Management and Care of Dengue with Bleeding Dr

Management and Care of Dengue with Bleeding Dr. Bahariah binti Khalid Head Unit Internal Medicine & Clinical Hematology Faculty of Medicine and Health Sciences Universiti Putra Malaysia

2

3

4

Outline 1. Overt and Assumptions of bleeding 2. Points to be emphasized to the team dealing with bleeding dengue 3. Dilemmas of blood product transfusion in bleeding dengue 4. Challenges that clinicians have to expect because it is real.

Table 2. Clinical symptoms experienced by study population. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

Table 1. Demographics of study cohort. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

Table 2. Clinical symptoms experienced by study population. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

Table 3. Liver enzyme profile of study population. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

FBC in DHF n High hematocrit n Low white blood cells count n Low absolute neutrophils n High absolute lymphocytes n High atypical lymphocytes n Low platelets n Slightly prolonged PT and APTT n Slightly prolonged or normalized thrombin time

Table 4. Blood and white blood cells profile of study population. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

Table 5. Laboratory diagnostic assay results in the study cohort. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215

Table 7. Association of cytokines with clinical parameters in the study cohort. Rathakrishnan A, Wang SM, Hu Y, Khan AM, et al. (2012) Cytokine Expression Profile of Dengue Patients at Different Phases of Illness. PLo. S ONE 7(12): e 52215. doi: 10. 1371/journal. pone. 0052215 http: //www. plosone. org/article/info: doi/10. 1371/journal. pone. 0052215
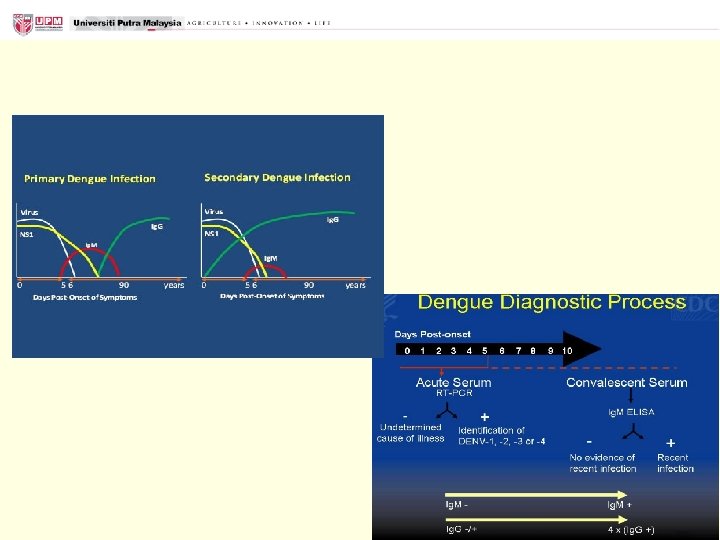

