MANAGEMENT OF ACUTE EXACERBATION OF COPD DR SADIYA

MANAGEMENT OF ACUTE EXACERBATION OF COPD DR. SADIYA NOUSHEEN PATEL FCCCM PART-2 GGSMH, MYSORE

INTRODUCTION �Third leading cause of death. �Increase morbidity and mortality. �In-hospital mortality of 3 -8 % and a 30 -day mortality of 14 -26%.

DEFINITION: An exacerbation of COPD is defined as, an event in the natural course of the disease characterised by a change in the patients baseline dyspnea, cough and/or sputum that is beyond normal day-to-day variations, is acute in onset and may warrant a change in regular medications.

RISK FACTORS FOR COPD �Smoking �Occupational exposure �Environmental pollution �Alpha-1 antitrypsin deficiency �Bio mass �Co-morbidities �Respiratory infections �Socioeconomic status �Nutrition

PRECIPITANTS OF ae. COPD �Infective, including Aspiration. MC being Strep. pneumonia, H. influenza -8 O% Others being S. viridans, mycoplasma pneumonia, pseudomonas etc… �Left ventricular failure �Sputum retention �Pulmonary embolism �Sleep apnoea etc…

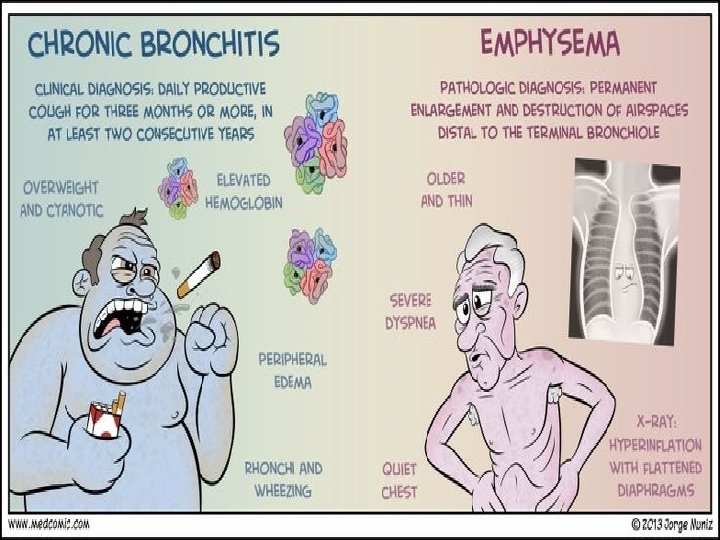
PATHOGENESIS �Inhaled cigarrette smoke and other noxious particles such as smoke from biomass fuel cause lung inflammation. �This chronic inflammatory response may induce parenchymal destruction and disrupts normal repair and defense mechanisms. �In addition to inflammation, an imbalance between proteinases and antiproteinases and oxidative stress are also important in the pathogenesis of COPD.

�The different mechanisms give rise to: ü mucous hypersecretions and ciliary dysfunction. ü Airflow limitation and hyperinflation ü Gas exchange abnormalities ü Pulmonary hypertension ü Systemic effects.

