Management of the neonate with arrhythmias Leila Rittey


")




")
")













- Slides: 26
Management of the neonate with arrhythmias Leila Rittey Paediatric Cardiology Registrar
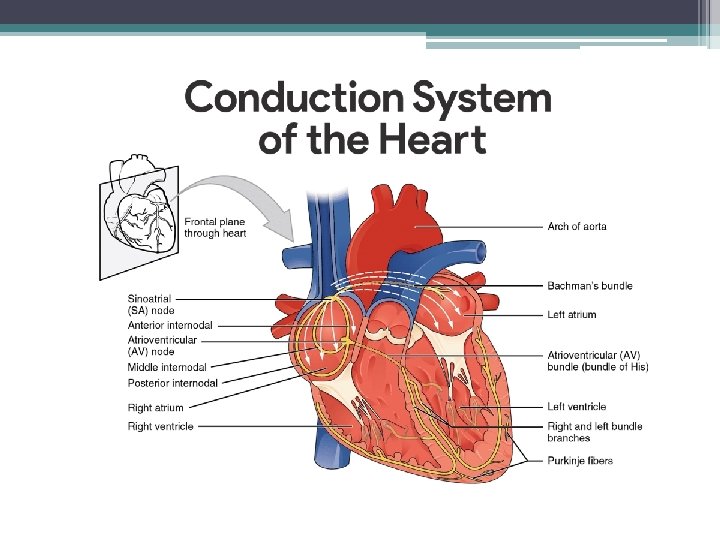
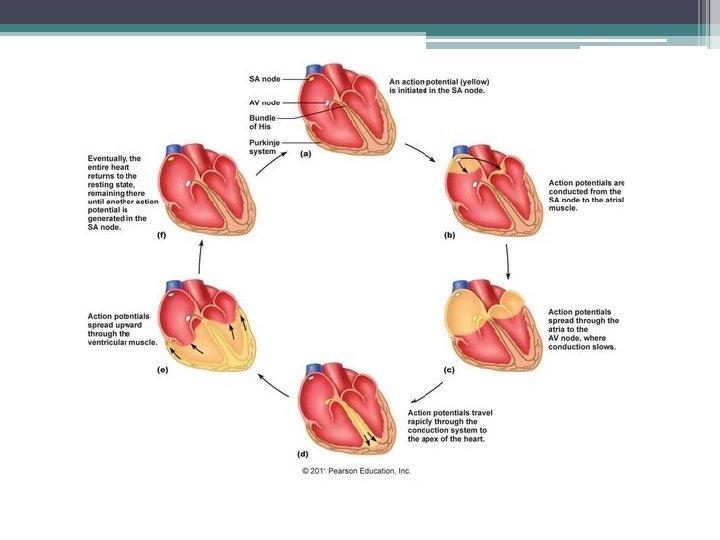
What common neonatal arrhythmias are there? • Atrial flutter • Supraventricular tachycardia • Congenital complete heart block
Atrial Flutter • Atrial signals very rapidly circulate around the tricuspid valve (atrial side) • Atrial rate around 300 bpm (can be much higher) • Often known about antenatally • Can look like any narrow complex tachycardia – adenosine can help with diagnosis
1: 1 2: 1
Flutter waves
Management of flutter • Sedate – use normal premeds for intubation – bag for 1 st shock, intubate if needs 2 nd • DC cardioversion – synchronised 1 -2 J/kg • Wake and extubate • No further management required unless recurrence – call cardiology if recurs after shock • Cardiac monitoring for 24 hours • Follow up in around 6/52 – for ECG and general review
Any questions on flutter? ?
Supraventricular tachycardia • Tachycardia starting above the ventricles • Narrow complex (unless aberrant conduction) • Generally safe – very prolonged (days/weeks) with fast rates can cause shock – can be very unwell even once cardioverted (echo – function) • Several different subtypes – all managed the same way acutely
Atrioventricular re-entry tachycardia (most common)
Management of SVT • Vagal manouvres – neonate – dunk in ice water at least 10 seconds, it will feel very long • Medical – adenosine – breaks cycle - antiarrythmics – propranolol/ atenolol, flecainide, amiodarone – stabilises myocardium • Electrical – if shocked – shock them (2 -4 J/kg)
Giving Adenosine • Give a proper dose - starting dose 200 micrograms/kg, if unsuccessful increase dose up to 300 then 500 micrograms/kg. • Adenosine needs a big flush – see next slide • Adenosine needs to be given quickly via a 3 way tap (broken down by red blood cells) • Always record a rhythm strip when giving adenosine – it gives us a lot of information • Very rarely can cause VF – always give in a room with a defib available
