Management of Barretts Esophagus Joint Hospital Surgical Grand

Management of Barrett’s Esophagus Joint Hospital Surgical Grand Ground 17 th July 2010 Dr KS Chan Queen Elizabeth Hospital

Barrett’s Esophagus n n Metaplastic change in the distal esophageal lining Normal squamous epithelium replaced by columnar epithelium Named after Dr Norman Rupert Barrett q Incorrect description q “Congenitally short esophagus with tubular intrathoracic stomach” First description by Wilder Tileston dated back to 1906 Norman Rupert Barrett (1903– 1979)

n Prevalence q q n n 1. 6 -5. 6% in general population 10 -15% in patients with reflux symptoms Premalignant condition Associated with esophageal adenocarcinoma q q q 0. 5 -1% per patient-year 30 -40 fold increased risk compared to general population 10 -15% per patient-year in BE with high grade dysplasia

Risks factor n n n Gastroesophageal reflux Obesity Male sex Advanced age White race

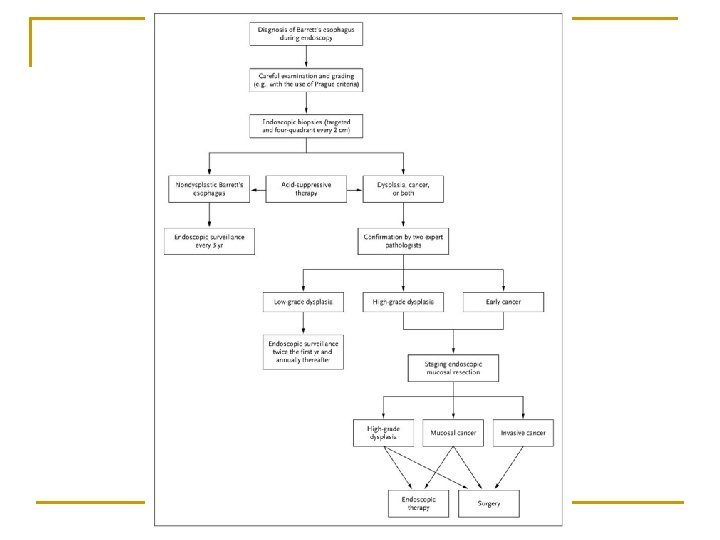
Diagnosis n White light endoscopy q n Salmon-coloured epithelium projects into the tubular esophagus Systematic biopsy q q 4 quadrant biopsies every 2 cm in the columnar segment Additional biopsies from any mucosal abnormalities or visible lesions

Advances in Imaging n n n High resolution white light microscopy Chromoendoscopy Narrow band imaging Autofluorescence imaging Confocal laser endomicroscopy Spectroscopy

Management n n n Most patient with Barrett’s esophagus do not progress Confirm the diagnosis Non-dysplastic disease or low grade dysplasia q n Managed conservatively High grade dysplasia q q Increase risks of progression to cancer Intervention advocated

Treatment of Barrett’s Esophagus n Anti-reflux treatment q q n Endoscopic Therapy q q n Proton Pump Inhibitor Fundoplication Ablative: Photodynamic therapy, Argon plasma coagulation, laser, cryotherapy, radiofrequency ablation, mutlipolar electrocautery Resection: Endoscopic mucosal resection, Endoscopic submucosal dissection Surgical Therapy q Esophagectomy

Photodynamic Therapy n n Most extensively studied Use of photosensitizer which acculumates in malignant and pre-malignant tissue q n n n Porfimer sodium, aminolevulinic acid Exposure to light of appropriate wavelength Production of singlet oxygen and reactive oxygen species Cell damage and apoptosis
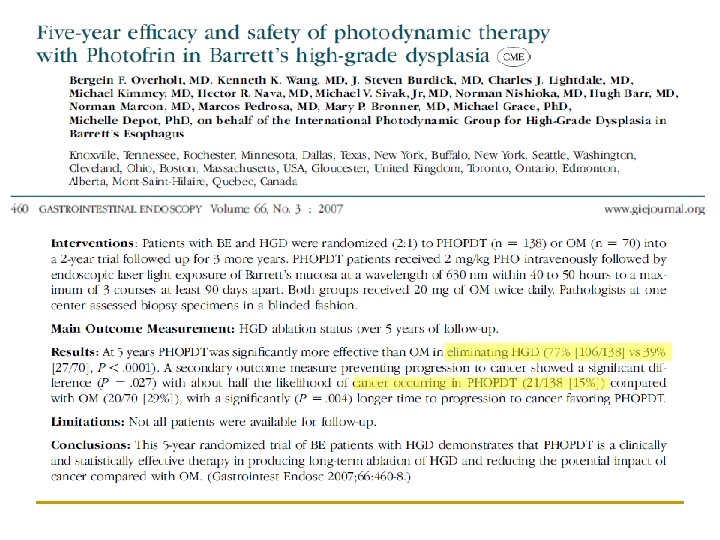

