Management of Neurogenic Bladder Dr Rajesh Taneja M

Management of Neurogenic Bladder Dr. Rajesh Taneja M. B. B. S. , M. Ch. (Urology), FGSI Senior Consultant Urologist New Delhi

The Urinary Bladder STORAGE – Suppression of tone of Detrusor – Contraction of smooth muscle sphincter, Trigone – Contraction of Voluntary Sk muscle sphincter EVACUATION Excitation and Contraction of Detrusor Cholinergic parasympathetic outflow S 2, 3, 4. Relaxation of Bladder neck and Trigone Inhibition of Sympathetic activity SENSORY INNERVATION Sympathetic T 11 -L 1 Somatic S 234
")
CENTRAL NERVOUS CONTROL OF MICTURICTION Prefrontal Corfex Limbic area Basal Ganglia Pons (Micturition centre) Dorsal Tegmental Nucleus in Cervical Cord Sacral Spinal Centre of Micturition (S 3) Dementia CVA Parkinsonism M. S. D. M.

Normal Urinary Bladder Reservior 500 ml Sensation of Distension Ability to accommodate Ability to initiate and sustain a contraction till Bladder is empty Voluntary initiation or inhibition of voiding
 International")
Classification of Neuropathic Bladder Failure to store Failure to void (Wain et al) International Continence Society Detrusor Smooth muscle sphincter Skeletal muscles sphincter Normal Hyper Hypo

Injury above the sacral micturition Centre Reduced capacity Involuntary Detrusor Contraction High Intra vesical pressure Marked Hyper trophy of bladder Spasticity of pelvic striated muscle Failure to Store

Spastic Urinary bladder Clinical Presentation Frequent involuntary urination Small capacity < 300 ml Scanty amounts Associated with spasms of lower extremities Lack of bladder sensation Upper tract dilation – Reflux / Obstruction Voiding may be triggered by stimulation of skin of perineum or genitalia Urinary Infection

Injury at or below the Sacral micturition Centre Large capacity urinary bladder Low Pressure No Voluntary contraction Failure to Evacuate Decreased tone of external spincter Evacuation may be accomplished by straining lower abdomen

Flaccid Bladder Overflow incontinence Reduced Sphincter tone No Sensation LMN Signs in lower limbs Kidneys are usually safe

Evaluation of Neuropathic Bladder History Bladder Sensation Frequency and volume of urination Frequency and volume of involuntary loss of urine Extent of voluntary control if any Fever, Flank pain, Hematuria Symptoms suggestive of renal failure Examination

Investigations Urine RE and Culture S Creatrine USG Full bladder capacity Residual urine Detrusor Hypertrophy Bladder neck status Hydronephrosis
 Bladder Capacity Bladder pressure Sensation Un inhibited Detrusor Contraction")
Urodynamic Evaluation Uroflometry Cystometrogram (CMG) Bladder Capacity Bladder pressure Sensation Un inhibited Detrusor Contraction EMG – Dyssynergia UPP Status of smooth muscle sphincter

Management of Neurogenic Bladder Understanding the individual problem Failure to store Failure to void Both Associated Problems Infection Obstruction and Dilatation of kidneys Stone Formation Renal Failure

GOALS OF MANAGEMENT • Preservation of upper tracts • To keep the patient dry-(minimise incontinence) • Evacuation at will • Prevention of infection
 Intermittent catheterisation Reducing Bladder")
Flaccid Bladder Parasympathomimetic drugs-Urotone Voiding by clock (To minimise leakage) Intermittent catheterisation Reducing Bladder outflow obstruction TUR BN/Prostate
 Roliten (Tolterodine ) Probanthin Continuous drainage Per")
SPASTIC BLADDER Pharmacotherapy Anticholinergic mediction Tropan (oxybutynine) Roliten (Tolterodine ) Probanthin Continuous drainage Per uretheral catheter Suprapubic catheter Condom Drainage Intravesieal pressure < 40 cm water No dilatation of upper tracts

SPASTIC BLADDER Sphinctertomy and condom drainage To save upper tract from deterioration Role of artificial Sphincters Rhizotomy (Sacral 3 -4) To reduce intravesical pressure Surgical Percutaneous Chemical Neuro prosthetics

