Management of Symptomatic Bradycardia and Tachycardia Introduction Cardiac

Management of Symptomatic Bradycardia and Tachycardia

Introduction Cardiac arrhythmias are a common cause of sudden death. l ECG monitoring should be established ¡ Collapse suddenly ¡ Have symptoms of coronary ischemia or infarction. l ECG monitoring ¡ Conventional or automated external defibrillator (AED) ¡ “Quick-look" paddles feature on conventional defibrillators l For patients with acute coronary ischemia, the greatest risk for serious arrhythmias occurs during the first 4 hours after the onset of symptoms. l

學習目標 Bradycardia: evaluation and treatment, algorithm 2. Tachycardia : evaluation and treatment, algorithm 1.

Principles of Arrhythmia Recognition and Management Should not base treatment decisions solely on rhythm interpretation and neglect clinical evaluation. l Evaluate the patient’s symptoms and clinical signs l ¡ ¡ ¡ Ventilation Oxygenation Heart rate Blood pressure Level of consciousness Look for signs of inadequate organ perfusion

Principles of Arrhythmia Recognition and Management Bradycardia l Unstable S/S ¡ ¡ ¡ acute altered mental status ongoing severe ischemic chest pain congestive heart failure hypotension other signs of shock Persist despite adequate airway and breathing prepare to provide pacing. l For symptomatic high-degree (second-degree or third-degree) AV block provide transcutaneous pacing ( TCP ) without delay. l

Principles of Arrhythmia Recognition and Management Tachycardia l Unstable with severe signs and symptoms related to tachycardia prepare for immediate cardioversion. l Stable narrow-complex or widecomplex tachycardia l Know when to call for expert consultation regarding complicated rhythm interpretation, drugs, or management decisions.

Bradycardia

Bradycardia l Defined as a heart rate of <60 beats per minute. l A slow heart rate may be physiologically normal for some patients. l While initiating treatment, evaluate the clinical status of the patient and identify potential reversible causes.

Bradycardia Algorithm Circulation 2005; 112: IV-67 -77 IVCopyright © 2005 American Heart Association

Bradycardia Algorithm Circulation 2005; 112: IV-67 -77 IVCopyright © 2005 American Heart Association

Bradycardia n l l l l Identify signs and symptoms of poor perfusion and determine if those signs are likely to be caused by the bradycardia hypotension acute altered mental status chest pain congestive heart failure seizures syncope other signs of shock related to the bradycardia

Bradycardia l AV blocks are classified as first, second, and third degree. l Causes of AV blocks : ¡ medications ¡ electrolyte disturbances ¡ structural problems resulting from acute myocardial infarction and myocarditis.
 l")
First-degree AV block l defined by a prolonged PR interval (>0. 20 second) l usually benign

Second-degree AV block l Mobitz ¡ block type I block is at the AV node ¡ often transient and may be asymptomatic

Second-degree AV block l Mobitz ¡ block type II block is most often below the AV node at the bundle of His or at the bundle branches ¡ often symptomatic, with the potential to progress to complete (third-degree) AV block

Third-degree heart block May occur at the AV node, bundle of His, or bundle branches l No impulses pass between the atria and ventricles l Can be permanent or transient, depending on the underlying cause l

Therapy Be prepared to initiate transcutaneous pacing quickly in patients who do not respond to atropine. l Pacing is also recommended for severely symptomatic patients, especially when the block is at or below the His-Purkinje level (ie, type II second-degree or third-degree AV block). l
 l Improved heart")
Therapy Atropine l First-line drug for acute symptomatic bradycardia (Class IIa) l Improved heart rate and signs and symptoms associated with bradycardia l Useful for treating symptomatic sinus bradycardia and may be beneficial for any type of AV block at the nodal level.

Therapy Atropine l The recommended dose for bradycardia is 0. 5 mg IV every 3 to 5 minutes to a maximum total dose of 3 mg. l Doses <0. 5 mg may paradoxically result in further slowing of the heart rate. l Atropine administration should not delay implementation of external pacing for patients with poor perfusion.

