Management of Difficult Airway in Anesthesia Part I






 Cormack Grade of Laryngoscopic View")
 Mallampati class Class 1 Cormack Grade Gr. 1 Gr.")
 Geriatric patients with depressed cheeks Patients with")



 Severe diabetes mellitus can result in abnormal cross-linkage of")
 32% of 115 diabetic patients who underwent renal and/or")
:")

 All-or-none gambling how could you take the")
 The only universal rule and the No.")
 Held in mid-October every year There")


 No matter where you practice, something you")
 Anticipated Difficult Airway Difficult Mask Ventilation YES")



 in Chinese Patients Anesthesia & Analgesia")
 Duration (min) Recovery Index (min) SCC 1 mg/kg 55.")








")


 Attach syringe at the end")
 Connect to a traditional ventilator Commercial")






. use O 2")



 Anticipated Difficult Airway Difficult Mask Ventilation YES")

 Puncture site should be close to")




- Slides: 73
Management of Difficult Airway in Anesthesia Part I Chan Wei-Hung MD Department of Anesthesiology National Taiwan University Hospital
Difficult Airway in Anesthesia Practice Inability to maintain airways explains more than 30% of death in anesthesia. More than 85% in respiratory-related malpractice would lead to severe brain damage or death.
Difficult Airway Anticipated Unanticipated How to evaluate the difficult airway? v Evaluation for Difficult Intubation v Evaluation for Difficult Mask Ventilation
Evaluation for Difficult Intubation Mallampati test Thyromental distance Mouth opening C-spine mobility Dentition Difficult recognition of cricothyroid membrane
Mallampati Test Class III Class IV
How to Do Mallampati Test Patient remains seated. Ask the patient to open the mouth as widely as possible and protrude tongue as far out as possible. Phonation should not be encouraged. Perform the test twice to avoid bias.
Validity of the Test (I) Cormack Grade of Laryngoscopic View
Validity of the Test (II) Mallampati class Class 1 Cormack Grade Gr. 1 Gr. 2 Gr. 3 Gr. 4 59. 5% 14. 3% 0 0 5. 7% 6. 7% 4. 7% 1. 9% 0 0. 5% 4. 3% 2. 4% (73. 8%) Class 2 (19%) Class 3 (7. 14%) Total 210 patients
Difficult Mask Ventilation Facial deformity (congenital, acquired) Geriatric patients with depressed cheeks Patients with a nasogastric tube Extremely fat patients Patients with head fixation devices Patients with long mustache High risk of aspiration Patients with orofacial burn Patients with extremely limited mouth opening —Difficulty in inserting an oropharyngeal airway
Pathological Conditions Associated with Difficult Airway Infection Trauma C-spine injury Obesity DM Acromegaly Foreign body Ankylosing spondylitis Rheumatoid arthritis Tumors Congenital syndromes Pregnancy
The ENT Cases Always check the chart for visibility of vocal cord. In case of airway tumors/abscess, search for CT/MRI images for the position and the width of the airway.
Rheumatoid Arthritis TMJ ankylosis, limitation of motion of the cervical spine, deviation of the larynx, cricoarytenoid arthritis Laryngeal involvement--edematous, hyperemic cords, arytenoid mucosa with swollen aryepiglottic folds and false cords A smaller ET tube may be necessary.