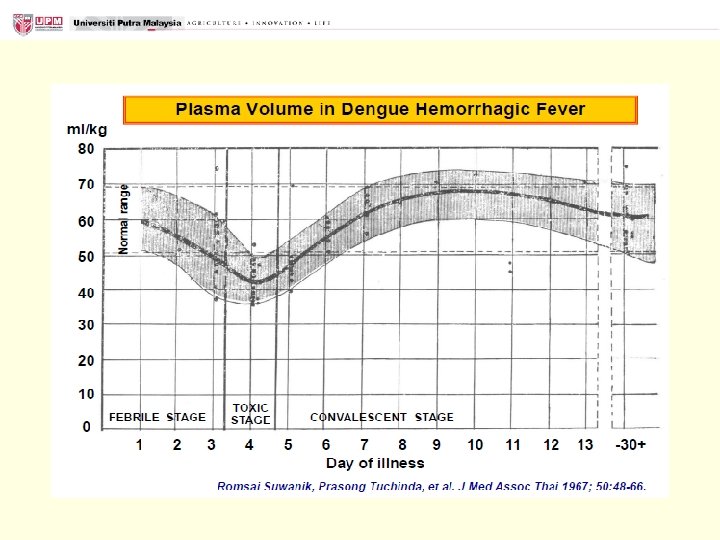
Plasma leakage
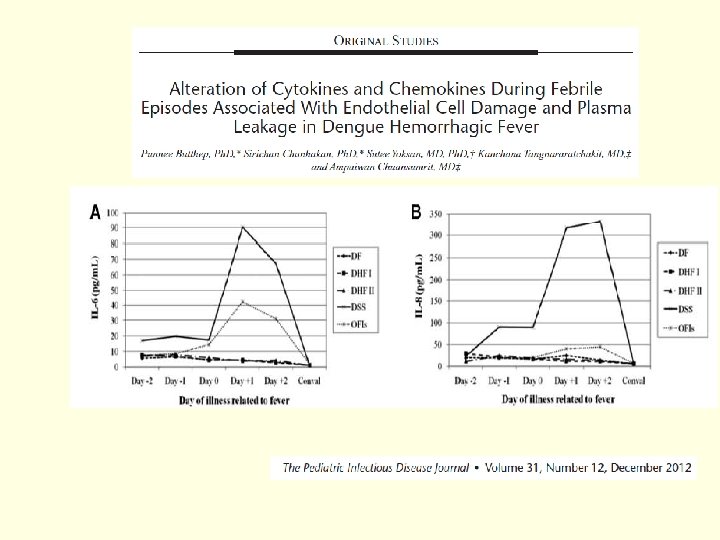
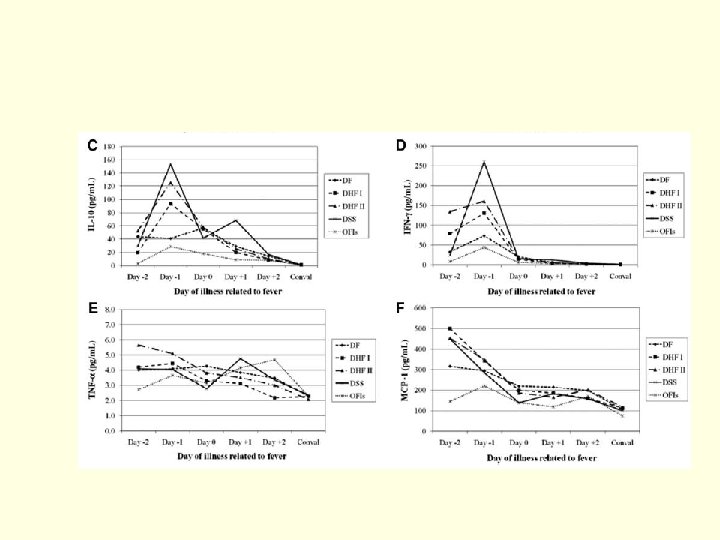

The cause of bleeding Dengue it is hemostasis defect

Overt and Assumptions of bleeding 1. Understanding haemostasis 2. Take a good bleeding history 3. Understand the possible causes for deranged coagulation profiles 4. Investigate the cause of a significant bleeding history and prolonged clotting times 5. Managing coagulopathy

Overt and Assumptions of bleeding n Immediate bleeding n Defects in primary haemostasis n - low platelets, CVC n Vascular abnormality n -capillary leak, procedures n Delayed bleeding n Defects in secondary haemostasis

Dengue infection can lead to disseminated intravascular coagulation. A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

23

Massive transfusions can lead to disseminated intravascular coagulation. A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

25

A good bleeding history is the best screening tool.

Parameters to indicate risk of bleeding in general…but in dengue? Age > 85 Active gastroduodenal ulcer Bleeding in 3 months before admission Central Venous Line insertion Current cancer Hepatic failure ( INR 1. 5 ) ICU / CCU admission Male sex Platelet count < 50 x 10˄9/L Rheumatic disease Severe renal failure (GFR , 30 m. L/min/m²)

WHO Bleeding Grades Grade 0, none Grade 1, petechiae, ecchymosis, occult blood in body secretions, and mild vaginal spotting n Grade 2, evidence of gross hemorrhage not requiring red cell transfusions over routine transfusion needs (e. g. epistaxis, hematuria, hematemesis) n Grade 3, hemorrhage requiring transfusion of 1 or more units of red cells/day n Grade 4, life-threatening hemorrhage, defined as massive bleeding causing hemodynamic compromise or bleeding into a vital organ (e. g. , intracranial, pericardial, or pulmonary hemorrhage) n n Tail it to your individual patient

A significant bleeding history n Epistaxis not stopped by 10 mins compression or requiring medical attention n Cutaneous haemorrhage or bruising without apparent trauma (esp. multiple/ large) n Prolonged (>15 mins) bleeding from trivial wounds, or in oral cavity or recurring spontaneously within 7 days n Post-operative bleeding n Menorrhagia (esp. from menarche)

Bleeding in the hospitalized patient n Bleeding prolonged, delayed or recurrent; or more rapid than normal? n Single site or several sites? n Appropriate to injury? n Past h/o bleeding? n Medications? n Diseases? n Family history?