Therapy Atropine l Use cautiously in the presence of acute coronary ischemia or myocardial infarction; increased heart rate may worsen ischemia or increase the zone of infarction. l Atropine may be used with caution and appropriate monitoring following cardiac transplantation. It will likely be ineffective because the transplanted heart lacks vagal innervation.
 l Class I intervention for symptomatic bradycardias l")
Therapy Pacing (Transcutaneous pacing, TCP ) l Class I intervention for symptomatic bradycardias l Indication : started immediately for patients ¡ Unstable, particularly those with high-degree block ¡ If there is no response to atropine ¡ If atropine is unlikely to be effective ¡ If the patient is severely symptomatic
 Can be painful and may fail to produce")
Therapy Pacing (Transcutaneous pacing, TCP ) Can be painful and may fail to produce effective mechanical capture l Use analgesia and sedation for pain control l Verify mechanical capture and re-assess the patient’s condition l If TCP is ineffective (eg, inconsistent capture) l ¡ ¡ prepare for transvenous pacing consider obtaining expert consultation

Therapy Alternative Drugs to Consider l Second-line agents for treatment of symptomatic bradycardia l They may be considered when the bradycardia is unresponsive to atropine and as temporizing measures while awaiting the availability of a pacemaker.

Epinephrine l Used for patients with symptomatic bradycardia or hypotension after atropine or pacing fails (Class IIb). l Begin the infusion at 2 to 10 µg/min and titrate to patient response. l Assess intravascular volume and support as needed.

Dopamine l Both α- and ß-adrenergic actions l Dopamine infusion (at rates of 2 to 10 µg/kg per minute) can be added to epinephrine or administered alone. l Titrate the dose to patient response. l Assess intravascular volume and support as needed.

Glucagon l Improvement in heart rate, symptoms, and signs associated with bradycardia l IV glucagon (3 mg initially, followed by infusion at 3 mg/h if necessary) l Given to in-hospital patients with druginduced (eg, ß-blocker or calcium channel blocker overdose) symptomatic bradycardia not responding to atropine.

Tachycardia

Tachycardia 三部曲 The first step l Determine if the patient’s condition is stable or unstable The second step l Obtain a 12 -lead ECG to evaluate the QRS duration (ie, narrow or wide). The third step l Determine if the rhythm is regular or irregular

Tachycardia 三部曲 l If the patient becomes unstable at any time, proceed with synchronized cardioversion. l If the patient develops pulseless arrest or is unstable with polymorphic VT, treat as VF and deliver high-energy unsynchronized shocks (ie, defibrillation doses).
 tachycardias ( QRS <0. 12 second ) in order of frequency")
Tachycardia Narrow–QRS-complex (SVT) tachycardias ( QRS <0. 12 second ) in order of frequency — Sinus tachycardia — Atrial fibrillation — Atrial flutter — AV nodal reentry — Accessory pathway–mediated tachycardia — Atrial tachycardia (ectopic and reentrant) — Multifocal atrial tachycardia (MAT) — Junctional tachycardia

Tachycardia Supraventricular tachycardias l From the atria or sinoatrial node ¡ ¡ l Sinus tachycardia Atrial fibrillation Atrial flutter Atrial tachycardia From the atrioventricular node ¡ ¡ Atrioventricular re-entrant tachycardia Atrioventricular nodal re-entrant tachycardia
 — Ventricular tachycardia (VT)")
Tachycardia Wide–QRS-complex tachycardias ( QRS > 0. 12 second ) — Ventricular tachycardia (VT) — SVT with aberrancy — Pre-excited tachycardias (advanced recognition rhythms using an accessory pathway) l Most wide-complex (broad-complex) tachycardias are ventricular in origin

Tachycardia Irregular narrow-complex tachycardias — Atrial fibrillation — Atrial flutter — MAT

Tachycardia Initial Evaluation and Treatment of Tachyarrhythmias l The evaluation and management of tachyarrhythmias is depicted in the ACLS Tachycardia Algorithm. l Note that the "screened" boxes indicate therapies that are intended for inhospital use or with expert consultation available.