How big is a big flush? • • Less than 1 kg – 5 ml 1 -2 kg – 7 ml 2 -3 kg – 10 ml >3 kg – 15 ml • There is no point giving a small flush - the adenosine won’t get where it needs to in time!!
SVT – shocked child • Crash team • If has IV access can quickly try adenosine whilst setting up defibrillator • DC cardioversion – synchronised 2 J/kg, if unsuccessful 4 J/kg • Can give adenosine IO – 500 -700 mcg/kg • Intubation – in itself this can sometimes help revert to sinus rhythm • May require amiodarone – only after discussions with paediatric cardiology
Follow up • • Can stop cardiac monitoring 48 hrs after last SVT If well controlled – minimal episodes – 4 -6/52 If difficult to control – 2/52 24 hr tape prior to follow up very useful
Any questions on SVT? ?
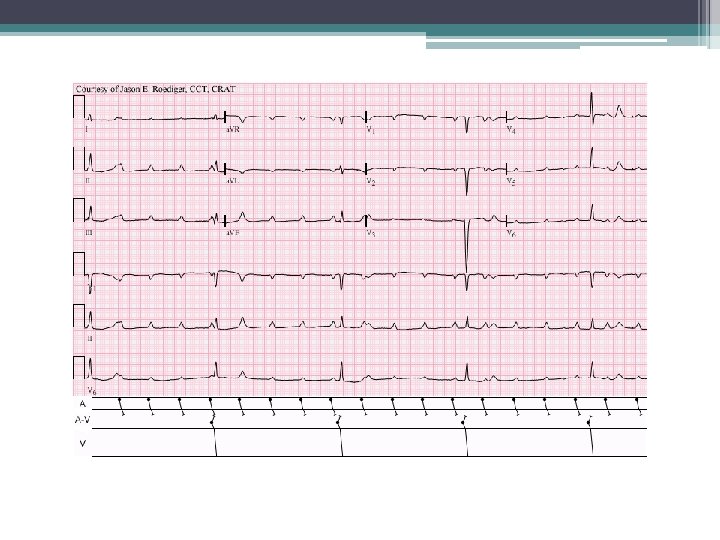
Congenital complete heart block • • The atria and ventricles do not communicate Ventricular escape rhythm determines heart rate Atria generally pumping much faster Can be associated with maternal Anti-Ro and Anti-La antibodies
Assessment • ECG - ? pauses, wide QRS complexes, long QTc • Echo – rarely associated cardiomyopathy/aortic root dilatation • Essentially – is the ventricular rate fast enough to maintain an adequate cardiac output? ? • Generally aim to keep the heart rate above 55 (or 70 if associated CHD)
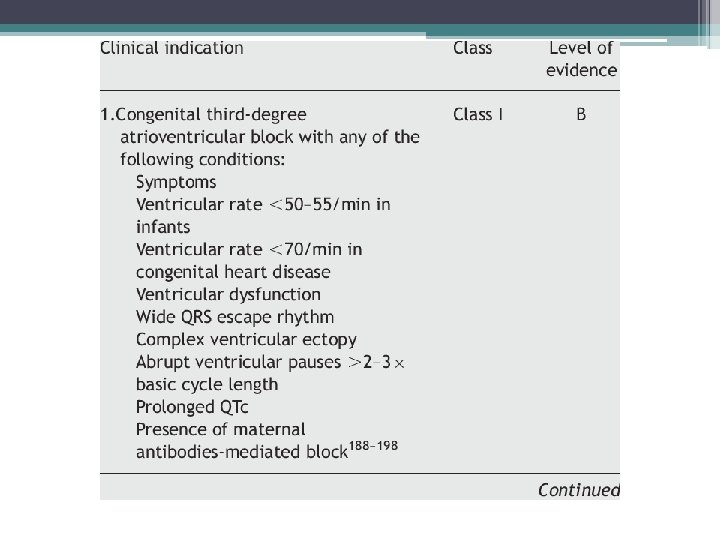
Management • Nothing – if the heart rate is sufficient follow up is all that’s required • Isoprenaline – medically speeds up the heart rate - 0. 02 microgram/kg/minute increase as necessary to a maximum infusion rate of 0. 2 microgram/kg/minute • Temporary pacing – if too small for permanent system/very sick in an emergency (defib) • Permanent pacing – from around 2 kg
Any questions on CCHB?
Summary • Atrial flutter – generally resolves completely after DC cardioversion with no ongoing management needed • SVT – beware the baby who has been in SVT for a long time (antenataly included) - Give adenosine properly • CHB – if HR over 55 -60 (70 if CHD) generally ok • Bonus point – atrial ectopics very common in neonates and nothing to worry about