Management of patients with Acromegaly H Delshad M







































 : - Long-acting Release : 10 , 20")









 All patients in the study")









- Slides: 64
Management of patients with Acromegaly H. Delshad M. D Endocrinologist Research Institute for Endocrine Sciences Shahid Beheshti University of Medical Sciences
Somatropin or Growth Hormone ● GH is synthesized in somatotrope cells which make up about 50% of ant. Pituitary cells. ●The pulsatile secretion of GH is regulated by two hypothalamic regulatory hormones, GHRH and somatostatin. + - GH GHRH Somatostatin
GH Target Tissues GH stimulates the hepatic production of IGF-1 that actually stimulates growth.
ACROMEGALY • Persistent hyper-secretion of GH • Prevalence : 60 – 120 individuals / million • Condition is underrecognized and many patients may never receive medical attention. • The average interval from the onset of symptoms until diagnosis is about 12 years.
Acromegaly: Causes • Pituitary somatotroph adenoma : The most common , 75% macroadenoma • GH-producing tumors are frequently mixed tumor • Pituitary somatotroph carcinoma • Hypothalamic GHRH releasing tumors • Non-endocrine GHRH secreting tumors • Non-endocrine GH secreting tumors • Excess growth factor activity (Acromegaloidism)
Gigantism 7
ACROMEGALY
Signs and symptoms at presentation of 324 patients diagnosed with Acromegaly from 1995 to 2006 Acral enlargement Facial features Hyperhydrosis Snoring Headache fatigue Gonadal dysfunction Macroglossia Teeth spacing Visual defects Paresthesia Acne/ Hirsutism Deepning of voice 0 100 20 40 60 80
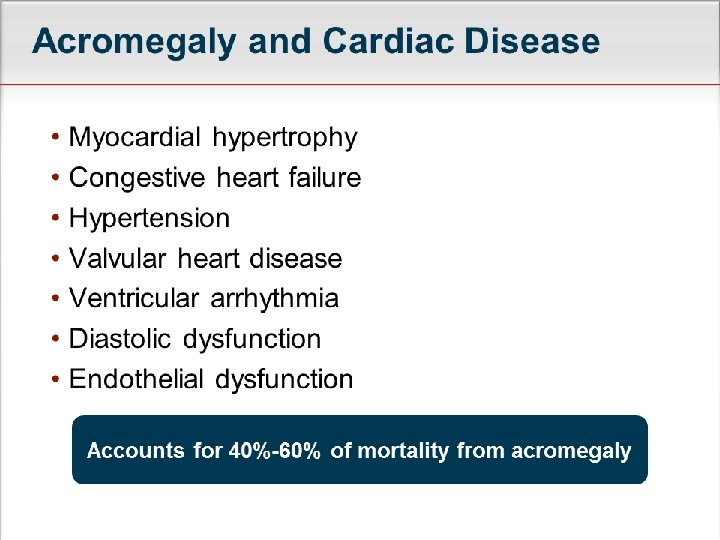
Acromegaly Comorbidities
Acromegaly Significantly Impact Survival
Investigation of patients with suspected ACROMEGALY ► Does the patient have ACROMEGA LY? ►If the answer is “yes” then what is the
Documenting Excess GH Secretion Basal GH IGF - 1 Oral GTT
GH secretion is pulsatile and diurnal During most of the day : 0. 5 – 1 ng/ml Before meal or after exercise : 2 – 5 ng/ml After vigorous exercise : 20 – 30 ng/ml GH is high : - Uncontrolled DM - Liver disease - Malnutrition.
GH Secretion
The best single test Do not vary from hour to hour Reflect integrated GH secretion during the preceding day or longer Age dependent
Pitfal in IGF-1 Level Low IGF-1 High IGF-1 ● Fasting, Anorexia , Malnutrition ● Pregnancy ● Poorly controlled DM ● Adolescence ● Puberty ● Liver disease ● Thyrotoxicosis ● Exogenous Estrogen
Oral GTT The most specific dynamic test for establishing the diagnosis Gold standard test for determining controls of GH secretion after surgery. 2 h GH after 75 gr. Glucose : * RIA < 1 ng/ml * IRMA or ICMA < 0. 3 ng/ml
DIAGNOSIS OF ACROMEGALY Initial screening : IGF-1 If IGF-1 is elevated, test GH : -Random or Fasting -Nadir GH following OGGT When IGF-1 and random GH are elevated in the setting of suggestive clinical findings, an OGTT is likely not necessary.
