MANAGEMENT OF ATRIAL FIBRILLATION 2019 Pro Dr Yadav

MANAGEMENT OF ATRIAL FIBRILLATION - 2019 Pro. Dr. Yadav Bhatta (MD, DM, DNB, FACC, FAPSIC) Director Department of Cardiology NORVIC International Hospital

WHY WORRY ABOUT AF • HEART FAILURE – ACUTE, CHRONIC • CARDIAC REMODELLING • THROBO EMBOLISM • DEMENTIA

Stroke risk related to various cardiac conditions Framingham study - Wolf et al. Stroke 1991; 22: 983– 98

Outcomes • Mortality: doubled • Stroke: increased 5 fold. More severe • Hospitalization: more frequent • Quality of life: wide variation, from no change to marked reduction. • Congestive heart failure: wide variation from none to severe(tachy myopathy)

AF- SYSTEMIC DISEASE

Triggers Haïssaguerre M et al. N Engl J Med 1998; 339: 659 -666.

Natural History

NATURE HISTORY OF AF

ATRIAL FIBRILLATION • DETECTION • DIAGNOSIS • MANAGEMENT

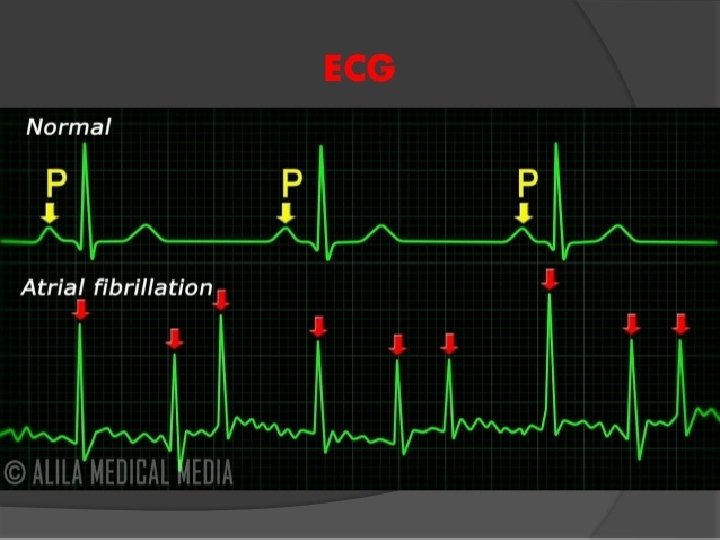
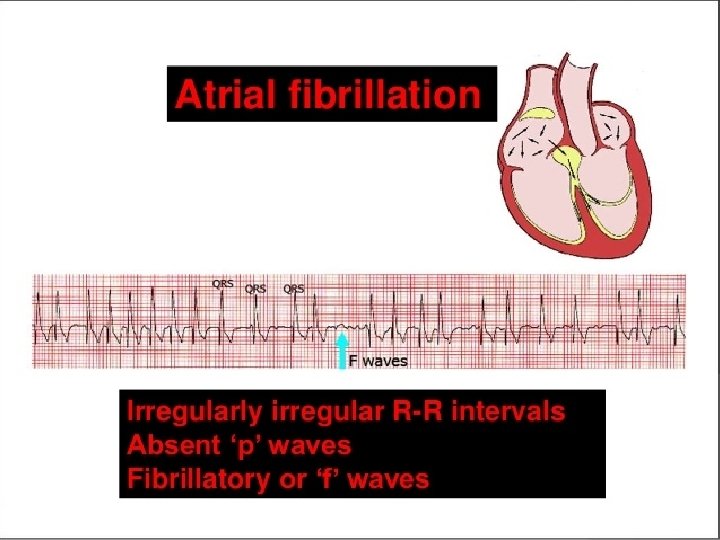
Detection • An irregular pulse or irregular heart beat on auscultation should raise suspicion • ECG is necessary to diagnose AF. • Any arrhythmia that has the ECG characteristics of AF and lasts sufficiently long for a 12 -lead ECG to be recorded, or at least 30 s on a rhythm strip, should be considered as AF. • Holter (24 -48 hrs) • Event monitors (upto 1 month) • Dual chamber pacemakers and defibrillators. • Implantable loop recorder (upto 3 yrs)