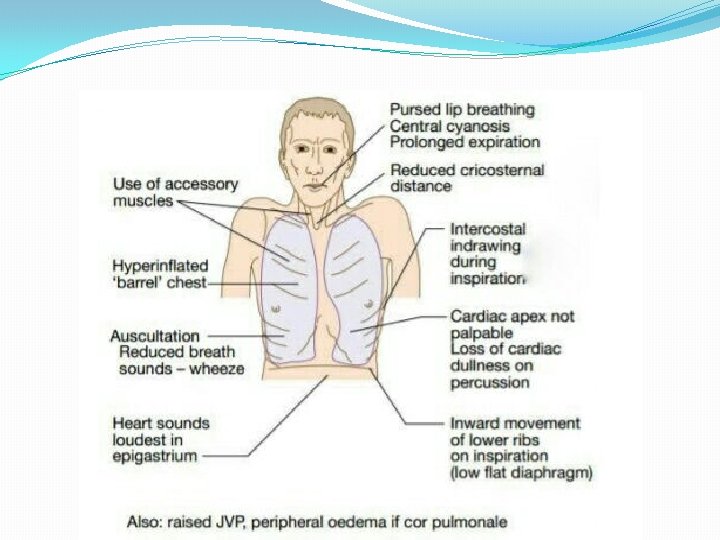
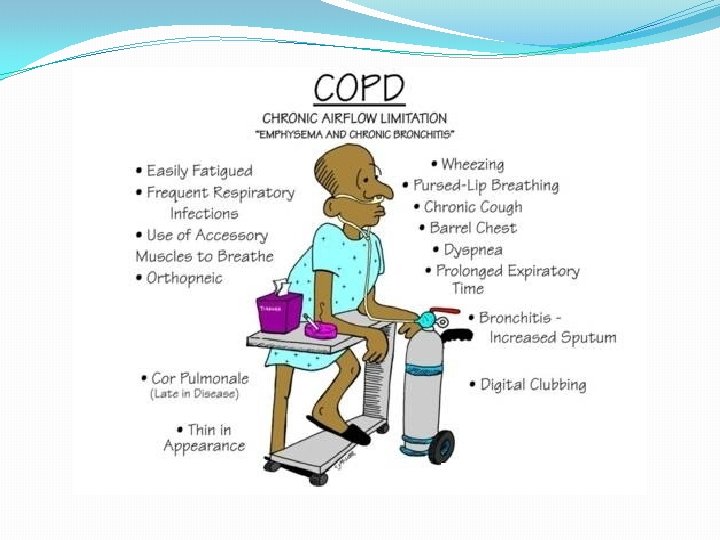
SIGNS AND SYMPTOMS

COR PULMONALE � May be secondary to chronic pulmonary problems. � Fatigue � Distended jugular veins � Anorexia and GI distress � Ascitis � Increased peripheral venous pressure � Hepatosplenomegaly � Weight gain � Pedal edema.

ASSESSMENT OF RISK �By history and spirometry: �Two or more exacerbations within the last year or an FEV 1 <50% of predicted value �One or more hospitalizations for COPD exacerbation
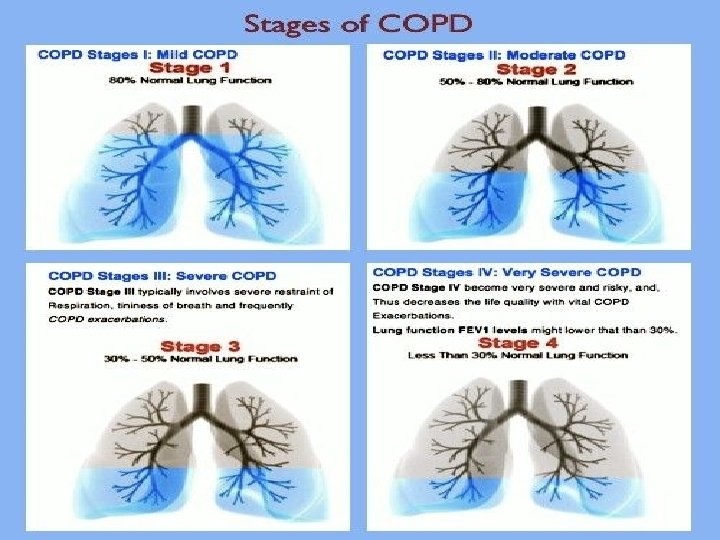
 � 1 � 2 � 3 � 4")
GOLD STAGING SCORE FEV 1/FVC (%) � 1 � 2 � 3 � 4 < 70 FEV 1 (%) �> 80 � 50 - 80 � 30 - 50 �< 30

BODE INDEX �Body mass index �Airflow obstruction �Dyspnoea �Exercise capacity Max. score is 10 4 yr survival rate is, Ø 80% for Score of 2 Ø 70% for 3 -4 Ø 60% for 5 -6 Ø 20% for 7 -10
 > 65 50 - 64 Six min walk distance")
SCORE O FEV 1 (%) > 65 50 - 64 Six min walk distance > 350 250 - 350 Mod. MRC dypnea score 0 - 1 2 > 21 < 21 BMI 1 2 3 36 - 49 < 35 150 - 250 < 150 3 4

GOALS OF MANAGING AN ACUTE EXACERBATION ü To reduce the symptoms, Ø By relieving symptoms Ø By improving exercise tolerance Ø By improving health status ü To reduce risk Ø By preventing disease progression Ø Preventing and treating exacerbations Ø By reducing mortality

INVESTIGATIONS �SPIROMETRY is the gold standard. �It should be performed after the administration of an adequate dose of Short-acting inhaled bronchodilator to minimize variability. FEV 1/FVC <0. 70 , confirms airflow limitation.