Case n 35/M/lady D 5 of fever admitted DSS with AKI on Noradrenaline. n She was covered with broad spectrum antibiotics. n Her GCS and saturation dropped that she requires ventilatory support and admitted to ICU. CT brain shows no ICB. n 3 hours later she had bleeding from the oral cavity and nose but no other bleeding elsewhere. The suction tube measured 1 L. n Hb 10. 1 HCT 37 TWC 6. 9 Plt 32 Pt 14 APTT 50

Will you request Sr. Fibrinogen for this patient? A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

33

Should DIVC regime be given? A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

35

There is no FIXED DIVC regime

Outline 1. Overt and Assumptions of bleeding 2. Points to be emphasized to the team dealing with bleeding dengue 3. Dilemmas of blood product transfusion in bleeding dengue 4. Challenges that clinicians have to expect because it is real.

In critical care medicine

In critical care medicine

Case n 35/M/lady D 5 of fever admitted DSS with AKI on Noradrenaline. n She was covered with broad spectrum antibiotics. n At 36 hours of defervescence, her GCS and saturation dropped that n n she requires ventilatory support and admitted to ICU. CT brain shows no ICB. 3 hours later she had bleeding from the oral cavity and nose but no other bleeding elsewhere. The suction tube measured 1 L. Hb 10. 1 HCT 37 TWC 6. 9 Plt 32 Pt 14 APTT 50 Other parameters were normal The volume partly because of the suction water for irrigation

Does this patient needs blood product transfusion? A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

43

Are prophylactic platelet transfusions necessary? n Unresolved issue n Should we give it before bleeding or only with the onset of active bleeding? n Might be safe in a select group of patients
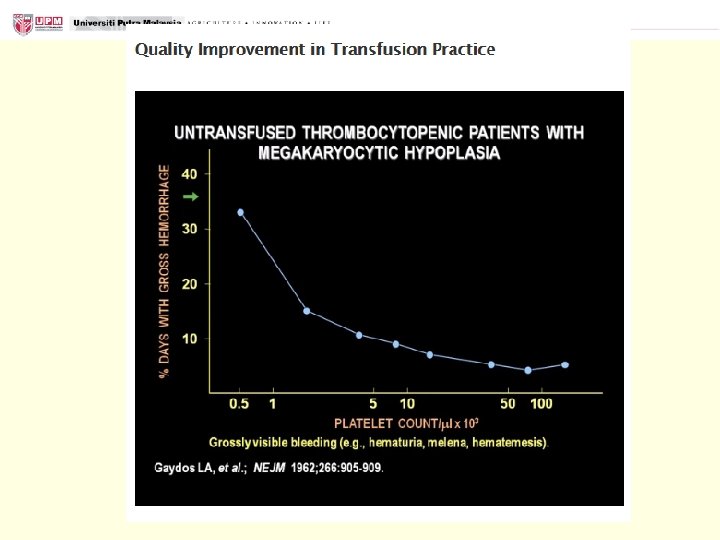

Platelet Transfusion n At least 7. 1 x 109 platelets/L are consumed daily in endothelial support functions n The equivalent of approximately one Random Donor Platelet daily for a 70 kg adult with marrow failure Kerok Petecheal hemorrhages Purpura fulminans

Therapeutic Platelet Transfusion n Platelet transfusion is usually needed when WHO bleeding grade 2 or more n Grade 3 or 4 Bleeding is usually associated with other factors (not low platelets alone) Uraemia n Drugs n Ulcers n Bleeding tumours n
: ○ Collected from whole blood ○ Expected")
Platelets : 2 types Random blood donor(RDP): ○ Collected from whole blood ○ Expected increment per unit: 5 -7 x 109/L ○ Should contain ≥ 5. 5 x 1010 platelets (average content Single donor apheresis(SDP): ○ Collected from apheresis by automated instrumentation ○ Expected increment per unit: 30 - 50 x 109/L ○ Should contain ≥ 3. 0 x 1011 approximately 8. 0 x 1010) per platelets (average content bag in approximately 50 m. L approximately 3. 5 -4. 0 x 1011) of plasma. per bag in about 250 m. L of plasma

Judiciously RDP Advantage- ? Disadvantage- exposure to many donor viral and bacterial transmission, many donor allosensitization SDP Advantage- single donor exposure Disadvantage- expensive – RM 300, more volume (equivalent to 4 -6 random donor)

Response n Measure platelet count from 10 minutes to 3 hours after transfusion. n Generally, expect an adult platelet count increment of approximately 7 -10, 000/ mm 3 for each RDP given, or 30 -60, 000/ mm 3 for each SDP given.

Indication n Use to treat bleeding due to critically decreased circulating platelet counts or functionally abnormal platelets. n Use prophylactically to prevent bleeding at prespecified low platelet counts. n Maintain platelet count n n n >10, 000/mm 3 in stable, non-bleeding patients, >20, 000/mm 3 in unstable non-bleeding patients and >50, 000/mm 3 in patients undergoing invasive procedures or actively bleeding.

