MANAGEMENT OF SECOND STAGE OF LABOUR SPONTANEOUS VERTEX

MANAGEMENT OF SECOND STAGE OF LABOUR: SPONTANEOUS VERTEX DELIVERY ELIZABETH CHODZAZA MELANIE HAMI BARBARA MLEWAH MAY, 2011

GOAL • To equip learners with knowledge, skills and attitudes in managing women during second stage of labour.

LEARNING OUTCOMES By the end of this session, learners should be able to: • Define second stage of labour • Demonstrate competencies in conducting the delivery of the baby • Demonstrate positive attitude in the management of a woman in second stage of labour

SECOND STAGE OF LABOUR • The second stage of labour begins from full dilation of the cervix to the delivery of the baby. • It lasts up to 30 minutes for multipara and up to one hour for primigravida

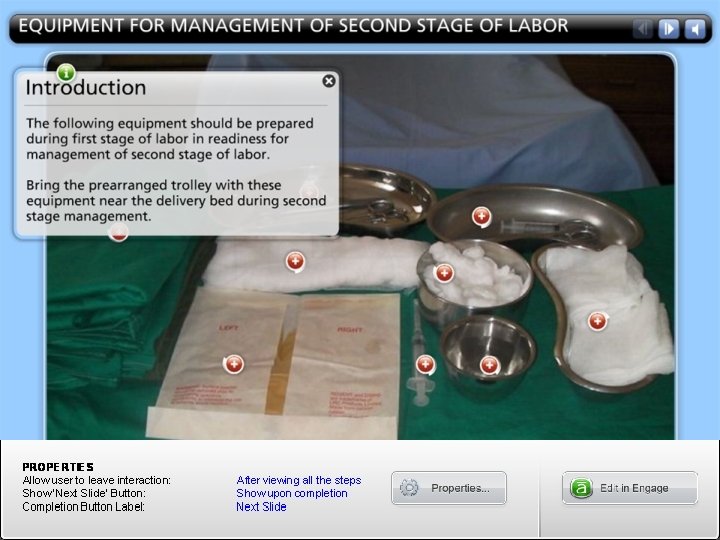
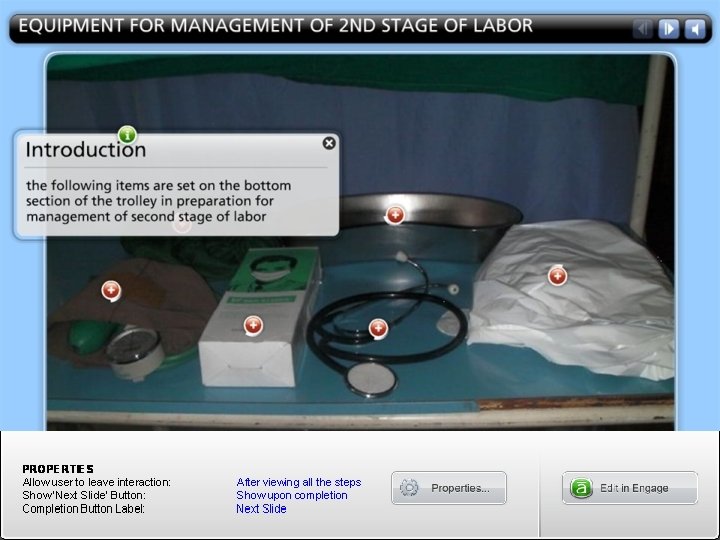
Delivery of the Baby 1. Preparation for Delivery • Delivery trolley should be ready and sterile equipment should be used • Check the following: foetal heart rate; contraction and descent of the head • Ensure bladder is empty

Preparation for Delivery cont’ • Put on clean apron, scrubs and on sterile gloves • Swabs the thighs and vulva with antiseptic solution • Do vaginal examination • Mother should be reminded on what to do during the delivery

Preparation for Delivery cont’ • Place the anal pad exposing the perineum • Do not leave the patient alone • Review positions of delivery (e. g. squatting, semi sitting, lithotomy, lateral hands and knees)

Actual Delivery • The midwife stands on the right side of the bed (if right handed) facing towards the woman if in supine position. • The woman should be encouraged to assume a position for pushing that is comfortable and aids in the descend of the foetus. • Note time and the women should push in response to her natural bearing down reflex

Actual Delivery cont’ • The midwife maintains flexion of the fetal head by applying gentle pressure on the presenting part in the direction of the perineum until biparietal diameter of 9. 5 cm sub occipital bregmatic diameter of 9. 5 cm are free of the vulva.

• Help her rest between contractions • Offer encouraging feedback after each push and praise her effort • The midwife maintains flexion of the fetal head by applying gentle pressure on the presenting part in the direction of the perineum until biparietal diameter of 9. 5 cm sub occipital bregmatic diameter of 9. 5 cm are free of the vulva

Actual Delivery cont’ • When crowning has occurred instruct the mother to pant • Allow spontaneous birth of the head • Discard the perineal pad • Quickly check the cord around the neck, if present, check if tight or loose. If tight place clamp and cut the cord to free the baby from strangulation

Actual Delivery cont’ • Clean secretions from eyes, mouth and nostrils, to ensure clear airway and prevent infection • Wait for the restitution and external rotation of the head which is accompanied by internal rotation of the shoulders, so that the smallest diameter is presented thereby preventing tears to birth canal
")
Actual Delivery cont’ • Place hands on each side of the baby’s head (biparietal) • Ask the woman to bear down • Direct the head downward towards the anus to deliver the upper or anterior shoulder then lift it gently to deliver the posterior shoulder.

Actual Delivery cont’ • Move the top most hand from the head to support the rest of the baby’s body as it slides out. • Place the baby on the mother’s abdomen • Note time and sex • Quickly wipe the baby while assessing for breathing and if there will be need for further resuscitation

MANAGEMENT OF SECOND STAGE OF LABOR


During delivery observe the following • Foetal heart rate in between contractions • Advancement of presenting part • Condition of the mother • Perineum for tear and make episiotomy if necessary
- Slides: 20