DM & Difficult Airway (I) Severe diabetes mellitus can result in abnormal cross-linkage of collagen by non-enzymatic glycosylation in connective tissues due to chronic hyperglycemia. These tissues then become stiff and may result in limited joint mobility (stiff joint syndrome). “Prayer sign”
DM & Difficult Airway (II) 32% of 115 diabetic patients who underwent renal and/or pancreatic transplant had a difficult laryngoscopy Anesth Analg 1988; 67: 1162 -5 Difficult laryngoscopy in 31% of 62 diabetic patients undergoing renal transplantation or Anaesthesia 1990; 45: 1024 -7 vitrectomy. Of 725 transplant patients, diabetic vs nondiabetic = 4. 8 vs 1. 0% were identified as having difficult laryngoscopies, but no extraordinary devices were required for intubation. Anesthesia & Analgesia. 86: 516 -9, 1998
Palm Print as a Predictor of Difficult Airway in DM Acta Anaesthesiologica Scandinavica. 42(2): 199 -203, 1998
Sensitivity Specificity Falsenegative Falsepositive Palm print grade>0 1. 00 0. 57 0 26 Mallampati >1 0. 41 0. 80 13 12 Mallampati >2 0. 50 0. 98 21 1 TMD <6 cm 0. 14 0. 9 19 6 Head extension<35° 0. 50 0. 70 11 18 BMI > 27 0. 23 0. 97 17 2 DM > 10 yrs 0. 91 0. 67 2 20 DM type 0. 45 0. 51 12 30 Acta Anaesthesiologica Scandinavica. 42(2): 199 -203, 1998
Decision Making in Anticipated Difficult Airway (I) All-or-none gambling how could you take the risk? The anesthesiologists always walk on a tightrope between becoming a hero or being bankrupted. An outcome-based question Personal experience and preference is supremely important and govern the outcome.
Decision Making in Anticipated Difficult Airway (II) The only universal rule and the No. 1 guideline Do not ever try to use anything that you are not familiar with or any fancy equipment in such a situation! So be well-prepared for such a hard time!
Annual Meeting of ASA (American Society of Anesthesiologists) Held in mid-October every year There always be a workshop for airway management, which is deserved to attend during residency. The 2002 Annual Meeting will be in Orlando, Florida on October 12 -16, 2002. http: //www. asahq. org/
Decision Making in Anticipated Difficult Airway (III) No matter where you practice, something you must know before you make decision: What kind of equipment do you have at hand? What is the quality of the equipment? Do you have any assistant? (mask ventilation) How much does your assistant know? Do you have immediate access to the help from your fellow anesthesiologists? What is the attitude of the surgeons?
Decision Making in Anticipated Difficult Airway (IV) Anticipated Difficult Airway Difficult Mask Ventilation YES Awake Intubation NO Induction Procedures
Succinylcholine: Friend or Foe? Rapid onset, short duration – always welcomed. Undeniable weak points: Fatal hyperkalemia (burn, spinal cord injury) Malignant hyperthermia Masseter spasm Atypical plasma cholinesterase
SCC vs Vecuronium In 44 pediatric patients, the mouth opening by mm: Succinylcholine Vecuronium Before After 16. 9± 2. 8 12. 6± 4. 3 19. 8± 3. 6 20. 9± 4. 1 Mouth opening was measured by a constant force (1. 4 N). Anesthesiology 69(1): 11 -6, 1988
Mivacurium or Rocuronium: Destined to Be Ousted? Low dose slow onset High dose long duration For Mivacurium For Rocuronium 0. 2~0. 25 mg/kg IV bolus Onset 2 min Duration 5~15 min 1~1. 2 mg/kg IV bolus Onset 45 sec Duration 30 min
The Prolonged Duration of Rocuronium (0. 6 mg/kg) in Chinese Patients Anesthesia & Analgesia 91(6): 1526 -30, 2000
Mivacurium + Rocuronium Onset (sec) Duration (min) Recovery Index (min) SCC 1 mg/kg 55. 1 4. 2 1. 3 Mi 0. 2 mg/kg 116 10. 4 4. 2 Ro 0. 6 mg/kg 97. 9 23. 7 9. 2 Ro 0. 9 mg/kg 70. 5 36. 4 10. 1 Mi 0. 1 mg/kg + Ro 0. 3 mg/kg 67 15. 2 7. 3 Mi 0. 15 mg/kg + Ro 0. 45 m/kg 55 25. 3 9. 9 British Journal of Anaesthesia 79(4): 450 -5, 1997
Preoxygenation: How Much Is Enough? Two techniques common in use: 1. Tidal volume breathing (TVB) of oxygen for 3– 5 min 2. Deep breaths (DB) 4 times within 0. 5 min Both are equally effective in increasing arterial oxygen tension (Pao 2). Anesth Analg 1981; 60: 313– 5
Anesth Analg 2001; 92: 1337 -1341
After preoxygenation to an end-tidal oxygen concentration greater than 90%, each subject received 5 mg/kg thiopental and 1 mg/kg succinylcholine. Anesthesiology 2001, 95: 754 -759 Succinylcholine itself cannot save your account. (Esp. when you did not do good
Who is at the risk of premature desaturation? Obesity Parturient Neonate Decreased FRC
Other Weak Points of Pentothal + SCC Copious secretion after awaking the patient, hampering subsequent fiberoscope. It is said that with this technique a period of inadequate ventilation would happen during recovery. “Pentothal + SCC then take a look” is generally a good idea, but it does not guarantee anything!