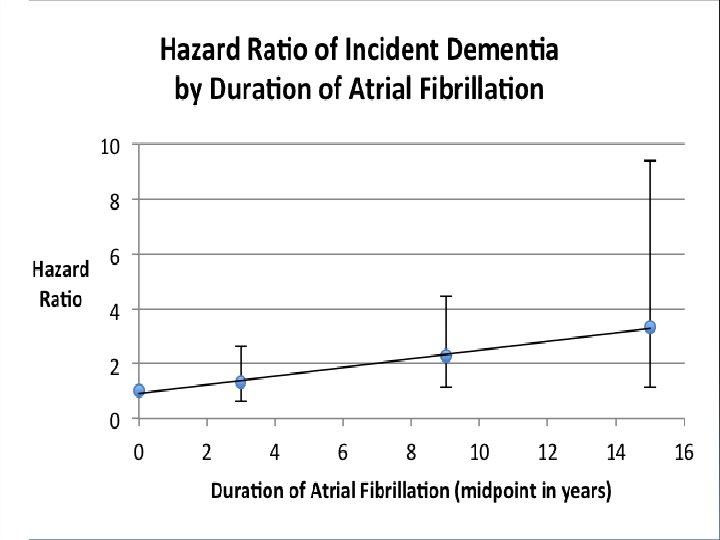
Dementia prevention

CHRONIC MANAGEMENT 1. RATE CONTROL • MANAGEMENT OF PRECIPITATING FACTORS • LIFESTYLE MODIFICATION 2. ANTICOAGULATION

ANTICOAGULATION

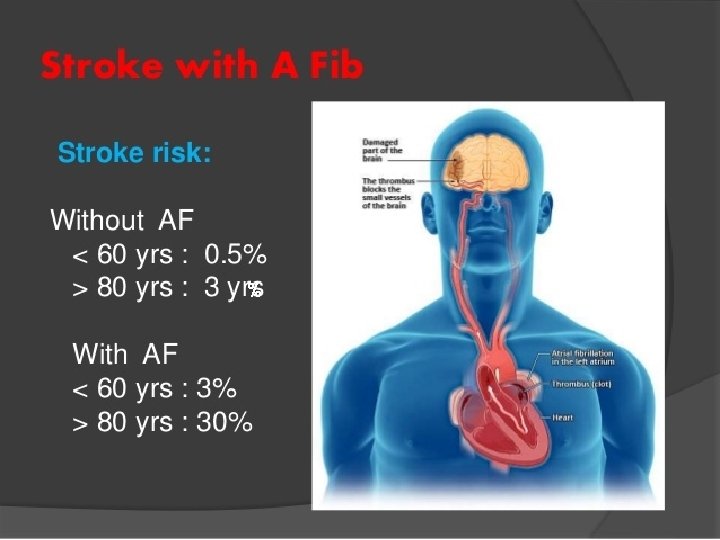

Anticoagulation • AF increases the risk of stroke by five-fold • Stroke in atrial fibrillation more disabling. • Anticoagulation reduces stroke risk by twothirds • Anticoagulation only treatment shown to reduce mortality in AF • Antiplatelet therapy reduces stroke risk by one -fifth

Incidence of major bleeding events with warfarin and enoxaparin Braidy et. Al. 2011

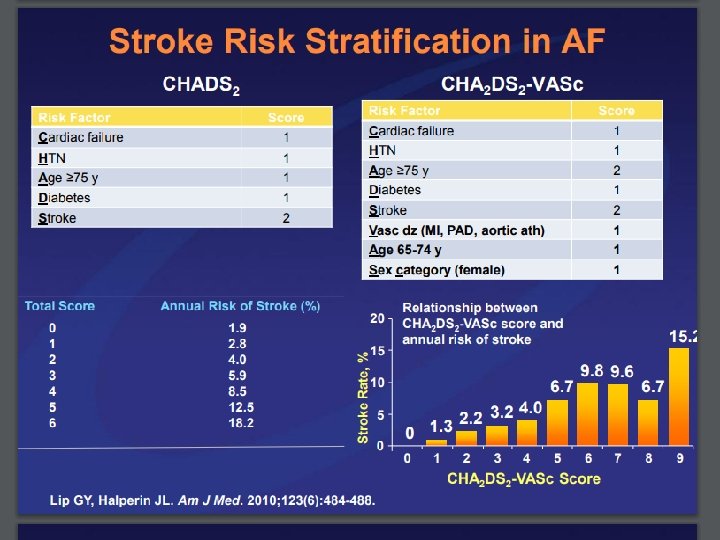
CHADS 2 Score • Evolved from the AF investigators and SPAF investigators criteria. • Initial rapid and easy to use means of assessing stroke risk. • CHADS 2 score of 0, an adjusted rate of 1. 9 per 100 pt yrs • Stroke rate increased by a factor of 1. 5 for each 1 -point • Recommendations low risk (score 0): No anticoagulation moderate risk (score 1) Aspirin or oral anticoagulation high risk (score >/= 2) Oral anticoagulation - Gage et al, JAMA. 2001; 285: 2864 2870