Baseline Evaluation Of Acromegaly • Pituitary function testing • Prolactin level • Pituitary MRI • Visual fields
21 Skull X-Ray
Pituitary Imaging Microadenoma Giant invasive macroadenoma Macroadenoma
Pituitary MRI
Pituitary Imaging Pituitary Apoplexy A 3× 2× 2 cm pituitary Macroadenoma with bleeding in the centre
Visual Filed
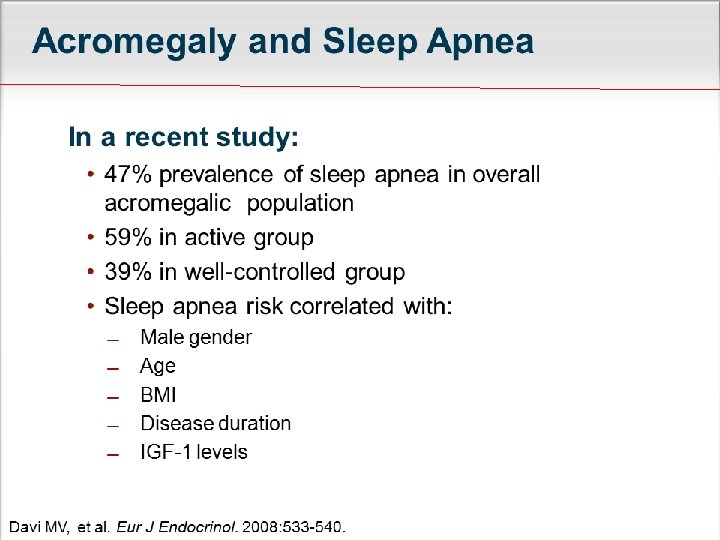
Screening For Comorbidities Colonoscopy Sleep tests for sleep apnea FBS & Hb. A 1 C Echocardiography
Predictors of Mortality GH > 2. 5 micg/L Elevated IGF-1 Hypertension Age Time of delay from diagnosis Male gender Prior pituitary radiotherapy ACTH dependent adrenal insufficiency Treatment with hydrocortisone > 25 mg/day
Acromegaly Treatment
In treating Acromegaly what matters most ? Tumor shrinkage? GH concentration? IGF-1 Concentration? Symptom control?
Probability of Survival According to Serum GH Concentration
Long –term Mortality Improves with Normal IGF-1 Level after Surgery
ACROMEGALY: Treatment Options
SURGERY Transsphenoidal resection: - Initial treatment in most cases % of Patients With Normalized IGF-1 - 80% microadenomas - < 50% macroadenomas Immediate effect Potentially curative
Risk of Surgery New hormone insufficiency 5– 10% of cases , may improve with decompression of gland CSF leak /meningitis : 1 – 2% Visual deterioration : < 1% Mortality nationwide : < 1% Risk of recurrence : 5 – 10 % at 5 years
SURGERY: Contraindicated Patient refusal Sever cardiomyopathy Sever respiratory disease
Is pretreatment beneficial? May reduce anesthetic risk Some studies have shown improved surgical remission with medical pretreatment: - Retrospective data show mixed result - Tow recent studies show a benefit but the studies have limitations It is not contraindicated but, there is currently insufficient evidence
Options for Medical Therapy Somatostatin Analogues • Octreotide • Lanreotide Dopamin Agonist • Bromocriptine • Cabergoline GH Receptor Antagonist • Pegvisomant
Options for Medical Therapy Somatostatin Analogues • SSA Receptor Ligands • Directly inhibit GH secretion • Indirectly inhibit IGF-1 secretion Dopamin Agonist • D 2 Receptor • Directly inhibit GH secretion GH Receptor Antagonist • Does not suppress GH secretion • Indirectly inhibit IGF-1 secretion • Directly inhibit IGF-1 secretion
Primary Medical Therapy For Acromegaly Should be considered if the surgery is contraindicated or refused. May be appropriate for : - Inaccessible, invasive tumor - Tumors unlikely to be surgically curable - Tumors not compressing optic chiasm
SOMATOSTATIN ANALOGUES OCTREOTIDE ( Sandostatin LAR) : - Long-acting Release : 10 , 20 , 30 mg/month - Subcutaneous : 100 – 500 micg / TDS LANTREOTIDE (Somatuline Depot) - Depot : 60 , 90 , 120 mg / month - Slow release : 30 mg every 7 to 14 days They appear to be equivalent for control of biochemical markers and symptoms
SSA THERAPY : EFFICACY Controls GH and IGF-1 excess in about 50 -65% Maximal benefit may be achieved after 10 years therapy When used as secondary therapy , tumor shrinkage occurs in about 30% of patients Tumor shrinkage in most patients is between 20 to 50 % Freda PU. JCEM 2002; 87: 3013 - 3018
Surgical debulking enhances efficacy of SSA therapy Colao, et al. JCEM 2006; 91: 85 -92 Petrossians p, et al. Eur J Endocrinol, 2005: 152: 61 -66 Karavitaki N, et al. Clin Endocrinol(Oxf), 2008: 68: 970 - 975
SSA THERAPY : SIDE EFFECTS GI : Diarrhea , Nausea , Abdominal pain - Early : 49% - Persistent : < 10% Biliary tract abnormalities - All types : 50% - New gallstones : 15% ( 4 – 22%) Abnormalities of Glucose metabolism - Hypoglycemia : 2% - Hyperglycemia : 7 – 15 % Freda PU. JCEM 2002; 87: 3013 - 18
