MANAGEMENT OF POST PARTUM HAEMORRHAGE DRILL Contributors Dr

MANAGEMENT OF POST PARTUM HAEMORRHAGE DRILL

Contributors Dr. Jyoti Bhaskar Dr. Jyoti Agarwal Dr. Sharda Patra Dr. Sharda Jain
 MMR – 109")
MDG 5 MMR IN 2010 -2012 – 178 ( from 212) MMR – 109 by 2015

MATERNAL MORTALITY Our Best Estimate is A Gross Underestimate 200, 000 women die from PPH each year** 35 -56%

How much time do we have ? It is estimated that, if untreated, Death occurs on average in: 2 hours from Postpartum Hemorrhage 12 hours from Antepartum Hemorrhage 2 days from Obstructed Labor 6 days from Infection

WHY DRILLS IN OBSTETRICS ? PPH • Death from PPH is avoidable • Are Mostly Unexpected – Immediate and Adequate action needed

High Risk Situations Medico- Legal Consequences

Guidelines of RCOG Green top No. 52 May 2009 ü COMMUNICATE. ü RESUSCITATE. ü MONITOR / INVESTIGATE. ü STOP THE BLEEDING.

CALL FOR HELP

CALL

RESUSCITATE A AIRWAY BREATHNG CIRCULATION
 for: • Crossmatch (4 units")
14 GUAZE – 2 IN NUMBER Venepuncture (20 ml) for: • Crossmatch (4 units minimum) • Full blood count • Coagulation screen including fibrinogen • Renal and liver function for baseline. START RINGER LACTATE TILL BLOOD COMES

Transfuse blood as soon as possible • • • Infuse 2 litres of warmed Crystalloid Hartmann’s solution Colloid (1– 2 litres) as rapidly as required. RAPID WARMED infusion of fluids.

If crossmatched blood is still unavailable Uncrossmatched Group Specific Blood OR ‘O Rh. D Negative” Blood

MONITORING • Keep position Flat • Keep the woman warm using appropriate available measures. • Temperature every 15 mts • Continuous pulse, blood pressure recording and respiratory rate • Foley catheter to monitor urine output. Documentation of fluid balance, blood products and procedures.

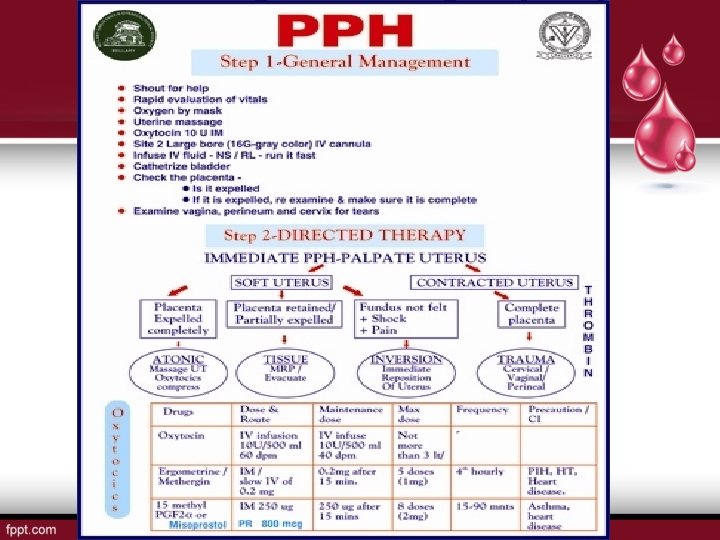
STOP THE BLEEDING Tone Tissue Trauma Thrombin

Bimanual Compression If uterus is relaxed : massaging the uterus will expel any retained bits & stimulate uterine contractions

UTEROTONICS -- OXYTOCIN 10 IU IM. Or • 20– 40 IU in 1 L of normal saline at 60 drops per minute. • Continue oxytocin infusion (20 IU in 1 L of IV fluid at 40 drops per minute) until hemorrhage stops FIGO Safe Motherhood and Newborn Health (SMNH) Committee / International Journal of Gynecology and Obstetrics 117 (2012) 108– 118

OXYTOCIN – FIRST LINE Storage • preferred storage is refrigeration • it may be stored at temperatures up to 30 °C for up to 3 months without significant loss of potency

ERGOMETRINE Dose: 0. 2 mg im or slow iv Repeat 0. 2 mg after I/M can be repeated every 2 -4 hrs Maximum 5 doses (1 mg) in 24 hr Storage: 2– 8 °C and protect from light and from freezing • Hypertension is a relative contraindication • Contraindicated with concomitant use of certain drugs used to treat HIV
. 1")
OR • Syntometrine (combination of oxytocin 5 units and ergometrine 0. 5 mg). 1 ampoule IM (warning, IV could cause hypotension).
. Single")
OR • Misoprostol (if oxytocin is not available or administration is not feasible). Single dose of 800 μg sublingually (4× 200 -μg tablets). Storage: aluminum blister pack, room temperature, in a closed container.

OR CARBOPROST Dose: 0. 25 mg im. Can be repeated every 15 min. Maximum upto 2 mg or 8 doses.

AORTIC COMPRESSION • It is simple life saving procedure • Aortic compression may be used to stop bleeding at any stage. • Ideally, the birth attendant should accompany the woman during transfer FIGO GUIDELINES 2012 Prevention and treatment of postpartum hemorrhage in low-resource settings☆ FIGO Safe Motherhood and Newborn Health (SMNH) Committee

AORTIC COMPRESSION

Non-Inflatable Anti-Shock Garment

If conservative measures fail to control haemorrhage Initiate Surgical Haemostasis SOONER RATHER THAN LATER

Internal Uterine Tamponade

CONDOM BALLON TAMPONADE

B-Lynch “Brace” Suture

Stepwise Uterine Devascularization • Uterine arteries • Tubal branch of ovarian artery • Internal iliac artery

Embolisation

Resort to hysterectomy SOONER RATHER THAN LATER (especially in cases of placenta accreta or uterine rupture)

Documentation and Debriefing Important to record: • Sequence of events • Time and sequence of administration of pharmacological agents, fluids, blood products • The time of surgical intervention • The condition of mother throughout.

REMEMBER • GOLDEN HOUR OF RESUSCITATION • RULE OF 30 • HAEMOSTASIS ALGORYTHM
 &")
HAEMOSTASIS algorithm • H- ask for help • A- assess (vitals, blood loss) & resuscitate • E 1. Establish etiology(tone, tissue, trauma, thrombine) 2. Ecbolics (syntometrine, ergometrine) 3. Ensure availability of blood • M - massage the uterus • O – oxytocin infusion & prostaglandin

§ SShift to operating theatre Bimanual compression Pneumatic anti-shock garment • T- Tissue & trauma to be excluded • A- apply compression sutures • S- systematic pelvic devascularisation • I - interventional radiology • S- subtotal/total hysterectomy

INNOVATIVE TECHNIQUES FOR LOW RESOURCE SETTINGS • EASY AND ACCURATE BLOOD LOSS MEASUREMENT

OXYTOCIN IN UNIJECT • Single • Prefilled • Nonreusable • Easy to use. • Compact size

Non-Inflatable Anti-Shock Garment

TOOL KIT FOR PPH

It is an Enigma • • It is sudden often unpredicted assessed subjectively Can be catastrophic. The clinical picture changes so rapidly that unless timely action is taken maternal death occurs within a short period.

To Conclude, Management of PPH Has Evolved From: • Panic • Hysterectomy l Pitocin l Prostaglandins l Happiness

Reminds Us -- Every mother has to be Saved
- Slides: 45