CHADS 2 Score - limitations • Too many patients classified as moderate risk • Even pt at mod risk (CHADs 2 =1) benefit from anticoagulation over aspirin • Did not include many stroke risk factors

CHA 2 DS 2 -VASc Score Lip et al, Chest 2010; 137: 263– 272

Recommendations • CHA 2 DS 2 -VASc score of 0, reasonable to omit antithrombotic therapy. • CHA 2 DS 2 -VASc score of 1, no antithrombotic therapy or treatment with an oral anticoagulant or aspirin may be considered. • CHA 2 DS 2 -VASc score of 2 or greater, oral anticoagulants are recommended • CHA 2 DS 2 -VASc score of 2 or greater and who have endstage CKD (Cr. Cl <15 m. L/min) or are on hemodialysis, it is reasonable to prescribe warfarin (INR 2. 0 to 3. 0) for oral anticoagulation.

Hart et al, Ann Intern Med. 2007; 146: 857867

Adjusted dose warfarin vs placebo/control 64%% - Hart et al, Ann Intern Med. 2007; 146: 857 -
 absolute risk")
Hart et al Stroke reduction Warfarin: 64% (95% CI, 49% to 74%) absolute risk reduction: 2. 7% per year Aspirin: Nonsignificant 19% (CI, -1% to 35%) absolute risk reduction: 0. 8% per year Warfarin vs antiplatelet therapy: 37% (CI, 23% to 48%) Major Bleeding warfarin vs aspirin: risk for intracranial hemorrhage doubled absolute risk increase small (0. 2% per year) Mortality warfarin versus control: all-cause mortality substantially reduced (26% [CI, 3% to 43%])

No. ACs vs Warfarin Limited reversal agents

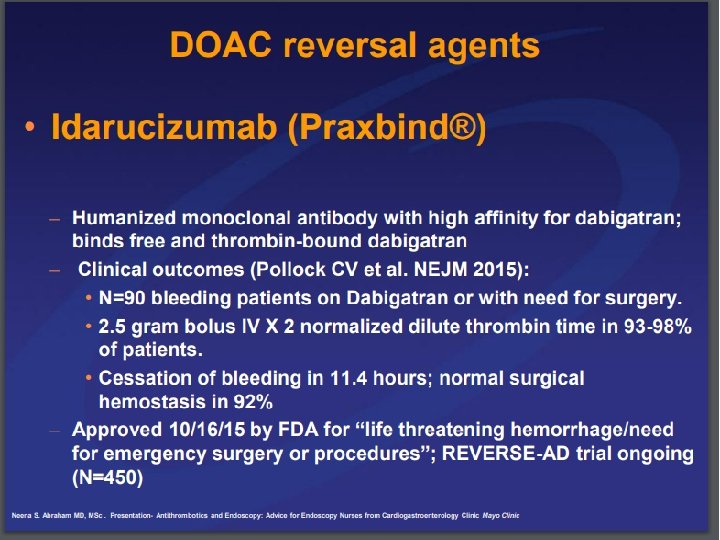
Dabigatran • Direct Thrombin Inhibitor • Alternative to warfarin for CHADS 2 Va. Sc of 2 or greater in those with nonvalvular afib • RE-LY Trial: 150 mg dose superior to warfarin in preventing ischemic stoke with no difference in bleeding • Praxbind ® (idarucizumab) is a specific reversal agent for Pradaxa

RELY

Rivaroxaban • Oral factor Xa inhibitor • Rocket AF: noninferior to warfarin for stroke prevention • no significant difference in risk of major bleeding • intracranial and fatal bleeding occurred less frequently • Antidote: FDA approves Andex. Xa

Rocket AF

Apixaban • Oral factor Xa inhibitor • Aristotle : superior to warfarin in preventing stroke • caused less bleeding • resulted in lower mortality • Antidote: FDA approves Andex. Xa • Dose Adjustment: Cr >1. 5, Age > 80, Wt < 60 kgs

