Management of Bone Mineral Disorder in Dialysis Patients

Management of Bone Mineral Disorder in Dialysis Patients 2013. 4. 10 fellow 우성애

CKD-MBD � Systemic disorder of mineral & bone metabolism due to CKD � Abnormalities of Ca, P, PTH or Vit. D metabolism � Abnormalities in bone turnover, mineralization, volume, linear growth, or strength � Vascular or other soft tissue calcification
2 D 3 감소 Resistance of")
Pathogenesis Renal function감소 Phosphate retention FGF-23 Klotho 1, 25(OH)2 D 3 감소 Resistance of bone to PTH hypocalcemia hyperparathyroidism Ca sensor 감소 Klotho-FGFR 1 Rc complex 감소 1, 25(OH)2 D 3 receptors 감소

� In mild to moderate CKD, a normal serum phosphate concentration does not necessarily indicate normal parathyroid status � Efforts to control phosphate, including dietary phosphate restriction and the use of phosphate binders should not be delayed until frank hyperphosphatemia develops. => CKD 3부터 MBD에 대한 평가 및 조절필요

Hyperphosphatemia

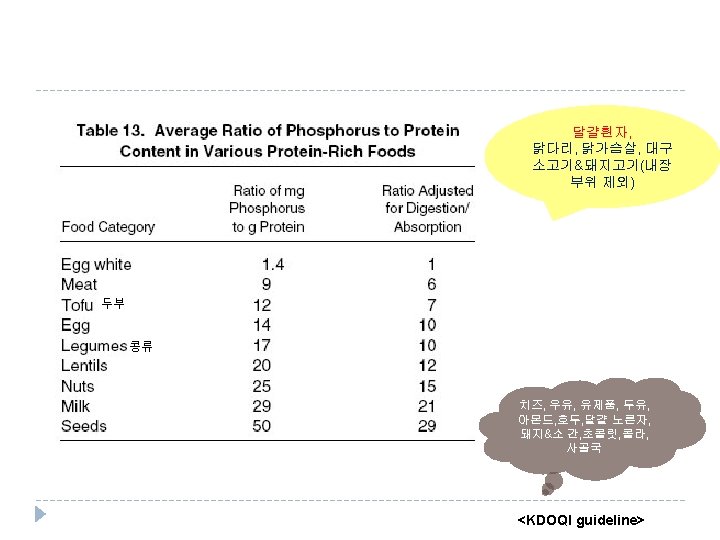
Phosphate Metabolism in Kidney Failure and in Health <NEJM 2010; 362: 1312 -24>

Dietary P restriction <IJKD 2010; 4: 89 -100>

Phosphate binder <comprehensive clinical nephrology>
 � ~ mid 1980 s, mainstay � Systemic aluminum")
Phosphate binder � Aluminum containing(Amphojelⓡ) � ~ mid 1980 s, mainstay � Systemic aluminum toxicity; encephalopathy, dementia, osteomalacia, anemia, GI side effects(esp. renal insufficiency) � short period, 40 -45 mg/kg/d이하, Ca containing binder의 사용에 제한이 있 을때(hypercalcemia, extensive vascular calcification, calciphylaxis)

� Ca based phosphate binders - Taken with meals effectively binds phosphates and limits their absorption - Doses may vary according to the patient’s compliance with dietary phosphate restriction as well as the CKD stage - element Ca intake; max 1500 mg/d(diet + binder; 2000 mg/d미만) - 문제점: hypercalcemia-associated risks including extraskeletal calcification and PTH suppression; adynamic bone disease > bone의 buffer capacity 감소하여 soft tissue Ca침착 증가, 심혈관 예후 악화 - Avoid : bone turnover감소(PTH persistently low, <150), hypercalcemia(Ca >10. 2), vascular calcification
 � Sevelamer hydrochloride(renagelⓡ); metabolic")
� Sevelamer � Non-absorbable, Anion-exchange resin(칼슘, 금속 기반 아닌 인결합제) � Sevelamer hydrochloride(renagelⓡ); metabolic acidosis sevelamer carbonate � Ca based binder와 비교시 low Hypercalcemia incidence & vascular calcification, but mortality 차이없음 <"Treat-to-Goal" trial> Ø Ø � Lower incidence of hypercalcemia (5 vs. 16%) Decreased incidence of low PTH levels (30 vs. 57%) Lower LDL-C (65 vs. 103 mg/d. L) Much lower % increases in median absolute Cascores in coronary arteries (5 vs. 25%) & aorta (5 vs. 23%) <Kidney Int 2002; 62: 0245 -252> Sevelamer may be combined c Ca containing binders if necessary
 � � 금속 기반의 인결합제, sevelamer에 비해 적은양 복용, chewable")
� Lanthanum carbonate (Fosrenolⓡ) � � 금속 기반의 인결합제, sevelamer에 비해 적은양 복용, chewable cleared primarily by the liver some lanthanum appears to accumulate in bone and liver Expensive -sevelamer 800 mg/1 T 880원 > 2. 4 g/d복용시 79200원/mo -Lanthanum 500 mg/1 T 1270원 (Ca. CO 3 500 mg 1 T 30원 > 1. 5 g(element Ca 600 mg)/d 복용시 2700원/mo) � 보험기준 투석을 받고 있는 ESRD 환자중 혈액검사상(매월 1회정도) 혈중 인(P) 수치가 5. 5㎎/㎗ 이상이면서 Ca× P산물(product)이 55 mg 2/㎗ 2 이상인 환자에게 인정

� calcium-containing phosphate binders remain a cost-effective firstline treatment option for the control of hyperphosphatemia, although the risk of long-term calcium exposure remains a concern. � Limiting calcium-containing phosphate binder use persistent hyperphosphatemia even in combination with calciumcontaining binders sevelamer may be most appropriate.

