Managing Chronic Kidney Disease in the Elderly Veteran









 Pitt B, Zannad F, Remme WJ, et al. The")



 • 10, 251 adults with established")

 Stages by Age Group in NHANES 1988 -1994")













 (A), combined outcome of doubling of serum creatinine")

 Stages by Age Group in NHANES 1988 -1994")












- Slides: 46
Managing Chronic Kidney Disease in the Elderly Veteran Ann M. O’Hare, MA MD Staff Physician, VAPSHCS Assistant Professor of Medicine University of Washington
For Ann O’Hare’s financial disclosure statement: http: //depts. washington. edu/greccva/OHare_Disclosure. doc
Generalizability of RCTs Gross, C. P. et. al. Ann Intern Med 2002; 137: 10 -16
RCTs in high impact medical journals Van Spall, JAMA 2007
Mean age of participants in heart failure trials Heiat et al, Archives of Internal Medicine, 2002
Exclusion criteria of heart failure trials
Acute MI • A total of 214 trials met inclusion criteria, involving 150, 920 study subjects. • Over 60% of trials excluded persons over the age of 75 years. • Studies published after 1980 were more likely to have age-based exclusions compared with studies published before 1980 Gurwitz, JAMA, 1992
Cancer treatment trials Hutchins, NEJM 1999
Exclusion of elderly in clinical trials • National Institutes of Health Revitalization Act of 1993 (Public Law 103 -143) – Requirements for the inclusion of women and minorities in clinical trials but not the elderly
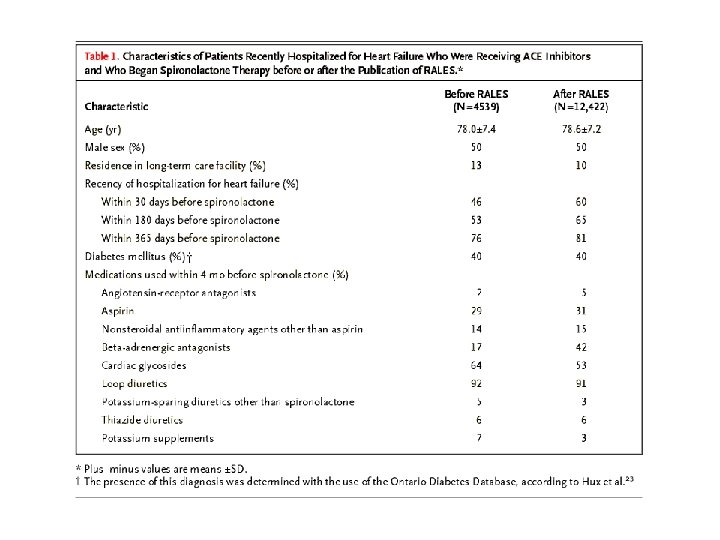
Randomized Aldactone Evaluation Study (RALES) Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med 1999; 341: 709 -717. [
Rates of spironolactone prescription Juurlink et al. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med. 2004 Aug 5; 351(6): 543 -51.
Rates admission for hyperkalemia
Rates of death
Action to Control Cardiovascular Risk in Diabetes (ACCORD) • 10, 251 adults with established type 2 diabetes • Aged 40 to 82 (average 62) • had diabetes for an average of 10 years • either already had diagnosed CVD or they had at least two CVD risk factors.
Chronic kidney disease Levey et al, Annals of Internal Medicine, 2003
Prevalence of Chronic Kidney Disease (CKD) Stages by Age Group in NHANES 1988 -1994 and 1999 -2004 Coresh, J. et al. JAMA 2007; 298: 2038 -2047. Copyright restrictions may apply.
CKD is common in the elderly.
In VA 75 -85 group is largest Adapted from O’Hare et al JASN 2007
High prevalence of comorbidities
Practice guidelines
Framework • Can existing guidelines for the management of CKD be generalized to these older patients? – What is the strength of evidence? – Does the evidence pertain specifically to older patients with CKD? • What are the characteristics of patients enrolled in clinical trails? – If not, can the available evidence reasonably be extrapolated to older patients? • Is there any reason to expect that real and perceived benefits of an intervention might differ by age? – Does CKD have similar features in older and younger patients? – Does CKD have similar clinical implications in older and younger patients? • Are the risks of the intervention comparable in older and younger patients? – Do the adverse effects of the intervention differ by age? – Do similar adverse effects have different implications for older and younger patients?
What is the quality of the evidence?
Early treatment can make a difference 100 No Treatment Current Treatment GFR (m. L/min/1. 732) Early Treatment 10 Kidney Failure 0 4 7 Time (years) 9 11
“Strong” evidence: the example of ACE inhibitors • Patients with diabetic kidney disease, with or without hypertension, should be treated with an ACE inhibitor or an ARB ACE inhibitors and ARBs are effective in slowing the progression of kidney disease with microalbuminuria due to type 1 and type 2 diabetes (Strong). • ACE inhibitors, ARBs, and nondihydropyridine calcium-channel blockers have a greater antiproteinuric effect than other antihypertensive classes in diabetic kidney disease (Strong). • Patients with nondiabetic kidney disease and spot urine total protein to creatinine ratio ≥ 200 mg/g, with or without hypertension, should be treated with an ACE inhibitor or ARB. • ACE inhibitors are more effective than other antihypertensive agents in slowing the progression of most nondiabetic kidney diseases (Strong). The beneficial effect is greater in patients with higher levels of proteinuria (Strong).
Recommendations for clinical performance measures • GUIDELINE 8 • All patients with diabetic kidney disease should be treated with either an ACE inhibitor or an ARB (Guideline 8. 2), unless there is a documented contraindication in the medical record (such as pregnancy or a history of allergy; see Table 124). • GUIDELINE 9 • All patients with nondiabetic kidney disease and spot urine total protein-to-creatinine ratio ≥ 200 mg/g) should be treated with either an ACE inhibitor or an ARB (Guideline 9. 2), unless there is a documented contraindication in the medical record (such as pregnancy or a history of allergy; see Table 124).