All the Toys You Know How to Play No 1 rule: Do not stick to the same one too long. No 2 rule: Always be doing something.
Equipment Ready to Use Direct laryngoscope Think more about the laryngoscopy: Patient position Smaller ET tube size Different blades Make good use of the stylet External laryngeal pressure If you can visualize epiglottis and make sure the midline position, you can give it a try; otherwise give it up immediately.
External Laryngeal Pressure
Other Techniques Light wand Laryngeal mask airway Combitube Wu’s scope Cuffed oropharyngeal airway (COPA) Awake the patient
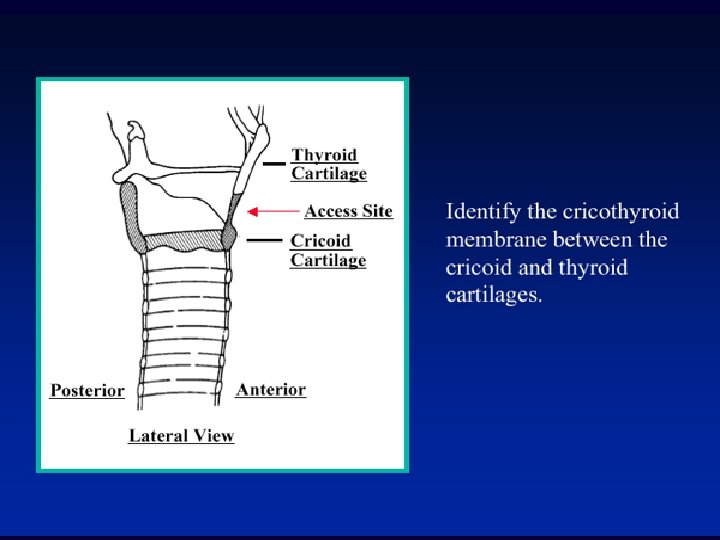
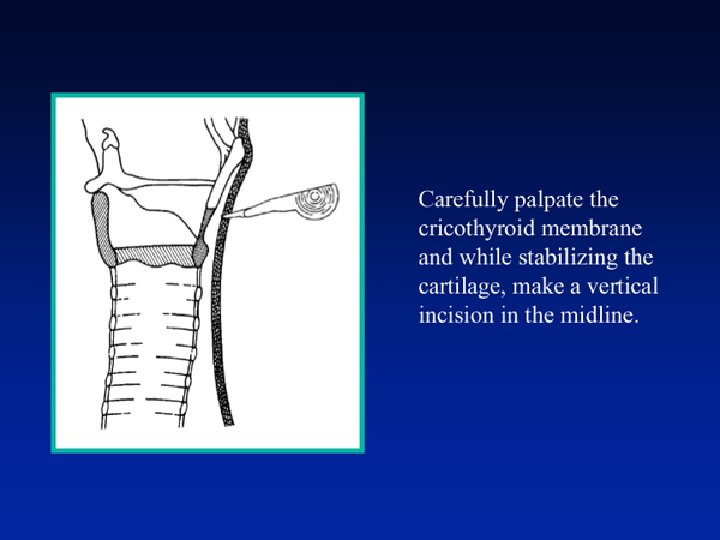
Endpoint of All Techniques Can’t intubate, can’t ventilate…… Establish airway through cricothyroid membrane immediately Easier said than done. Not every cricithyroid membrane is easily recognized. (Especially on your first time, perhaps the last time, too) Try to define it on a fat man with a short neck. Remember to hyperextend the neck.