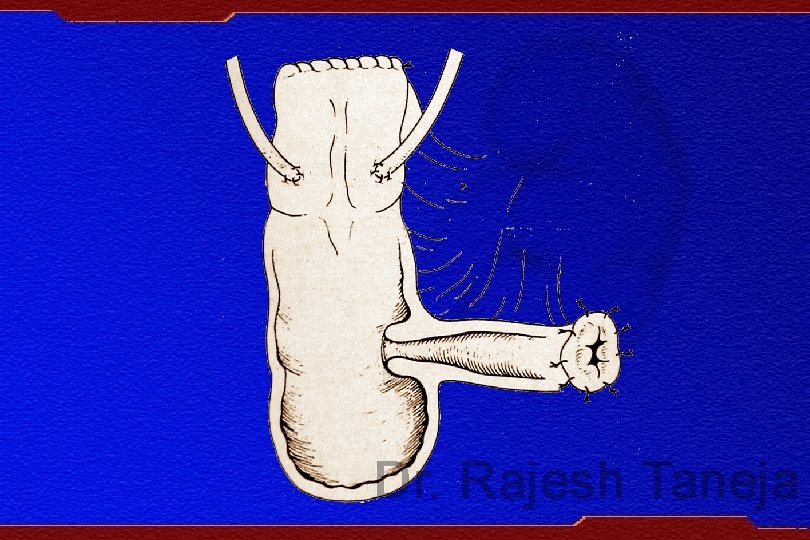
Augmentation of Bladder Use of Intestinal segment to augment Bladder Reduces Pressure Increases capacity of reservoir Reduces frequency of intermittent catherterisation Ureters may be reimplanted if refluxing or obstructed
 Free external")
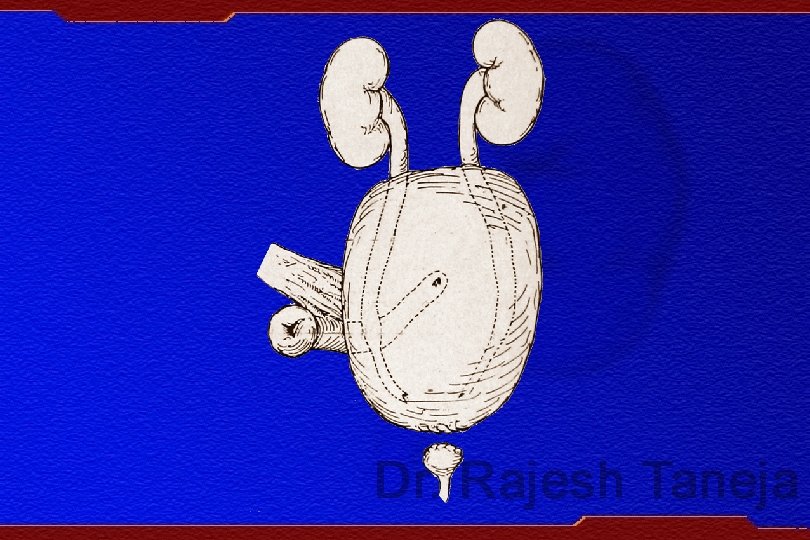
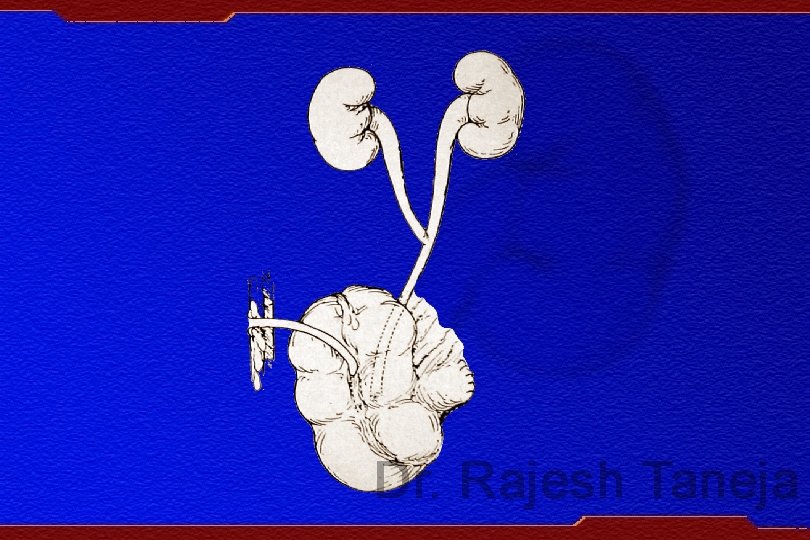
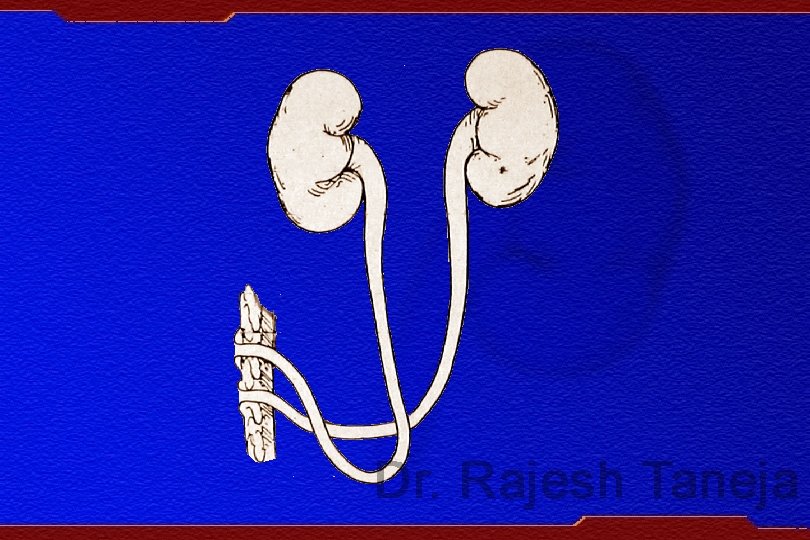
Diversion of Urine Continent Abdominal Stoma with reservoir (Serum creatnine <2 mg%) Free external diversion in Renal failure Cutaneous ureterostomy Ileal conduit

FUTURE TRENDS STEM CELL THERAPY

CONCLUSION Prime aim of management of Neuropathic bladder is preservation of renal function Attempt should be made to delineate the exact nature of vesical dysfunction Milder form of neurogenic bladder can be managed pharmacologically Timely appropriate surgical intervention can prevent deterioration of upper urinary tracts and preserve renal function
- Slides: 25