When to consider other strategies? SSA is poorly tolerated due to side effects SSA is not effective in normalizing levels of GH and IGF-1 Tumor grows on SSA
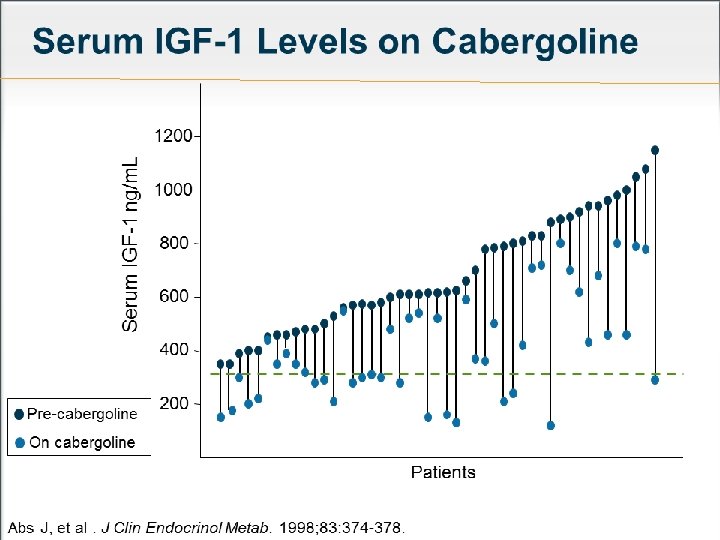
Dopamine Agonists Cabergoline : has a modest effect in some patients. It is recommended to use in combination with SSA Primary therapy for patients with a small adenoma and mild elevation of IGF-1. Cabergoline : 0. 5 mg/week , if necessary 1 mg twice a week. Side effects : Nausea, Light headedness, Depression , Constipation, Nasal stuffiness
GH Receptor Antagonist Pegvisomant : a mutated GH molecule to which polymers have been attached at several sites to prolong its half-life. Daily self-administered SC injection (10 -30 mg) Must follow IGF-1 levels (every 4 to 6 weeks) because GH levels will not be interpretable.
Results in 90 patients with acromegaly who were treated with Pegvisomant for 12 to 24 months. The open circles represent the pretreatment values and the closed circles the lowest post-treatment values. The shaded areas represent the normal ranges for age. van der Lely, et al. Lancet 2001; 358: 1754.
PIGVISOMANT : Adverse Effects Injection site reaction Elevated liver enzyme Increase of pituitary tumor growth Headache
PIGVISOMANT : Effect on tumor size N= 61 on Pigvisomant 3 patients had tumors that increased significantly ( > 25% increase in size) 45 patients had MRI at 24 months with no significant change Buhk J, et al. J Clin Endocrinol Meta. 2010; 95: 552 -558
Pigvisomant Plus SSA Therapy (It is an expensive combination) All patients in the study achieved control of their IGF-1 levels, which were previously uncontrolled on maximal doses of an SSA, when Pegvisomant was added. Neggers SJ, et al. JCEM , 2007; 92: 4598 -4601
Control Criteria by Treatment Type Post Surgical : Normal IGF-1 and OGGT GH nadir < 0. 4 mig/L Somatostatine Analogue : Normal IGF-1 and random GH < 1. 0 mig/L Pegvisomant: Normal IGF-1
Interpreting Discordant Results In patients with discordant IGF-1 and GH : - IGF-1 elevation more predictive of persistent symptoms and increased insulin resistance. In patients on SSA therapy - Decrease in IGF-1 is a better predictor decrease in tumor size than a decrease in GH In the setting of discordant result, normalization of IGF-1 may correlate with improved Acromegaly control.
Radiation Therapy Tow goals Post-operatively Further tumor growth cessation Biochemical normalization IGF-1 and GH
Radiation Result
Late Effects of Pituitary Radiation
SSAs and Radiation
ACROMEGALY Effects of Successful Treatment • Glucose and lipid metabolism improve. • Cardiovascular disease improves. • Respiratory disease improves but sleep apnea does not always revers. • Joint thickness and joint pain may improve , but bone deformities are permanent Harvey Cushing, s first Acromegalic patient operated in 1909 shows the typical changes of Acromegaly.
Updated outcomes criteria ; 2010 Outcome Criteria • Random GH< 1 Controlled disease micg/L • GH after OGTT < 0. 4 micg/L • Age – Sex normalized IGF-1 • Random GH> 1 micg/L Active Disease • Nadir GH after OGTT > 0. 4 micg/L • Elevated IGF-1 • Clinically Active Giustina A, et al. JCEM 2010; 95(7) : 3141 -3148
Monitoring The Patient Measurement of GH and IGF-1 GH response to OGTT: 3 -6 months after surgery OGTT is not helpful in patient on SSA MRI : 3 -6 months after therapy Pituitary function : - 3 months after surgery -periodically after radiotherapy