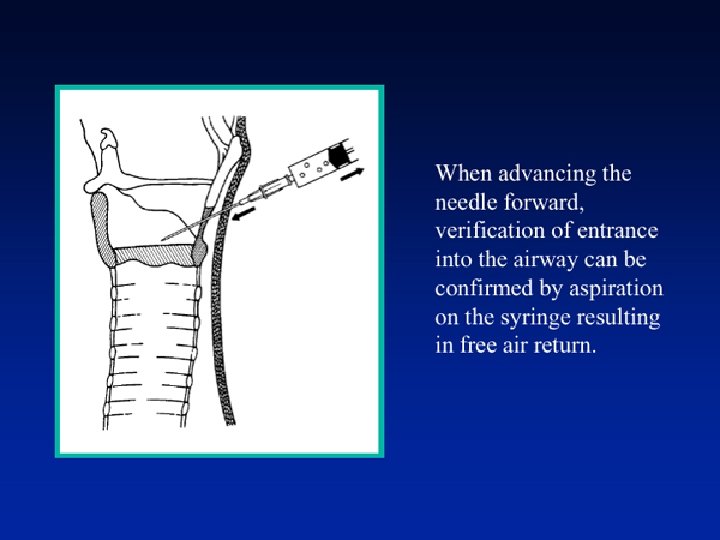
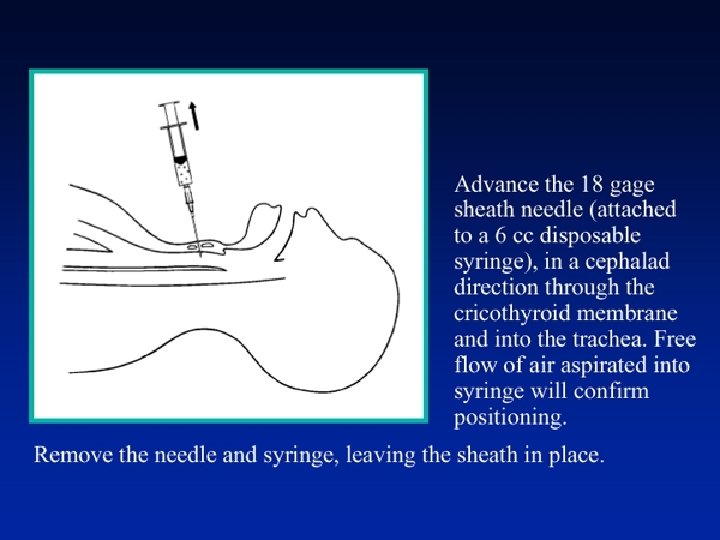
Cricothyroid Membrane Puncture You won’t need to do so for too many times in life. However, you must know how to do it.
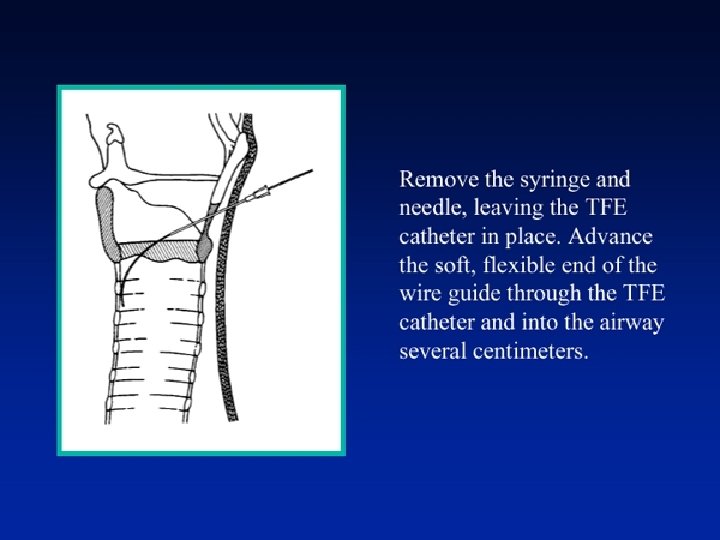
On Hand Technique Use big-bore cath-over-needle (14# or 16#) Attach syringe at the end of the cath, keep gentle negative pressure Puncture caudally until air is withdraw from the syringe Advance needle a little bit with extreme care (much like the way in vascular access) Hold the needle and advance the cath Remove needle, attach syringe to the hub of the cath, aspirate air to ascertain its correct position.