Aristotle

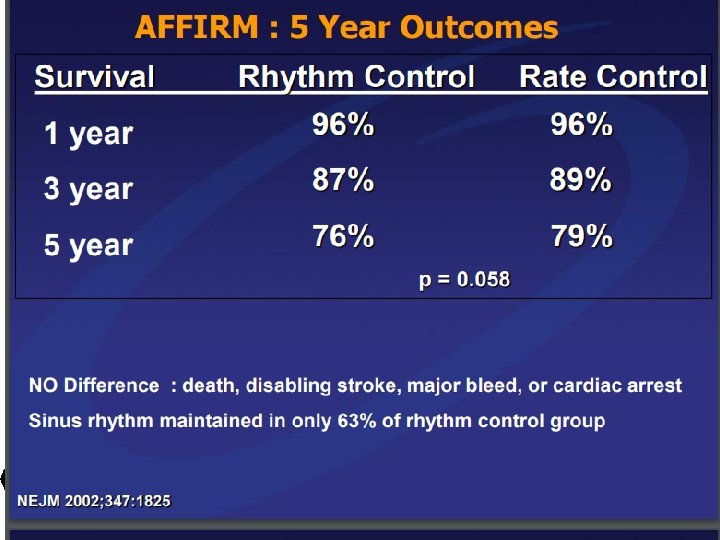
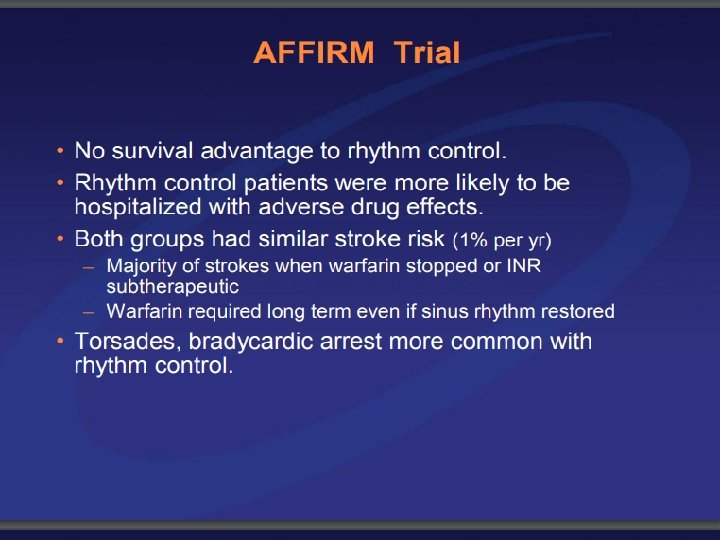
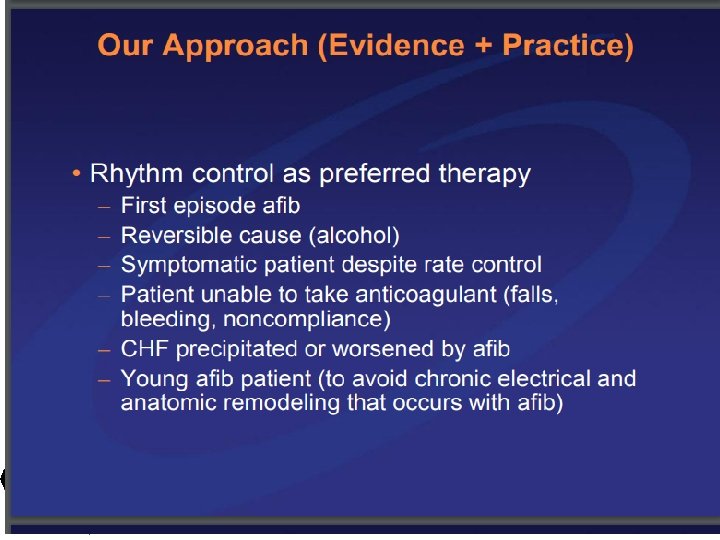
AF- RATE vs RHYTHM CONTROL
. Warfarin use")
Sinus Rhythm associated with decreased risk of death (HR 0. 53). Warfarin use associated with decreased risk of death (HR 0. 50) AADs associated with increased mortality only after adjustment for the presence of SR(HR 1. 49). AADs are not associated with improved survival, which suggests that any beneficial antiarrhythmic effects of AADs are offset by their adverse effects. If an effective method for maintaining SR with fewer adverse effects were available, it might be beneficial.

