the potential for addiction in medical patients prescribed opioids for chronic painthose that are more predictive of addiction and those that are less predictive. n 7. Become familiar with pain mechanisms including transmission, transduction, modulation, and perception. n 8. Recognize alternative approaches to the treatment of chronic pain focusing on a multidisciplinary approach including physical and psychological modalities. n 9. Be cognizant of alternative novel pharmacological approaches to pain management including NSAIDS, antidepressants, anticonvulsants, and interventional treatment strategies. n 10. Be knowledgeable of guidelines concerning prescribing and administering drugs with abuse liability with the addict in recovery. n 11. Identify physical pain as a relapse trigger and develop strategies for effective management to reduce the possibility of returning to active use.

A. Primary Problem: Behavioral Definitions Chronic Pain • Physical discomfort or distress of at least three months' duration. • Screaming, moaning, or phrases suggesting suffering (e. g. , "Oh, oh, " "I have such a terrible headache today, " "My back is killing me") apparently associated with physical sensation. • Grimacing or other facial expression suggesting physical discomfort and suffering. • Tensing or withdrawing body part in anticipation of or reaction to physical distress. • Refusal to engage in activity because "it hurts. " • Decreased activity level attributed to physical discomfort, resulting in poor physical strength and endurance. • Reduction (or complete loss) in ability to engage in normal social, vocational, and recreational activities because of physical distress. • Relationships dominated or strongly influenced by pain. • Excessive use of over-the-counter analgesics. • Increased tolerance and perceived need for narcotic medication. • Use of street drugs or illegal substances with intent to decrease physical discomfort.

Long Term Goals • Reduce physical discomfort and emotional suffering to tolerable levels. • Refrain from frequent verbalizations or other communications about level of physical distress and suffering. • Participate in necessary and routine activities despite discomfort. • Maintain physical fitness through regular exercise suited to physical capabilities. • Manage activity level and energy expenditure to allow for participation in a variety of work, social, and recreational activities. • Reduce or terminate dependence on narcotic medications while utilizing medications that reduce pain according to physician's recommendations. • Identify and utilize benign interventions (e. g. , heat, relaxation, transcutaneous neural stimulation) effectively to increase comfort level. • Become knowledgeable, active, and self-reliant in managing pain.

Thank you, and have a nice day! n n n A copy of today’s training is available for download on my website. William F. Dougherty, Psy. D. , NCP My Clinical Office located at: 301 West Grove St. Clarks Summit, PA www. drdougherty. org Tel: 570 -480 -6140 Copyright 2018 William F. Dougherty, Psy. D. , NCP
- Slides: 47