Three Ways to Go Transtracheal jet ventilation (TTJV) Connect to a traditional ventilator Commercial cricothyrotomy kit
Transtracheal Jet Ventilation This can be delivered directly through the cath or (if you have the time) insert a single-lumen CVP catheter by Seldinger technique. Drawbacks: Not always available High risk of complication (barotrauma) Angiocath is prone to kinking Problem shooting: attach a syringe and aspirate air to test (kinking, subcutaneous penetration); auscultation
Transtracheal Jet Ventilation Because of drastic outcome with its complication, you must be very alert all the time when using TTJV. (Complication may occur even when you think ”I’m safe now”. ) So when TTJV is working well, don’t just go away; try some other thing like fiberoptic intubation / call ENT doctor for tracheostomy immediately!!
Settings of TTJV Driving pressure : 50 psi (20 -50 have been proposed as acceptable) I: E ratio = 1: 1~3 Rate: 10~20/min Higher frequency (100~600/min) is for those who have compromised pulmonary function (improving oxygenation along with less barotrauma compared with conventional positive pressure ventilation).
Recovery from TTJV Bucking and glottic closure during TTJV may increase the risk of barotrauma, esp. when short-duration agent (like SCC) is used. Monitoring EMG at forearm is not practical (laryngeal and diaphragmatic muscles are more resistant to muscle relaxants. ); airway pressure tracing was proposed for monitoring. Pay heed to patient’s movement; oral suction regularly while hold TTJV momentarily.
Pros and Cons of TTJV Simpler, quicker, less training required compared with ciricothyrotomy With poor patency of upper airway, gas exhalation can be hindered and lung hyperexpansion ensues increased risk for barotrauma Insert an artificial airway when using TTJV. Decrease the I/E ratio (longer expiration). Use in long procedures is not favored.
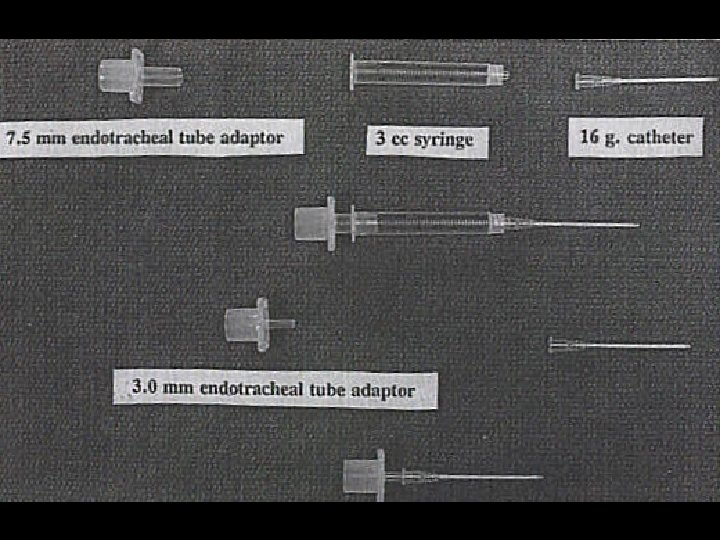
Connect to a Traditional Ventilator Unorthodox method: not generally accepted, better than nothing 1. Connect the hub of the cath to the ventilator via a 3 mm ET tube adaptor. 2. Connect the hub of the cath to a 5 -ml syringe then insert a 7. 0 mm ET tube inside, inflate the cuff, then connect to the ventilator. 3. Connect the hub of the cath to a 3 -ml syringe then insert an adaptor form a 7. 5 mm ET tube inside, then connect to the ventilator
Connect to a Traditional Ventilator Higher respiratory pressure required (mimic TTJV). use O 2 flush button. Self-inflated reservoir bag can be used as well.