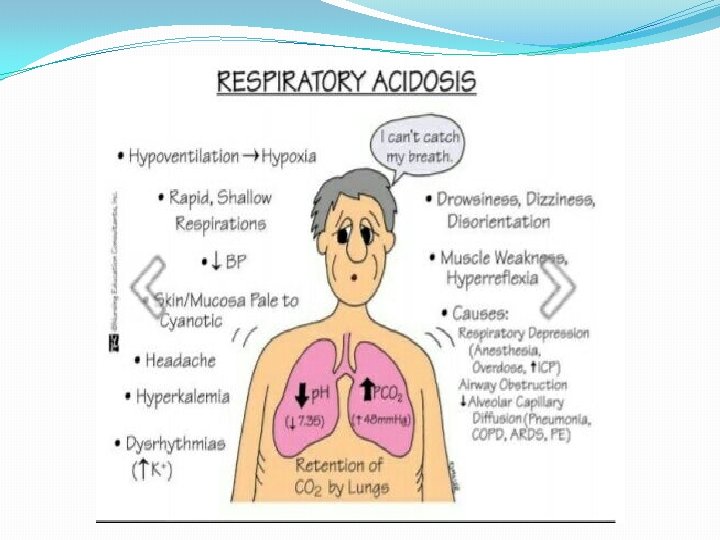
�ABG - Pa. O 2 <8. 0 k. Pa with or without Pa. CO 2>6. 7 k. Pa when breathing room air indicates Respiratory failure. �CHEST RADIOGRAPH: To exclude other diagnosis, near normal except increased broncho vascular markings. �ECG- helps in diagnosis of coexisting cardiac problems. �ECHOCARDIOGRAPHY- to diagnose Corpulmonale by measuring PASP

�CBC- To r/o. infective origin of COPD �SPUTUM- for AFB, Gram stain and culture �BIOCHEMICAL TESTS�LUNG VOLUME AND DIFFUSING CAPACITY: Helps to characterise severity , but not essential to patient management.

TREATMENT OF ACUTE EXACERBATION �PHARMOCOLOGICAL THERAPY �NON-INVASIVE VENTILATION AND �INVASIVE VENTILATION
 –Salbutamol. -Terbutaline ü Long-Acting")
PHARMOCOLOGICAL: �Beta 2 agonists: ü Short- Acting Beta 2 Agonists(SABA) –Salbutamol. -Terbutaline ü Long-Acting Beta 2 Agonists(LABA) – Formoterol, Salmeterol, Indacaterol, Vilanterol ü Inj. Salbutamol 1. 25 mg and ipratropium bromide 500 mcg/kg 8 th hrly.
Ipratropium, Oxitropium ü Long Acting Muscarinic Antagonist(LAMA)Tiotropium, glycopyronnium etc…")
�Anticholinergics: ü Short Acting Muscarinic Antagonist(SAMA)Ipratropium, Oxitropium ü Long Acting Muscarinic Antagonist(LAMA)Tiotropium, glycopyronnium etc… Inj. Budesonide 0. 5 mg 12 th hrly

�SABA and SAMA – for short term use in acute cases �LABA and LAMA – for maintenance therapy

ADVANTAGES OF NIV �Decreases the need for invasive ventilation and may be associated with improved outcome. �Reduces the work of breathing during weaning and during sleep. �Lower rate of treatment failure and lowers mortality. �Reduced iatrogenic complications. �Reduced length of hospital stay.

INDICATIONS OF NIV �Moderate to severe dyspnea with the use of accessory muscles of respiration and paradoxical breathing. �Moderate to severe acidosis with p. H≤ 7. 35 and Pa. CO 2>45 mm. Hg or Pa. O 2/Fi. O 2<200 �RR >28 breaths/min �Use of accessory muscles of respiration.

PHYSIOLOGY OF NIV �Augmentation of alveolar ventilation to reverse respiratory acidosis and hypercarbia. �Alveolar recruitment and increased Fi. O 2 to reverse hypoxia. �Reduction in WOB to reduce or prevent respiratory muscle insufficiency �Stabilisation of chest wall in presence of chest trauma �Reduction in left ventricular afterload that may lead to improved cardiac function. �Reduction in right ventricular afterload and improved right ventricular function.