KDOQI & KDIGO guideline 2003 KDOQI 2009 KDIGO CKD 3 -4 CKD 5 Ca normal 8. 4 -9. 5 mg/d. L maintain normal range P 2. 7 -4. 6 3. 5 -5. 5 mg/d. L maintain normal range towards normal range (dialysis) PTH 35 -70 (CKD 3) 70 -110(CKD 4) 150 -300 pg/ml 2 -9 times the upper limit of normal Ca x P <55 25(OH) Vit. D Not recommended in CKD stage 5 maintain within 30 -100 ng/ml Ca x P ; extraskelet al calcification 의 risk factor

< 8. 4 ≤ ~ < 9. 5 ≤ ~ < 10. 2≤ <3. 5 CACA/CAAC식후 1시간 No (CACA 쓰던경우 유지) No (CACA 쓰던경 우 감량) No (CACA 쓰던경 우 중지) 3. 5≤ <5. 5 CACA/CAAC식후 1시간 No (CACA 쓰던경우 유지) No (CACA 쓰던경 우 감량) No 5. 5≤ <7. 0 & Ca x P < 55 CACA/CAAC 3 T with meal NO 5. 5 ≤ <7. 0 & Ca x P ≥ 55 Renagel 800 mg tid & CACA/CAAC식 후1시간 Renagel 800 mg tid Renagel 1600 mg tid & CACA/CAAC식 후1시간 Renagel 1600 mg tid Ca P 7. 0 ≤ <삼성 서울병원 가이드라인

< 8. 4 ≤ ~ < 9. 5 ≤ ~ < 10. 2≤ <3. 5 CACA/CAAC식 후1시간 No (CACA 쓰던경 우 유지) No (CACA 쓰던경 우 감량) No 3. 5≤ <5. 5 CACA/CAAC식 후1시간 No (CACA 쓰던경 우 감량) No 5. 5≤ <7. 0 & Ca x P < 55 CACA/CAAC 3 T with meal No Ca x P ≥ 55 5. 5 ≤ <7. 0 Renagel 800 mg tid 7≤ Renagel 1600 mg tid Ca P * 7 ≤ P & Ca x P < 55: Renagel 1600 mg tid(비보험), aluminum based binder고 려 <순천향 서울병원 가이드라인

<NEJM 2010; 362: 1312 -24>

Treatment of abnormal PTH level
 � Calcimimetics � � parathyroidectomy")
Secondary hyperparathyroidism VDRA(Vit D receptor activator) � Calcimimetics � � parathyroidectomy
, (Rocaltrolⓡ) - � Paricalcitol(19 -nor-1 -alpha,")
Vitamin D therapy � Calcitriol(1, 25 -dihydroxyvitamin D), (Rocaltrolⓡ) - � Paricalcitol(19 -nor-1 -alpha, 25 -dihydroxyvitamin D 2; Zemplarⓡ) � � � Parathyroid gl의 the vitamin D receptor (VDR) 에 작용하여 PTH transcription을 억제, Parathyroid cell 증식 감소 뼈와 장에서 칼슘 흡수 증가시켜 혈청 칼슘을 증가 -> PTH분비 억제. Hypercalcemia, hyperphosphatemia, vascular calcification, adynamic bone dz "second generation" vitamin D analogue. Selective VDRA less severe increments in serum calcium and phosphate (prospective randomized trial is needed) Vitamin D derivatives should not be given until the serum phosphate con has been controlled (<5. 5 mg/d. L) and the serum calcium is less than 9. 5 mg/d. L : metastatic calcification risk (P <5. 5 & Ca<9. 5 가 아니라면 vitamin D 투여 금기)
")
Calcimimetics � acts as a positive allosteric modulator of the Ca sensing Rc(Ca. R) , increase the sensitivity of the Ca. R in the parathyroid gland to calcium

Calcimimetics � Efficacy: Cinacalcet added to standard therapy facilitates the achievement of the Kidney Disease Outcomes Quality Initiative (KDOQI) clinical practice guidelines 56% vs 10% 46% vs 33% 42% vs 24% 41% vs 6% <Kidney Int.
 � Indication patients with PTH >300 pg/m. L, s. Ca >")
Calcimimetics � Cinacalcet(Regparaⓡ) � Indication patients with PTH >300 pg/m. L, s. Ca > 8. 4 mg/d. L � Dose Starting dose 30 mg/d, stepwise increments to 60, 90, 180 mg/d q 4 wks � should not be started if serum calcium is below 8. 4 mg/d. L
- Slides: 24