Connect to a Traditional Ventilator Problem with the method: high pressure is mostly absorbed by corrugated connection tubing. Pressure limit in some anesthesia machine models
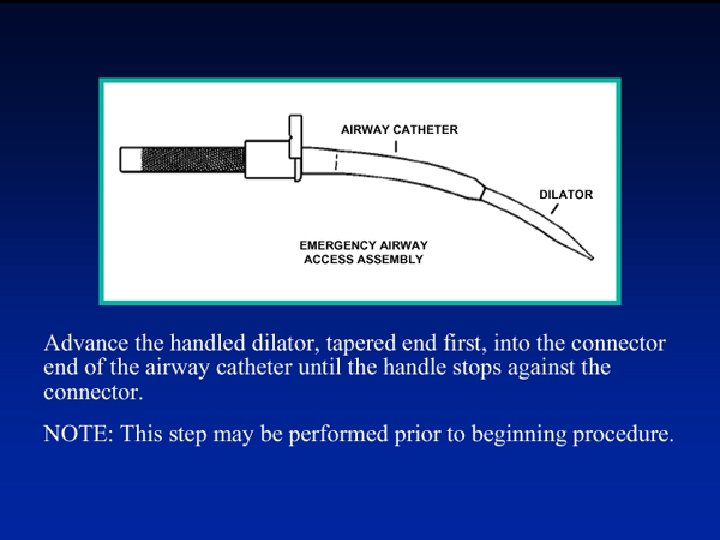
Commercial Cricothyrotomy Kit If you are familiar with this kit, I suggest you try it first. Use Seldinger technique or knife cutting Direct connection to ventilator
Decision Making in Anticipated Difficult Airway (IV) Anticipated Difficult Airway Difficult Mask Ventilation YES Awake Intubation NO Induction Procedures
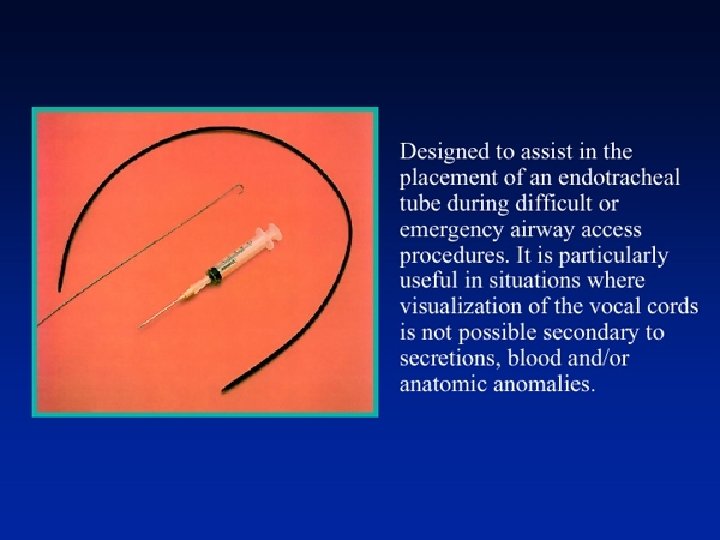
Awake Intubation Take a look with laryngoscope Oral/Nasal fiberoptic intubation Retrograde intubation