ACLS Tachycardia Algorithm Copyright © 2005 American Heart Association Circulation 2005; 112: IV-67 -77 IV-
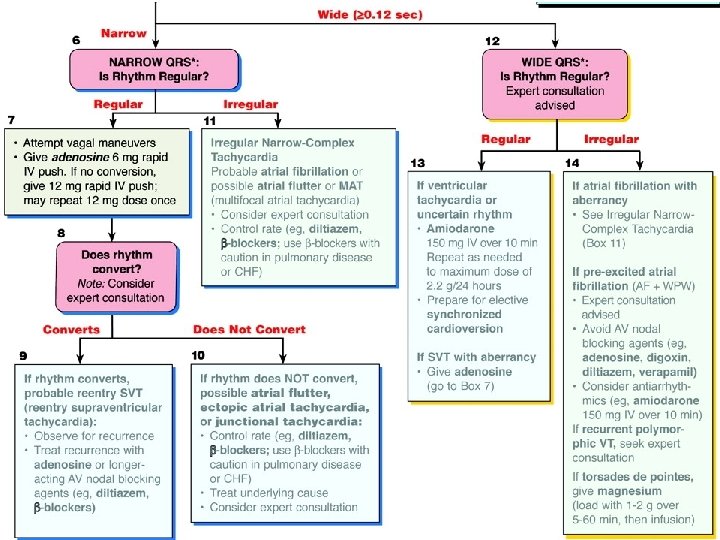

ACLS Tachycardia Algorithm

Synchronized Cardioversion and Unsynchronized Shocks l Low-energy shocks should always be delivered as synchronized shocks because delivery of low energy unsynchronized shocks is likely to induce VF. l If cardioversion is needed and it is impossible to synchronize a shock (eg, the patient’s rhythm is irregular), use highenergy unsynchronized shocks (defibrillation doses).
 unstable SVT")
Synchronized Cardioversion and Unsynchronized Shocks Synchronized cardioversion is recommended to treat (1) unstable SVT due to reentry (2) unstable atrial fibrillation (3) unstable atrial flutter (4) unstable monomorphic (regular) VT

Synchronized Cardioversion and Unsynchronized Shocks l If possible, establish IV access before cardioversion and administer sedation if the patient is conscious. l Consider expert consultation.

Cardioversion The recommended initial dose Atrial fibrillation l 100 J - 200 J with a monophasic waveform l 100 J - 120 J with a biphasic waveform l Escalate the second and subsequent shock doses as needed.

Cardioversion The recommended initial dose Atrial flutter and other SVTs l 50 J - 100 J monophasic damped sine (MDS) waveform is often sufficient. l If the initial 50 -J shock fails, increase the dose in a stepwise fashion. l More data is needed before detailed comparative dosing recommendations for cardioversion with biphasic waveforms can be made.

Cardioversion The recommended initial dose Ventricular tachycardia l Determined by the morphologic characteristics and the rate of the VT l Monomorphic VT : unstable but has a pulse treat with synchronized cardioversion ¡ ¡ l initial shock of 100 J with a monophasic waveform insufficient data to recommend specific biphasic energy doses for treatment of VT If there is no response to the first shock, increase the dose in a stepwise fashion (eg, 100 J 200 J 360 J).

Cardioversion Polymorphic VT : unstable l Treat the rhythm as VF l Deliver high-energy unsynchronized shocks (ie, defibrillation doses) l If there is any doubt whether monomorphic or polymorphic VT is present in the unstable patient, do not delay shock delivery to perform detailed rhythm analysis—provide high-energy unsynchronized shocks (ie, defibrillation doses).

Cardioversion is not likely to be effective for treatment of l Junctional tachycardia l Ectopic or multifocal atrial tachycardia ¡ these rhythms have an automatic focus, arising from cells that are spontaneously depolarizing at a rapid rate ¡ shock delivery to a heart with a rapid automatic focus may increase the rate of the tachyarrhythmia

Regular Narrow. Complex Tachycardia

Sinus tachycardia

Sinus Tachycardia l Common and usually results from a physiologic stimulus, such as fever, anemia, or shock l Occurs when the sinus node discharge rate is >100 times per minute in response to a variety of stimuli or sympathomimetic agents. l No specific drug treatment is required. l Therapy is directed toward identification and treatment of the underlying cause.