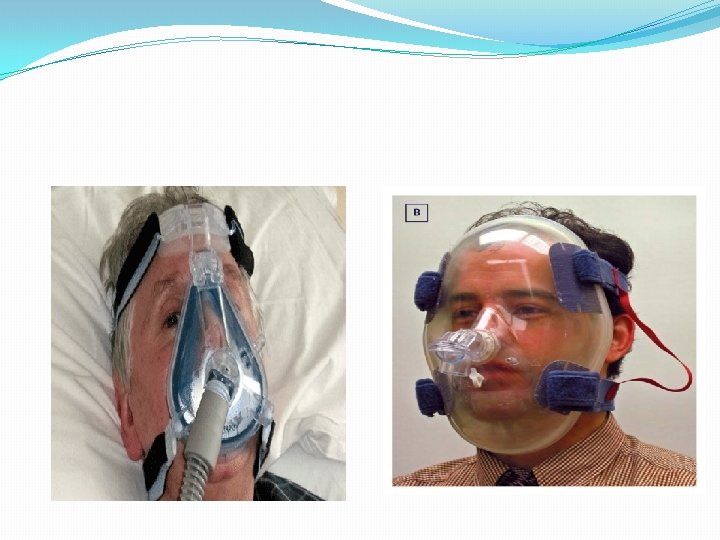
�First and foremost , we need to educate the patient regarding the mask fitness and how it helps in breathing. �To gain confidence and compliance in the patient. �Initiate with low pressure and gradually increase acc. to the individual requirement.

PREREQUISITES FOR NIV �Patient should be conscious, alert, �Haemodynamically stable.

�Commonly described NIV modes are, ü CPAP- Continuous positive airway pressure ü BIPAP- Bilevel / biphasic positive airway pressure ü Pressure or volume limited- intermittent PPV ü High frequency assist ventilation etc…

SETTING AN NIV �EPAP ü Provides PEEP ü Increases functional residual capacity ü Reduces Fi. O 2 required to optimise saturation �IPAP ü Decreases WOB and Oxygen demand ü Increases spontaneous TV ü Decreases spontaneous RR

SIDE EFFECTS OF NIV �Patient discomfort, intolerance �Facial or ocular abrasions �Nasal congestion, sinus pain �Gastric distension

CONTRAINDICATIONS FOR NIV ABSOLUTE �Decreased level of consciousness �Immediate need of endotracheal intubation �Past facial surgery precluding mass fitting �Excess secretions and risk of aspiration and vomiting RELATIVE �Hemodynamic instability �Poor pt. compliance �Severe hypoxia or hypercarbia, Pa. O 2/Fi. O 2 ratio <200 �Lack of trained staff

INDICATIONS FOR INVASIVE VENTILATION �Life threatening Hypoxemia Pa. O 2<40 mm. Hg �Severe Acidosis (p. H<7. 25) and hypercapnia(pa. CO 2>60 mm. Hg) �Respiratory arrest �RR >35/min �Altered mental status �Cardio vascular instability �NIV failure

GOALS OF IMV �To support ventilation , �To allow respiratory muscle to rest, �To minimise dynamic hyperinflation. Ø patients requiring low level support may be commenced on 8 -15 cm H 2 O pressure support, with 3 -8 cm H 2 O PEEP. Ø Patients who are completely exhausted, post arrest, comatose or not tolerating PS , should be commenced on SIMV /ACMV mode.

VENTILATORY SETTINGS: �Pressure or volume ventilation per individual or institutional bias �Avoid Air trapping, ü inspiratory time – 0. 8 -1. 2 sec (high flow) ü RR- 12 -15 breaths/min expiratory ü TV- 6 -8 ml/kg �Pplat < 30 cm H 2 O �PEEP ü Counter-balance Auto-PEEP ü Avoid over- distension �Fi. O 2 - Adequate to maintain spo 2 88 -92%

DYNAMIC HYPERINFLATION �Is the further increase in hyperinflation due to slow expiratory airflow , not allowing completion of expiration before the arrival of next breath. It must be avoided , ü By using low minute ventilation- 115/ml/kg ü By allowing adequate time for expiration. ü By using low TV (8 ml/kg) and ventilator rate <14/min.