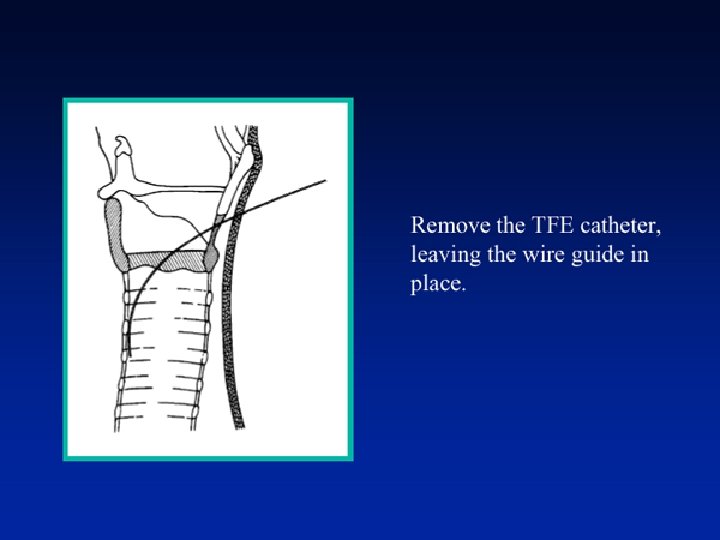
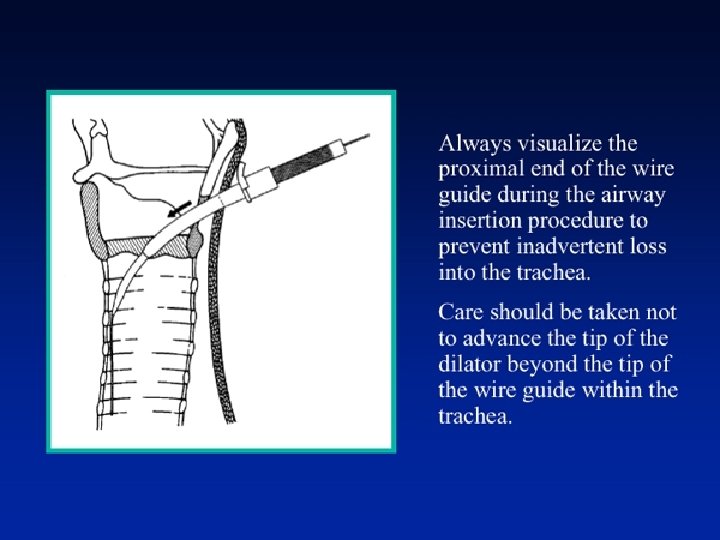
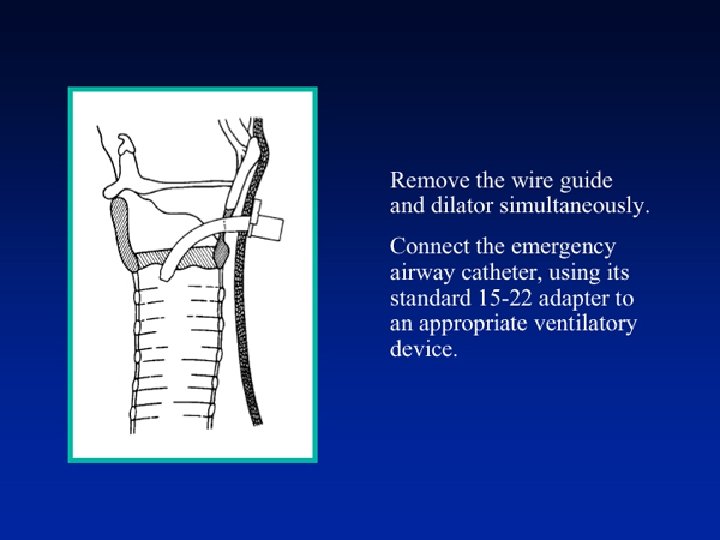
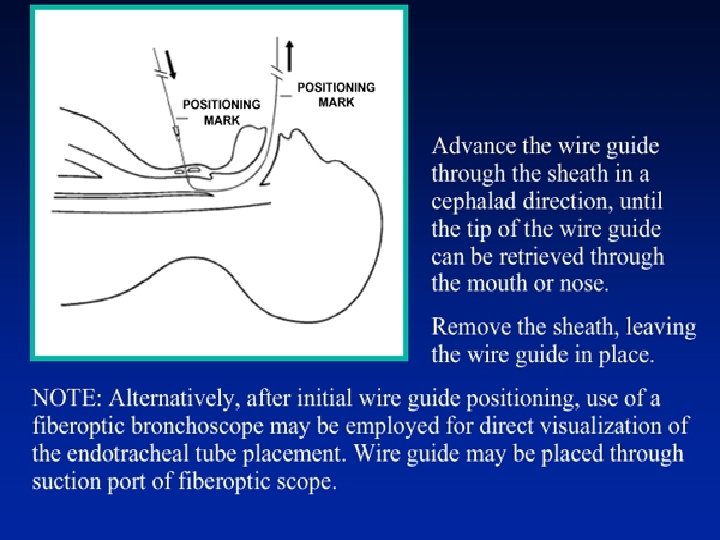
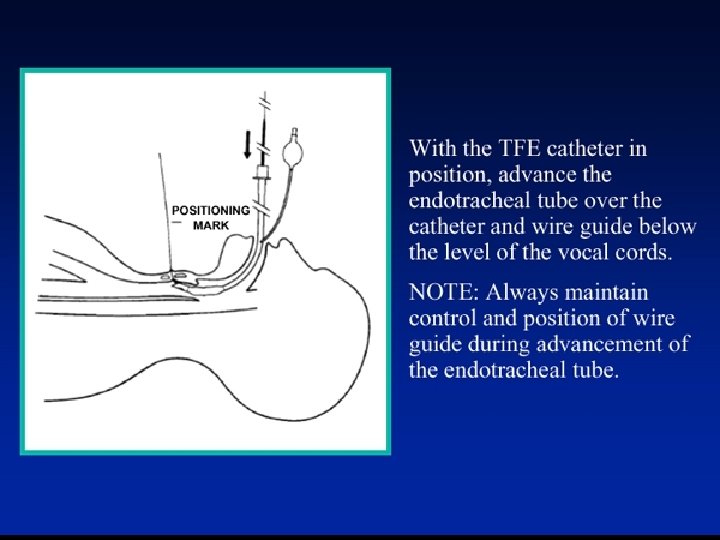
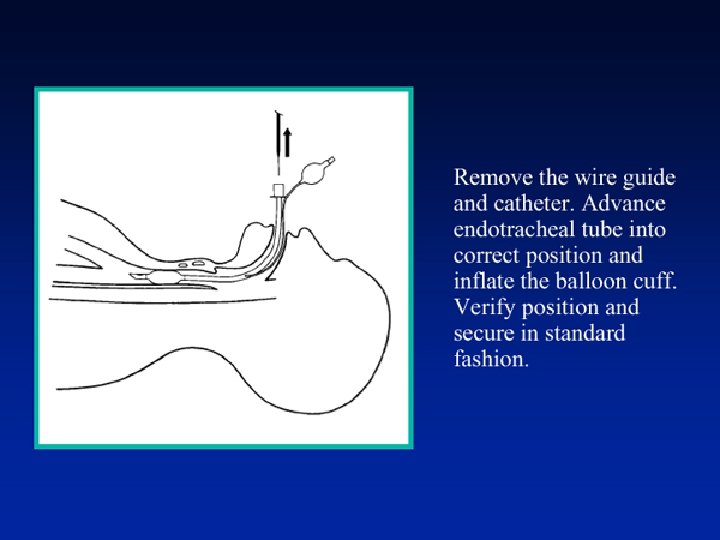
Retrograde Intubation Usually not for emergent conditions (timeconsuming) Puncture site should be close to cricoid cartilage. A smaller ET tube may be easier to slide into the trachea. Do check the position of the tube before you put the patient into sleep. (ET-CO 2!!) The combination with fiberoscope is desirable.
Retrograde Intubation: Risks and Contraindications: 1. Ongoing coagulopathy 2. Obscure cricothyroid anatomy 3. Infection of the cricothyroid membrane 4. Neck mass (i. e. goiter) Risks: bleeding in the airway ET tube may not pass easily into the larynx.
TFE catheter: prevent the ET tube form redundancy over the guidewire decrease trauma, increase success rate
Retrograde Intubation with the Aid of Fiberoscope 1. Guidewire goes through Murphy eye; fiberoscope goes through main lumen. OR 2. Thread guidewire through the suction lumen of the fiberoscope.
Highlights for Part II Lightwand intubation Laryngeal mask airway Awake fiberoptic intubation ASA algorithm for difficult airway Exclusion of Esophageal Intubation