Sinus Tachycardia l When cardiac function is poor, cardiac output can be dependent on a rapid heart rate. l In such compensatory tachycardias, stroke volume is limited, so "normalizing" the heart rate can be detrimental.
 Evaluation l Paroxysmal supraventricular tachycardia (PSVT) : often abrupt onset")
Supraventricular Tachycardia (Reentry SVT) Evaluation l Paroxysmal supraventricular tachycardia (PSVT) : often abrupt onset and termination l The rate of reentry SVT exceeds the typical upper limits of sinus tachycardia at rest (>120 beats per minute) with or without discernible P waves.
 Therapy l Vagal maneuvers l Adenosine l Calcium Channel Blockers")
Supraventricular Tachycardia (Reentry SVT) Therapy l Vagal maneuvers l Adenosine l Calcium Channel Blockers l ß-Blockers

Vagal maneuvers l Vagal maneuvers and adenosine are the preferred initial therapeutic choices for the termination of stable reentry SVT. l Vagal maneuvers alone (Valsalva maneuver or carotid sinus massage) will terminate about 20% to 25% of reentry SVT l In younger patients, vagal maneuvers were often unsuccessful.
 l Give rapidly")
Adenosine l 6 mg as a rapid IV push (Class I) l Give rapidly over 1 to 3 seconds through a large (eg, antecubital) vein 20 -m. L saline flush and elevation of the arm l If the rate does not convert within 1 to 2 minutes, give a 12 -mg bolus. l Give a second 12 -mg bolus l More rapid with fewer severe side effects than verapamil.

Adenosine l Safe and effective in pregnancy l Have several important drug interactions l Increased dose : significant blood level of theophylline, caffeine l Reduced dose to 3 mg : ¡ in patients taking dipyridamole or carbamazepine ¡ those with transplanted hearts ¡ if given by central venous access

Adenosine l Side effects : common but transient ¡ flushing ¡ dyspnea ¡ chest pain l Monitor the patient for recurrence and treat any recurrence with adenosine or control the rate with a longer-acting AV nodal blocking agent (eg, diltiazem or ßblocker).

Calcium Channel Blockers l Rate control with a nondihydropyridine calcium channel blocker (ie, verapamil or diltiazem) or ß-blocker as a second-line agent (Class IIa) l Act primarily on nodal tissue ¡ slow the ventricular response to atrial arrhythmias by blocking conduction through the AV node ( 阻斷傳導 ) ¡ terminate the reentry SVT that depends on conduction through the AV node ( 終止再迴旋)
 and, to a lesser extent, diltiazem (")
Calcium Channel Blockers Verapamil ( isoptin ) and, to a lesser extent, diltiazem ( Herbesser )may decrease myocardial contractility and critically reduce cardiac output in patients with severe left ventricular dysfunction. l Harmful when given to patients with atrial fibrillation or atrial flutter associated with known pre-excitation (Wolff-Parkinson-White [WPW]) syndrome. l ß-Blockers should be used with caution in patients with pulmonary disease or congestive heart failure. l

Calcium Channel Blockers Verapamil l l 2. 5 to 5 mg IV bolus over 2 minutes (over 3 minutes in older patients) Repeated doses of 5 -10 mg may be administered every 15 -30 minutes to a total dose of 20 mg. An alternative dosing regimen is to give a 5 -mg bolus every 15 minutes to a total dose of 30 mg. Should be given only to patients with narrowcomplex reentry SVT or arrhythmias known with certainty to be of supraventricular origin. Should not be given to patients with impaired ventricular function or heart failure.
 IV over 2")
Calcium Channel Blockers Diltiazem l 15 -20 mg (0. 25 mg/kg) IV over 2 minutes l if needed, in 15 minutes give an IV dose of 20 -25 mg (0. 35 mg/kg). l The maintenance infusion dose is 5 -15 mg/h, titrated to heart rate.

ß-Adrenergic Blockers l. A wide variety of ß-blockers may be given for treatment of supraventricular tachyarrhythmias. l Atenolol, metoprolol, labetalol, propranolol, esmolol l the effects of circulating catecholamines and heart rate and blood pressure l They also have various cardioprotective effects for patients with acute coronary syndromes.