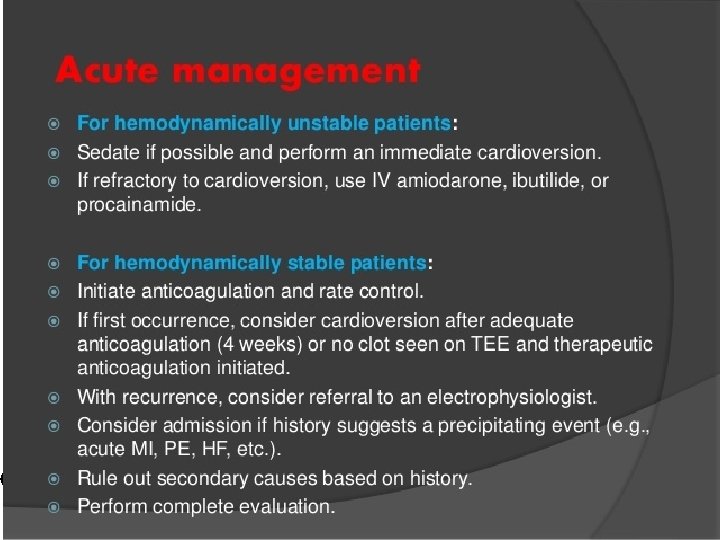
CARDIOVERSION

Catheter ablation for AF

Guidelines Indicated in patients with • Symptomatic paroxysmal AF refractory or intolerant to at least 1 antiarrhythmic medication when a rhythmcontrol strategy is desired (1 A) • Symptomatic persistent AF refractory or intolerant to at least 1 antiarrhythmic medication. (2 A) • Recurrent symptomatic paroxysmal AF, catheter ablation is a reasonable initial rhythm-control strategy. (2 A)

AV node ablation

AV node ablation Guidelines • AV nodal ablation with permanent ventricular pacing is reasonable to control heart rate when pharmacological therapy is inadequate and rhythm control is not achievable. (IIA)

AV node ablation • provides highly effective control of ventricular rate • patients in whom pharmacological rate control has failed and rhythm control with drugs and/or LA ablation has failed. • improves quality of life • reduces mortality • patients with reduced LV function may require biventricular pacing after atrioventricular node ablation.

Left atrial appendage occlusion • Watchman device only FDA approved percutaneous LAA closure device • semi-spherical nitinol frame with a polyethylene terephthalate membrane coating • deployed transseptally using a dedicated 14 Fr sheath usually under transesophageal echocardiography and fluoroscopic guidance.

Recommendations FDA approved for patients • at increased risk of stroke and systemic embolism based upon CHADS 2 or CHA 2 DS 2 -VASc scores • deemed by their physicians to be suitable for warfarin therapy • have an appropriate rationale to seek a nonpharmacological alternative to warfarin

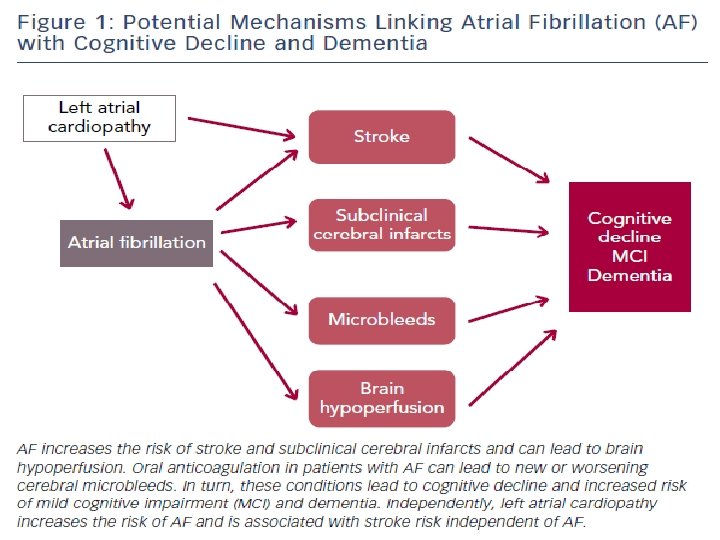
AF & DEMENTIA

Thank you dryadavbhatta. com. np
- Slides: 70