n n 69% of the subjects who received PDT developed photosensitivity reactions 36% developed esophageal strictures that required dilation therapy n First RCT showing reduction in adenocarcinoma risks in BE patients with any therapeutic intervention n 5 -ALA better tolerated with fewer complications

Radiofrequency Ablation n n High power radiofrequency energy generator, sizing balloon catheters and ablation catheters Penetration 0. 5 mm

n n n Treatment repeated every 2 -3 months All visible BE eradicated After final treatment session, biopsy taken over the original BE segment to exclude buried Barrett’s
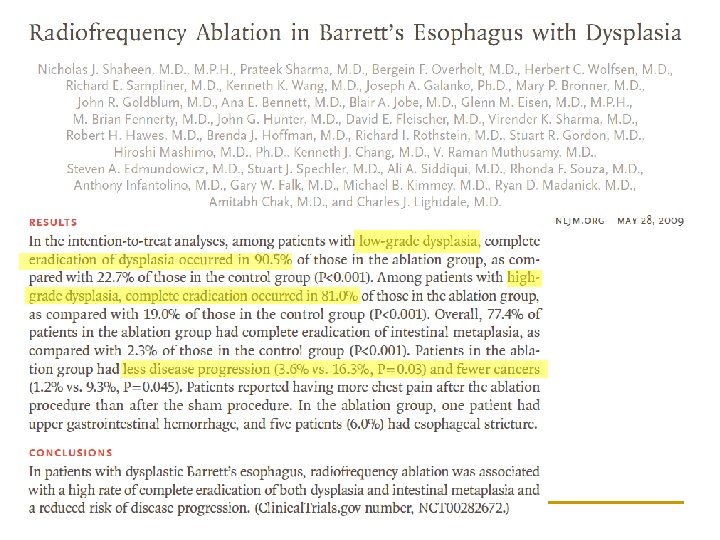

n n Promising treatment modality Side effect q Esophageal stricture, GI bleeding and chest pain n Substantially lower than those in photodynamic therapy n Long term data needed
 and Endoscopic submucosal dissection (ESD) Provide")
Endoscopic Resection n n Endoscopic Mucosal Resection (EMR) and Endoscopic submucosal dissection (ESD) Provide specimen for histopathological assessment Size of specimen resected by EMR limited to ~2 cm each attempt ESD enable en bloc resection of lesion regardless of size

EMR n n “Suck and cut” method Complications q q q Bleeding Perforation Stricture

Endoscopic Therapy n n n No single therapy achieve complete eradication without complications Recurrence Buried metaplasia q n Partially ablated Barrett’s epithelium healed with overlying squamous epithelium Applicable to lesion confined to mucosa only q Breach muscularis mucosae, >20% LN metastasis

Surgical Treatment n n n Esophagectomy considered as the ‘gold standard’ for high grade dysplasia and early adenocarinoma Morbidity and mortality Reported mortality rate ranges from 2% (Reed 2005), up to 20% post-operatively (Urba 2001)

Which is the best treatment? n n Currently no randomized controlled trials Only 6 restrospective, non-randomized trials q All with no significant difference in survival n Difficult to draw definitive conclusion n Should be individualized Considering age, co-morbidities, life expectancy and extent of disease n

Conclusion n n Barrett’s esophagus is a pre-malignant condition Diagnosis relies on both endoscopic and histological findings Management should be based on risks stratification Emerging evidence on the use of endoscopic therapy Treatment should be individualized

Thank You
- Slides: 23