ß-Adrenergic Blockers For acute tachyarrhythmias, these agents are indicated for rate control in the following situations : l For narrow-complex tachycardias that originate from either a reentry mechanism (reentry SVT) or an automatic focus (junctional, ectopic, or multifocal tachycardia) uncontrolled by vagal maneuvers and adenosine in the patient with preserved ventricular function (Class IIa) l To control rate in atrial fibrillation and atrial flutter in the patient with preserved ventricular function
 l 5 mg slow IV (over 5 minutes). l")
ß-Adrenergic Blockers Atenolol (ß 1) l 5 mg slow IV (over 5 minutes). l If the arrhythmia persists 10 minutes after that dose and the first dose was well tolerated, give a second dose of 5 mg slow IV (over 5 minutes). Metoprolol (ß 1) l Given in doses of 5 mg by slow IV/IO push at 5 -minute intervals to a total of 15 mg.
 l 0. 1 mg/kg by")
ß-Adrenergic Blockers Propranolol (ß 1 and ß 2 effects) l 0. 1 mg/kg by slow IV push divided into 3 equal doses at 2 - to 3 -minute intervals. l The rate of administration should not exceed 1 mg/min. l May repeat total dose in 2 minutes if necessary.
 ß 1 selective ß-blocker that")
ß-Adrenergic Blockers Esmolol Short-acting (half-life 2 to 9 minutes) ß 1 selective ß-blocker that is l Administered in an IV loading dose of 500 µg/kg (0. 5 mg/kg) over 1 minute, followed by a 4 minute infusion of 50 µg/kg per minute (0. 05 mg/kg per minute) for a total of 200 µg/kg. l If the response is inadequate, a second bolus of 0. 5 mg/kg is infused over 1 minute, with an increase of the maintenance infusion to 100 µg/kg (0. 1 mg/kg) per minute (maximum infusion rate: 300 µg/kg [0. 3 mg/kg] per minute). l

ß-Adrenergic Blockers Side effects : bradycardias, AV conduction delays, and hypotension l Cardiovascular decompensation and cardiogenic shock : infrequent complications l Contraindications : second-degree or thirddegree heart block, hypotension, severe congestive heart failure, and lung disease associated with bronchospasm l These agents may be harmful for patients with atrial fibrillation or atrial flutter associated with known pre-excitation (WPW) syndrome. l
 Complex Tachycardia")
Wide- (Broad-) Complex Tachycardia
 Complex Tachycardia The most common forms of wide-complex tachycardia are 1. VT")
Wide- (Broad-) Complex Tachycardia The most common forms of wide-complex tachycardia are 1. VT 2. SVT with aberrancy 3. Pre-excited tachycardias (associated with or mediated by an accessory pathway) l An unstable patient with wide-complex tachycardia is presumed to have VT, and immediate cardioversion is performed

Ventricular Tachycardia

Non-sustained ventricular tachycardia and accelerated idioventricular rhythm
 Complex Tachycardia VENTRICULAR Regular l Monomorphic VT Irregular l Polymorphic VT l")
Wide- (Broad-) Complex Tachycardia VENTRICULAR Regular l Monomorphic VT Irregular l Polymorphic VT l Torsades de pointes tachycardia
 Complex Tachycardia SUPRAVENTRICULAR Regular l SVT with aberrancy Irregular l Atrial fibrillation")
Wide- (Broad-) Complex Tachycardia SUPRAVENTRICULAR Regular l SVT with aberrancy Irregular l Atrial fibrillation with aberrancy l Pre-excited atrial fibrillation (ie, atrial fibrillation with WPW syndrome)
 l Unstable: synchronized cardioversion")
Therapy for Regular Wide-Complex Tachycardias VT ( ventricular tachycardia ) l Unstable: synchronized cardioversion l Stable : IV antiarrhythmic drugs may be effective l Amiodarone (Class IIa) ¡ Give 150 mg IV over 10 minutes ¡ Repeat as needed to a maximum dose of 2. 2 g IV per 24 hours l Alternative sotalol. drugs : procainamide and

Irregular Tachycardias

Rhythm strip in atrial fibrillation
")
Rhythm strip in atrial flutter (rate 150 beats/min)

Atrial Fibrillation and Flutter Evaluation l An irregular narrow-complex or wide-complex tachycardia is most likely atrial fibrillation with an uncontrolled ventricular response. Other diagnostic possibilities include MAT. l We recommend a 12 -lead ECG and expert consultation if the patient is stable.