HOW TO ASSESS DHI ? ? ? �Clinically by visualising the expiratory flow-time curve and by measuring plateau airway pressure (Pplat) or PEEP. �Pplat should be measured by applying an endinspiratory pause of 0. 5 sec. �This should be applied only following a single breath as it shortens expiratory time and if it is applied to a series of breaths it increases DHI. �If Pplat is >25 cm H 2 O, it is likely to be excessive DHI and the ventilator rate should be reduced.

�PEEPi , measured as a prolonged end-expiratory pause more directly assesses DHI, as PEEPi rises above 8 -10 cm. H 2 O, further prolongation of expiratory time must be considered. �High inspiratory flow rate is recommended as it results in a shorter inspiratory time and hence a longer expiratory time for a given rate.

COMPLICATIONS OF IMV �Equipment: ü Malfunction / Disconnection ü Incorrectly set or prescribed ü Contamination. �Pulmonary : ü Airway intubation ü VAP ü VALI ü O 2 toxicity ü Overt barotrauma

�Circulation : ü Decreased RV preload- decreased CO ü Increased RV afterload ü Decreased splanchnic blood flow with high level of PEEP or mean peak airway pressures ü Increased intracranial pressures with high level of PEEP or mean peak airway pressures ü Fluid retention due to low CO and low renal blood flow.
. ü Mucosal ulceration and bleeding. ü Peripheral")
�Others : ü Gut distension(air swallowing, hypomotility). ü Mucosal ulceration and bleeding. ü Peripheral and respiratory muscle weakness. ü Sleep disturbance, agitation and fear. ü Neuropsychiatric complications.

�Noninvasive positive pressure ventilation improves respiratory acidosis and decreases respiratory rate, breathlessness, need for intubation, mortality, and length of hospital stay. �Inhaled bronchodilators (beta agonists, with or without anticholinergics) relieve dyspnea and improve exercise tolerance in patients with COPD.

�Short courses of systemic corticosteroids in patients with COPD increase the time to subsequent exacerbation, decrease the rate of treatment failure, shorten hospital stays, and improve FEV 1 and hypoxemia. � Low-dosage corticosteroid regimens are not inferior to high-dosage regimens in decreasing the risk of treatment failure in patients with COPD.

�Oral prednisolone is equivalent to intravenous prednisolone in decreasing the risk of treatment failure in patients with COPD. �Antibiotics should be used in patients with moderate or severe COPD exacerbations, especially if there is increased sputum purulence or the need for hospitalization.

�The choice of antibiotic in patients with COPD should be guided by symptoms (e. g. , presence of purulent sputum), recent antibiotic use, and local microbial resistance patterns. �Smoking cessation reduces mortality and future exacerbations in patients with COPD. �Long-term oxygen therapy decreases the risk of hospitalization and shortens hospital stays in severely ill patients with COPD.

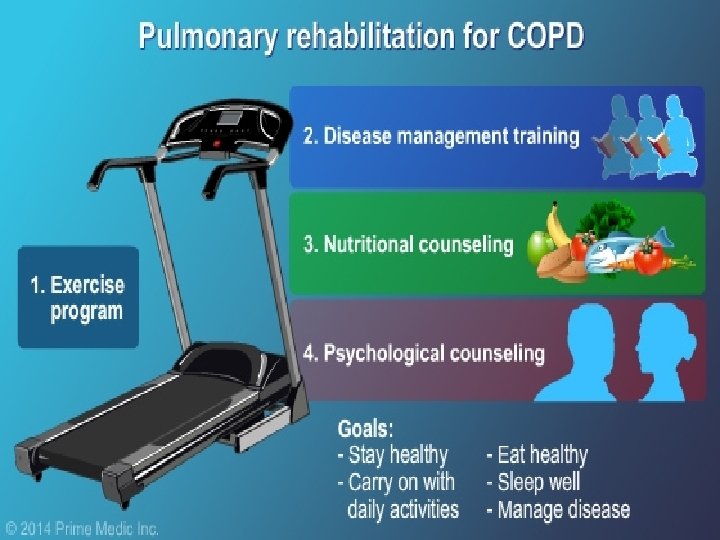
REHABILITATION �Pulmonary rehabilitation �Patient education �Vaccination: Annual influenza and 5 -yrly pneumococcal is recommended. �Exercise �Nutritional counselling �Psychological counselling �Lung transplantation.



- Slides: 56