Platelets is contraindicated in Immune-mediated platelet destruction n HIT/ITP- Such use is usually reserved for situations of potentially life-threatening haemorrhage Thrombotic thrombocytopenic purpura/haemolytic uraemic syndrome n Transfusion of platelets has been accompanied by acute deterioration n Still allowable for large bore cannulation
 n Plasma consists of the noncellular portion of blood that")
Fresh Frozen Plasma (FFP) n Plasma consists of the noncellular portion of blood that is separated and frozen after donation prepared from whole blood or collected by apheresis n Stored at – 30°C n Plasma frozen within 8 hours is called fresh frozen plasma (FFP) n 1 unit FFP (150 – 300 ml), will increase each clotting factor activity by 2 -3%

Indications Frozen Plasma is indicated for use in patients with the following conditions: 1. Active bleeding due to deficiency of multiple coagulation factors, or risk of bleeding due to deficiency of multiple coagulation factors. 2. Severe bleeding due to warfarin therapy, or urgent reversal of warfarin effect 3. Massive transfusion with coagulopathic bleeding. 4. Bleeding or prophylaxis of bleeding for a known single coagulation factor deficiency for which no concentrate is available. 5. Thrombotic thrombocytopenic purpura. 6. Rare specific plasma protein deficiencies, such as C 1 -inhibitor.

and contraindications of FFP n Frozen Plasma should not be used for 1. Increasing blood volume or albumin concentration 2. Coagulopathy that can be corrected with administration of Vitamin K. 3. Normalizing abnormal coagulation screen results, in the absence of bleeding.

Dosing n Determined by the patient size and clinical condition. n For correction multiple coagulation factor deficiencies, plasma transfusion should be guided by coagulation testing. n Therapeutic or prophylactic replacement n PT > 1. 5 times the mid-range of normal n APTT > 1. 5 times the top of the normal range n or factor assay less than 25% in an appropriate clinical setting. n If testing not readily available, use clinical evidence of bleeding for transfusion decisions. n Dosing guide n achieve a minimum of 30% of plasma factor concentration eg. 10 -20 m. L/kg, though more may be required depending upon the clinical situation. n 12– 15 ml/kg (usually about 3 -6 units) in would typically increase fibrinogen levels by about 1 g/l

Lactate >5, I would choose whole blood to be transfused? A. Disagree B. Disagree Somewhat C. Neutral D. Agree Somewhat E. Agree

58

Whole blood n Massive transfusion guideline n Short Screening at least 2 days as PDN are tight at infective screening. n More likely for allosensitization as they have more Lymphocytes n High 2, 3, DPG n Equivalent to 1 FFP, 1 unit RDP, 1 pint PC

Transfusion reactions

Outline 1. Overt and Assumptions of bleeding 2. Points to be emphasized to the team dealing with bleeding dengue 3. Dilemmas of blood product transfusion in bleeding dengue 4. Challenges that clinicians have to expect because it is real.

Dengue fever are taught as mostly not septic looking. n Can this cause late in instituting treatment for sepsis thus high mortality? n Survival Sepsis guideline has transfusion guideline that helps just as a guide. 63

Is dengue Sepsis? n No studies on prevalence of dengue with concomitant sepsis. n Viraemia in the first 3 -5 days (old school considered as sepsis) n Later part is the ADE responses n Latest school- Sepsis is meant for BACTERIAL only 64

Outline 1. Overt and Assumptions of bleeding 2. Points to be emphasized to the team dealing with bleeding dengue 3. Dilemmas of blood product transfusion in bleeding dengue 4. Challenges that clinicians have to expect because it is real.

Dengue in challenging population n Foreigners and disabled-language barrier n Concomittant other infections n Dengue patients warfarinized or on NOAC n Pregnancy and postpartum n Obese n Elderly n Post vaccination n Transfusion reactions n Early institution of VTE prophylaxis in high risk of thrombosis

Conclusion n Difficult bleeding dengue is a challenge and it can happen at all ages and it is due to defect in hemostasis n Emphasize should be made to identify dengue population at risk of bleeding and the bleeding sites as early when the patient is suspected to have dengue infection n Stop the bleeding or advise the managing team accordingly to what is watchful expectation.

Conclusion n Avoid hypothermia, hemodilution/overload, acidosis and prolonged unsolved bleeding at all times as it affects the poor function of the coagulation factors. n Find the alternative if failing the conventional treatment but remember it is not without side effects.
- Slides: 69