Atrial Fibrillation and Flutter Therapy l Management should focus on ¡ Control of the rapid ventricular rate (rate control) ¡ Conversion of hemodynamically unstable atrial fibrillation to sinus rhythm (rhythm control)

Atrial Fibrillation and Flutter l Initial rate control with ¡Diltiazem ¡ß-blockers ¡Magnesium

Atrial Fibrillation and Flutter l Rhythm control in patients with atrial fibrillation of < 48 hours duration ¡ Amiodarone ¡ Ibutilide ¡ Propafenone ¡ Flecainide ¡ Digoxin ¡ Clonidine ¡ Magnesium

Atrial Fibrillation and Flutter Patients with atrial fibrillation for >48 hours are at increased risk for cardioembolic events and must first undergo anticoagulation before rhythm control. l Electric or pharmacologic cardioversion (conversion to normal sinus rhythm) should not be attempted in these patients unless the patient is unstable or the absence of a left atrial thrombus is documented by transesophageal echocardiography (TEE). l

WPW Syndrome l Expert consultation is advised. l Do not administer AV nodal blocking agents such as adenosine, calcium channel blockers, digoxin, ß-blockers. (can cause a paradoxical increase in the ventricular response to the rapid atrial impulses of atrial fibrillation )
 VT l Requires immediate treatment because it is likely to deteriorate to")
Polymorphic (Irregular) VT l Requires immediate treatment because it is likely to deteriorate to pulseless arrest. l Pharmacologic treatment of recurrent polymorphic VT is determined by the presence or absence of a long QT during sinus rhythm.
 VT l Unstable provide high-energy (ie, defibrillation dose) unsynchronized shocks. l The")
Polymorphic (Irregular) VT l Unstable provide high-energy (ie, defibrillation dose) unsynchronized shocks. l The many QRS configurations and irregular rates present in polymorphic VT make it difficult or impossible to reliably synchronize to a QRS complex. l A good rule of thumb is that if your eye cannot synchronize to each QRS complex, neither can the defibrillator/cardioverter.
 VT If there is any doubt whether monomorphic or polymorphic VT is")
Polymorphic (Irregular) VT If there is any doubt whether monomorphic or polymorphic VT is present in the unstable patient, do not delay shock delivery for detailed rhythm analysis—provide high-energy unsynchronized shocks (ie, defibrillation doses). l Use the biphasic device-specific dose ¡ Truncated exponential waveform 150 -200 J ¡ Rectilinear waveform 120 J l If a monophasic defibrillator is used, use a dose of 360 J for all unsynchronized shocks l

Torsades de pointes l Polymorphic VT with long QT interval l The first step is to stop medications known to prolong the QT interval. l Correct electrolyte imbalance and other acute precipitants l Magnesium l Isoproterenol l Ventricular pacing

Torsades de pointes

Magnesium l l l Recommended for the treatment of torsades de pointes VT with or without cardiac arrest, but it has not been shown to be helpful for treatment of non-torsades pulseless arrest. Effective for rate control in patients with atrial fibrillation with a rapid ventricular response Give magnesium sulfate in a dose of 1 to 2 g diluted in D 5 W over 5 to 60 minutes. Slower rates are preferable in the stable patient. A more rapid infusion may be used for the unstable patient.

Summary The goal of therapy for bradycardia or tachycardia is to rapidly identify and treat patients who are hemodynamically unstable. l Pacing or drugs, or both, may be used to control symptomatic bradycardia. l Cardioversion or drugs, or both, may be used to control symptomatic tachycardia. l ACLS providers should closely monitor stable patients pending expert consultation and should be prepared to aggressively treat those who develop decompensation. l
- Slides: 94