Adherence to treatment guidelines – room for improvement Percent of patients The percentage of diabetic CKD patients receiving ACE-Is/ARBs has been slow to improve USRDS ADR, 2007
Enrollment characteristics of trials of ACE or ARB to slow progression of CKD ACE DM 1 ACE DM 2 ARB DM II ACE or ARB non-diabetic CKD All Number of studies 6 11 5 9 31 Number of patients 775 4, 941 4, 267 6, 451 16, 434 Explicit upper age exclusion, % 3 (49 -57) 5 (50 -80) 3 (70 -80) 7 (65 -70) 18 (58%) Maximum age of participants <70* 4 (67%) 3 (27%) 3 (60%) 7 (78%) 17 (55%) Comorbidity exclusion, % 3 (50%) 9(82%) 4 (80%) 8 (89%) 24 (77%) Weighted mean age, range 33. 7 (28. 9 -39) 63. 7 (4470. 2) 59. 4 (58. 6 -60) 63. 3 (45. 370. 2) 60. 8 2004 KDOQI guidelines on Hypertension and Anti-hypertensive agents in CKD; 2007 KDOQI guideline on Diabetes and Chronic Kidney Disease
Scatter plot of mean age by number of participants Mean weighted age 60. 8 yr
ALLHAT • ALLHAT differs in some important ways from other studies of antihypertensive agents in CKD. – First, the ACE inhibitor and dihydropyridine calcium-channel blocker were prescribed without a diuretic. By contrast, other studies in CKD have compared classes of antihypertensive agents usually prescribed in combination with a diuretic. – Second, the risk of kidney failure was lower than observed in other studies in CKD. – Third, proteinuria was not measured in ALLHAT, either in baseline or in follow-up. By contrast, most studies in CKD have included patients with proteinuria. – Thus, differences between ALLHAT and other studies in CKD may be due to the study design and the type of patient enrolled, rather than true differences in efficacy of combinations of antihypertensive agents used in CKD in slowing progression of kidney disease.
Risk for end-stage renal disease (ESRD) (A), combined outcome of doubling of serum creatinine or ESRD (B), or relative risk for these outcomes (Cand. D) in patients taking angiotensin-converting enzyme inhibitors (squares) and controls (circles), according to baseline urinary protein excretion Jafar, T. H. et. al. Ann Intern Med 2001; 135: 73 -87
• It is the opinion of the Work Group that the ALLHAT results do not rule out a beneficial effect of ACE inhibitors in nondiabetic kidney disease, particularly in patients with proteinuria. Instead, the Work Group concluded that ACE inhibitors should be used to delay the progression of most nondiabetic kidney diseases.
Prevalence of Chronic Kidney Disease (CKD) Stages by Age Group in NHANES 1988 -1994 and 1999 -2004 Coresh, J. et al. JAMA 2007; 298: 2038 -2047. Copyright restrictions may apply.
CKD “phenotype” in older patients • NHANES 99 -04: inclusive of patients 20 and older with a measured serum • creatinine and single spot urine albumin and creatinine measurement (n=13, 011) • CKD (n=1, 525): – e. GFR<60 – e. GFR>=60 with ACR>=200 mg/g
O’Hare et al, unpublished work
70. 2 yr 59. 7 yr 52. 4 yr O’Hare et al, unpublished work
Burden of co-morbidity O’Hare et al, unpublished work
162, 277 veterans with an e. GFR<60 or ACR>=200 mg/g
Summary patients • The vast majority of older individuals with CKD do not have proteinuria and do not have diabetes. • More than half of all non-proteinuric diabetic and non-diabetic CKD occurs in those 70 or older. • Older patients with CKD have a higher prevalence of co-existing cardiovascular disease compared with their younger counterparts.
Summary trials • Most trials of ACE/ARB conducted among populations with diabetes • Most have an upper age exclusion • Most have not enrolled participants older than 70 • ALLHAT included the largest number of participants (with and without diabetes) and had the highest mean age and was a negative trial • ALLHAT participants accounted for 58% of all participants in trials of non-diabetic CKD
Background considerations in evaluating benefits of ACE/ARB in elderly • We know very little about how the course of CKD varies with age. CKD progression may be slower in the elderly though this may reflect the higher prevalence of nonproteinuric CKD. • It is unclear that the same proxy outcomes are appropriate in elders (e. g. development of albuminuria in patients with diabetes). • Limited life expectancy. Competing risk of death is much higher in older compared with younger adults with CKD. • Higher prevalence of competing co-morbid conditions and polypharmacy in older patients with CKD may modify the benefits of ACE or ARB.
Rate of change in e. GFR Hemmelgarn et al, Kidney International Kidney Int. 2006 Jun; 69(12): 2155 -61.
Absolute risk of ESRD decreases with age among patients with similar level of e. GFR
Do the real and perceived risks of treatment differ by age? • Side effect profile of ace inhibitors in older patients is largely unstudied. • Burden of a given side-effect may differ by age (e. g. hyperkalemia may prompt hospital admission vs. outpatient treatment in a frail older patient). • Multiple comorbidities and polypharmacy so common in the elderly may complicate the burden and risks of any intervention.
What can primary care providers do?